Elderly Midterm
1/142
Earn XP
Description and Tags
Y r u gey
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
143 Terms
Be able to compare and contrast the theories of aging
For each of the following, state the core concept of the theory and the reasoning behind each
Mitochondrial aging theory (Role of energy production and associations with aging)
Developmental genetic theories (Core concept and aging as a continuum)
Stochastic theories (Core concept and mechanism)
Newer theories: evolving ideals in aging research (Sleep and aging, telomere theory)
Mitochondrial Aging Theory
a. Role of Energy Production (ATP): As mitochondria become damaged over time, ATP production decreases.
b. Associations with Aging: Mitochondrial decline results in less energy for cell maintenance and repair, accelerating aging.
Developmental Genetic Theories
a. Core Concept: Aging is a genetically programmed process. Genes that regulate growth and development may also control lifespan.
b. Aging as a Continuum: Aging is not separate from development; it's part of a continuous, genetically regulated timeline, much like puberty or menopause.
Stochastic Theories
a. Core Concept: Aging results from random environmental damage (pollution, food quality, pesticides) to cells and molecules (DNA, proteins, lipids) over time.
b. Mechanism: Environmental stressors like radiation, toxins, and ROS cause damage that accumulates and impairs cellular function.
Newer Theories: Evolving Ideas in Aging Research
a. Sleep and Aging: Poor sleep quality is associated with accelerated aging and neurodegeneration.
b. Telomere Theory: Telomeres (chromosome end caps) shorten with each cell division. When critically short, they trigger cell senescence or death.
Be able to describe the normal physiological changes associated with aging
What can be seen visually (appearance) ?
In terms of thermoregulation?
Musculoskeletal changes?
Skin changes?
Cardiovascular changes?
Pulmonary changes?
Neurological changes?
Gait changes in older adults?
Immune function?
Intersystem homeostasis?
Hormonal changes?
Gastrointestinal changes?
Renal and urinary changes?
Sensory changes (For hearing, vestibular and proprioception, taste and smell, and vision)?
Appearance
Gray hair, skins changes, tooth color, posture, movement, body composition
Thermoregulation
Hypothermia Risks: slower metabolism, decreased body fat, poor nutrition, impaired ability to perceive the cold (dementia)
Hyperthermia Risks: decreased sweating, chronic illness, meds, dehydration
Prevention is key!
Musculoskeletal Changes
Cartilage: decreased hydration & elasticity, reduced elasticity
Muscle: less type II fibers, sarcopenia, decreased strength and muscle mass
Bone: decrease in calcium, vitamin D, bone strength, increased fracture risk
Organ shrinkage is one of the main reasons why mortality increases in MVA involving older adults. Think of a smaller brain moving within the skull, causing a terrible whiplash
Skin Changes
Slower healing, less able to resist injury and infection
Sweat and sebum glands as well as sensors and hair follicles atrophy
Think of the fat pads that cover the veins and tendons of our hands and feet. Older adults lose this fat pad, so they are essentially walking on “skin and bones”
Cardiovascular Changes
Increased BP, decreased HR max, decreased VO₂ max, stiffer vessels
Decreased response to stress, decreased ventricular compliance
Loss of cells from the SA node (pace maker needed)
A pulse pressure over 60 is indicative of a future cardiac event!
Pulmonary Changes
Decreased chest wall compliance & elastic recoil
Decreased intercostal/diaphragm/abdominal strength
Decreased vital capacity, increased residual volume (lungs are overinflated)
Neurological Changes
Decrease in neurons, decreased conduction velocity, decreased blood flow
Decrease in sensory neurons, slower response time
Decreased encoding and retrieval with age (learning issues)
Plaques and tangles noted in neurons
Memory loss that does not impair social or personal functioning
Gait Changes in Older Adults
Decreased speed, decreased step length, increased stance time
Increased gait variability, decreased joint excursion
Decreased ankle power, more stooped posture
Immune Function
Decreased infection defense, more prone to autoimmune disorders
Increased systemic inflammation (what helps: anti-inflammatory drugs, antioxidants, caloric restriction, exercise)
Intersystem Homeostasis
Decreased thermoregulation, decreased basal metabolic rate, decreased hormonal regulation, ANS dysfunction, decreased BP to the brain
Hormonal Changes
Decreased insulin, testosterone, estrogen
Considerations for hormone replacement
Gastrointestinal & Hepatic Changes
Decreased motility, decreased nutrient absorption
B12 deficiency: Lack of intrinsic factor reduces absorption in the stomach, so sublingual pills tend to be used often to bypass the stomach
Gallbladder: increased gallstones
Liver: decreased function, increased fat accumulation
Renal & Urinary Changes
Decreased kidney mass, decrease in nephrons, decreased blood flow
Increased nocturia, residual urine, UTI risk, incontinence
Sensory Changes: Hearing
Presbycusis: decreased high-frequency hearing
Decreased auditory receptors, TM changes
Sensory Changes: Vestibular & Proprioception
Decreased otolith function, decreased proprioceptive input
Sensory Changes: Taste & Smell
Decrease in taste buds, decreased saliva, decreased olfactory bulb cells
Sensory Changes: Vision
Decreased tear production, decreased lens flexibility (presbyopia)
What are the keys to successful aging? (3)
Avoiding Disease: chronic illnesses and their complications
Maintaining High Cognitive and Physical Function: the ability to think clearly and move independently
Engagement with Life: staying socially and productively involved
How does sleep architecture change with aging?
Sleep Latency
Increased time to fall asleep
Deep Sleep Decline (Slow-Wave Sleep)
Decreased time spent in deep sleep (Stages 3 & 4)
Less restorative sleep contributes to feeling unrefreshed
REM Sleep Decline
May affect memory consolidation and emotional regulation
Increased Sleep Fragmentation
Nighttime awakenings and lighter sleep
Breathing-Related Disruptions
Snoring and sleep apnea cause arousals
Increased Sleep Disorders
Insomnia, obstructive sleep apnea, restless legs syndrome, and gastroesophageal reflux disease
Decreased Sleep Satisfaction
More daytime fatigue
Medical and Medication Effects
Physical and psychiatric conditions (pain, depression) and medications (beta-blockers, diuretics, antidepressants)
Circadian Rhythm Changes
Shift toward earlier sleep and wake times ("advanced sleep phase")
Phase Advance Syndrome
Rhythm is shifted so that the older adult falls asleep early in the evening but then wakes up very early in the morning while still obtaining the same 7 or 8 hours of sleep
Light exposure may be a helpful treatment
How can we promote improved sleep hygiene with our older patients, while maintaining safety?
Establish a consistent?
Create what type of environment?
Limit what two things?
Monitor intake of what?
Establish a Consistent Sleep Schedule
Create a Sleep-Conducive Environment: Quiet, cool, dark bedroom; remove noise or light distractions. Use nightlights to prevent falls
Limit Naps: If needed, nap early in the day and keep it under 30 minutes.
Limit Screen Time Before Bed: Blue light suppresses melatonin production.
Monitor Caffeine, Alcohol, and Fluids: Reduce fluid intake 1 to 2 hours before bed to avoid bathroom-related falls.
How do nutritional components and exercise relate to brain health and the prevention of Alzheimer’s?
What type of diet is ideal for Alzheimer prevention? What diet combines two (and what diets does it combine)?
What supports neuronal membrane integrity and reduces brain inflammation?
What do antioxidants do?
B vitamins lower ______ levels. Higher ______ levels are associated with?
Low levels of vitamin ___ are associated with cognitive decline
Exercise and brain health promotes/improves what things?
Increases what factor? This factor helps with?
Mediterranean Diets → Leafy greens, berries, whole grains, nuts, fish, olive oil
MIND Diet: Combination of Mediterranean and DASH (diuretic)
Omega-3 Fatty Acids → Fatty fish (salmon, sardines), flaxseed
Supports neuronal membrane integrity and reduces brain inflammation.
Antioxidants → Berries, dark chocolate, green tea, leafy greens
Counteract oxidative stress that damages brain cells.
B Vitamins (B6, B12, folate) → Whole grains, legumes, leafy greens, eggs
Lower homocysteine levels (high levels are linked to brain atrophy)
Vitamin D → Low levels are associated with cognitive decline
Exercise & Brain Health → promotes neuroplasticity, improves sleep and mood, enhances blood flow to the brain
Increases Brain-derived Neurotrophic Factor (BDNF): supports the survival of neurons and the growth of new brain cells, particularly in the hippocampus (key for memory)
Reduces Risk Factors: diabetes, obesity, hypertension, and depression
How can patients keep their cognitive abilities sharp?
Stay Mentally Active: Learn a new skill or hobby, do puzzles, crosswords, Sudoku, or brain training apps, read books or listen to informative podcasts
Stay Physically Active: Improves blood flow to the brain and supports memory
Stay Socially Engaged: Join clubs, volunteer, or attend classes
Neurobic Activities (brain-stimulating activities designed to build new neural pathways by breaking your everyday routines and engaging multiple senses simultaneously)
What would be considered neurobic activities?
What are neurobic activites? How does it work? Examples?
Neurobic activities are non-routine tasks that engage the brain in novel, multisensory, and emotionally engaging ways.
Stimulate different neural pathways, enhancing brain flexibility and memory.
Brush your teeth with your non-dominant hand
Listen to music you don’t normally hear
Eat with chopsticks if you usually don’t
Describe nutritional issues related to older adults.
What is the connection of various nutrients related to conditions associated with aging?
What two vitamins are good for older adults and why? Deficency risks?
Vitamin D
Enhances calcium absorption in the gut and regulates bone turnover
Older adults often have lower sun exposure and decreased skin synthesis, leading to vitamin D deficiency
Deficiency Risks: Increased bone loss, fractures, falls, and muscle weakness
Calcium
A key mineral for bone structure and strength
Intestinal absorption decreases with age
Deficiency Risks: Accelerated bone loss and osteoporosis
How does protein relate to sarcopenia?
What sort of resistance do older adults have? How does protein intake relate to this?
Anabolic Resistance
Older adults have anabolic resistance, meaning their muscles are less responsive to protein intake
Higher protein intake is needed to stimulate muscle maintenance
Sarcopenia
Age-related loss of skeletal muscle mass and function
Protein
Provides the amino acids necessary for muscle protein synthesis
What are the Blue Zones’ 9 Lessons for Living Longer?
What are the areas of the “blue zone”?
Blue Zone Principles
Move Naturally: Be active without having to think about it
Hara Hachi Bu: Stop eating when you are 80 percent full
Plant Slant: Avoid meat and processed foods
Grapes of Life: Drink red wine in moderation
Purpose Now: Take time to see the big picture
Downshift: Take time to relieve stress
Belong: Participate in a spiritual community
Loved Ones First: Make family a priority
Right Tribe: Be surrounded by those who share Blue Zone values
Moving Hara Plants Grapes Purposefully Down Below Love Tribe
Areas of the “Blue Zone”
Loma Linda, California
Sardinia, Italy
Icaria, Greece
Okinawa, Japan
Nicoya, Costa Rica
Lomo Saltado Is Outstanding Naturally.
How can the physical therapist use the Mini-Nutritional Assessment to evaluate a patient?
What age is this usually done for?
What are the normative values?
Nutritional Risk Assessment
Evaluate nutritional risk in older adults (usually age 65+). It helps identify malnutrition or risk of malnutrition
Malnutrition impacts muscle mass, bone health, wound healing, and immune function
Addressing nutrition can enhance therapy outcomes, promote independence, and reduce hospital readmissions
Scoring
Normal = 12-14 points
At risk = 8-11 points
Malnourished = 0-7 points
Be able to design an appropriate exercise prescription for an older adult.
Aerobic, including HIIT
150 min / aerobic a week
Prolonged warm up & cool down to prevent arrhythmias
Balance (for fall prevention)
Range of Motion and Flexibility (Static and Dynamic Stretching)
For fall prevention
Static stretching for 30s: optimal to increase ROM and minimize the negative effects on the neural function of involved nerve roots
Strength, Muscle Endurance, Power, Key Muscle Groups, Plyometrics
2-3x per week
1 set of 8-12 reps major muscle groups
Posture
Aquatics
Should not wear paddles or webbed gloves
Fins are okay on LE as long as they have no severe weakness or pain
Snorkel is good for cervical ROM
How does the exercise prescription relate to functional activities?
Exercise targets specific deficits to improve daily function
Sit-to-stand → squat strength for transfers
OH press → reaching activities
How can the exercise program be advanced? Modified based on a case scenario?
Progress by increasing intensity, complexity, or duration.
Modify based on pain, fatigue, or impairments
Be able to apply the FITTE formula, including all elements of an exercise prescription.
F - How many days a week?
I - Min, mod, or max intensity?
T - How many minutes a week of aerobic activity?
T - What types of exercise are ideal?
E - What would boost adherence?
Frequency (3 to 5x/week)
Intensity (moderate)
Time (≥150 min/week aerobic)
Type (aerobic, strength, flexibility)
Enjoyment (individual preference boosts adherence)
Be able to apply the CDC Older Adult Physical Activity guidelines to a patient case scenario
How many minutes a week and what intensity for aerobic activity?
How many days a week of strength training and how many reps per activity?
What type of training for fall prevention? Give some examples. What muscle groups can be strengthened to also improve fall prevention?
150 min/week moderate aerobic activity
2+ days/week of strength training
8 to 12 repetitions per activity
Balance training for fall prevention
Walking backward, standing on one leg, or using a wobble board are examples of balance activities
Strengthening back, abdomen, and leg muscles also improves balance
Calculate exercise heart rates, including the Karvonen formula
What is the Karvonen formula? What is the formula for HRmax? What intensity range is ideal?
• THR = [(HRmax − HRrest) × %Intensity] + HRrest
• HRmax = 220 – age
• Use 50–85% intensity range
Prescribe appropriate resistance training parameters
How many sets, how many reps, and how many times per week?
2 to 3 sets, 8 to 12 reps, 2 times per week
What is aquatic heart rate reduction? How is it found? Target heart rate for land and aquatic?
How does hydrostatic pressure help?
How does buoyancy help?
How does thermal conductivity help?
physiological phenomenon where your heart rate is typically 10 to 17 beats per minute lower in water than during land-based exercise
Subtract 10 to 17 bpm from land-based target HR due to hydrostatic pressure and cooling effect
Land Target HR = 130 bpm
Aquatic Target HR = 115–120 bpm
Hydrostatic Pressure
Water pressure helps circulate blood more efficiently
The heart doesn't have to work as hard to return blood to the heart
Buoyancy
Reduces gravitational stress → less effort from muscles and heart
Thermal Conductivity
Water removes heat from the body faster, keeping the cardiovascular system cooler and reducing HR
Prescribe a stretching program for an older adult. How long to hold a static stretch?
Hold static stretches 30 seconds
How are the different types of muscle contractions related to function and exercise prescription?
(Not on Ashleys, general chat GBT answer here)
Concentric (muscle shortens) – helps with movements like standing up from a chair or climbing stairs.
Eccentric (muscle lengthens) – helps control movement, such as sitting down slowly or walking downhill; important for balance and fall prevention.
Isometric (muscle contracts without movement) – helps improve stability and maintain strength when joint movement is limited.
How do specific types of contractions and motor learning relate to an exercise program?
Concentric and eccentric: Which one is shortening which one is lengthening? What does concentric improve vs eccentric?
The gait cycle is about __% eccentric or concentric contractions?
What is Isometric? What does it help improve?
Use for what muscles?
What is the cognitive stage, associative stage, and autonomous stage when it comes to learning a movement?
Concentric
Shortening → Strength building
Eccentric
Lengthening → Improves control, reduces injury risk, helps with balance and shock absorption
Gait cycle is about 60% eccentric contractions!
Isometric
No movement → Builds joint stability, useful when joint movement is painful or restricted
Use for trunk muscles!
Cognitive Stage: Patient is learning the "what and how", needs more verbal/visual feedback
Associative Stage: Patient refines movements, fewer errors, improved coordination
Autonomous Stage: Movements become automatic, less conscious thought, functional carryover
How does The Physical Stress Theory relate to strength training?
Body adapts to the level of stress
More load = more strength
Too little = atrophy
Too much = injury
Be able to prescribe power exercises.
Use ____, ____ movements with what level of load (light moderate or heavy)
Give some example exercises.
Use fast, controlled movements with light or moderate loads
Sit-to-stand with speed, step-ups
How are the concepts of Fun, Function, Frail, and Failure related to the slippery slope of aging?
Aging is a continuum, what can prevent decline?
Explain each of the “F”s.
Aging is a continuum. Exercise prevents decline.
Fun (unrestricted participation)
Function (some limits): may need to modify performance
Frail (assistance needed)
Failure (dependent): may be bedridden
Design an exercise program related to functional movements and key muscle groups.
Nothing on ashleys. Self explanatory really.
How can a physical therapist maximize patient education activities?
Use simple language, visuals, hands-on demos, and repeat key info.
Make it relevant and goal-focused.
Describe how ageism and bias might influence physical therapy care.
One mistake is to assume?
Treat based on what?
What method can be used to bolster positive age beliefs?
Assuming limitations due to age may lead to under-dosing or ignoring goals
Treat based on ability, not age
ABC Method to Bolster Positive Age Beliefs
Awareness: Identifying where negative and positive images of aging are found in society
Blame: Understanding that health and memory problems can be the result, at least in part, of the negative age beliefs we acquire from society
Challenge: Taking action against ageism so that it is no longer harmful
Describe the physiology of aging and normal changes associated with aging
Discussed in previous cards
How do these (age) changes impact functional status?
Decline in?
Decrease ability to preform what activities?
Loss of?
Decline in mobility, balance, and endurance
Increased fall risk and fatigue
Decreased ability to perform ADLs (dressing, bathing, walking)
Loss of independence!
How could these age-related changes influence a patient’s motivation?
Can cause what emotions? This can decrease what and lead to what sort of issues?
Cause frustration, fear, or a sense of dependence
Decrease motivation: “I’m too old to get better”
Lead to depression or apathy, especially with multiple comorbidities
How can a physical therapist strengthen a patient’s motivation?
Set meaningful, achievable goals
Use motivational interviewing and positive reinforcement
Include them! Encourage patient choice and shared decision-making
Celebrate small wins and functional gains
Incorporate social support (family, groups)
How does lifestyle relate to the physiology of aging?
What type of lifestyle slows decline and improves cognition?
A sedentary lifestyle accelerates what? This can lead to?
What are some things that are ideal to know for patient history?
Active lifestyle slows physical decline and promotes cognitive health
Sedentary behavior accelerates loss of function and leads to depression
History of exercise? Exposure to sunlight?
Describe how aging interacts with the various systems of the body (Age related change and functional impact)
Muscular
skeletal
Cardiopulmonary
Pulmonary
Nervous
Sensory
G/Renal
System | Age-Related Change | Functional Impact |
|---|---|---|
Muscular | ↓ Mass & strength | Weakness, ↓ mobility |
Skeletal | ↓ Bone density | ↑ Fracture risk |
Cardiovascular | ↓ Reserve, ↑ BP | ↓ Endurance, ↑ cardiac stress |
Pulmonary | ↓ Elasticity, ↑ RV | ↓ Exercise tolerance |
Nervous | ↓ Reaction time, balance | ↑ Fall risk, ↓ coordination |
Sensory | ↓ Vision, hearing | Difficulty with ADLs, ↑ fall risk |
GI/Renal | ↓ Absorption, ↓ excretion | ↑ Medication sensitivity, constipation |
How would a physical therapist accommodate these age-related changes into treatment?
Should have a thorough screening of what?
Tailor _____. Start low and progress based on?
Use of what devices and why?
Address _____ loss. How?
What training is critical to do due to increased fall risk?
Thorough Screening
Fall risk, strength, endurance, vision/hearing, cognition
Tailor Intensity
Start low, progress based on tolerance (FITTE model)
Use Assistive Devices
For safety and independence
Address Sensory Loss
Speak clearly, use large print, ensure good lighting
Balance Training
Critical due to increased fall risk
What modifications to physical therapy interventions would be necessary?
Longer warm-ups and cool downs
Frequent rest breaks
Simplified instructions, demonstrations
Use of functional tasks (sit-to-stand, step-ups)
Incorporate dual-task or cognitive-motor activities
Hydration and nutrition education when appropriate
What accommodations can be made for an older adult with sensory impairments?
What can be done for the environment?
What assistive technology can help?
Demonstrate exercises and use what method?
Environmental Modifications
Lighting, noise reduction, contrasting colors, clear pathways, adaptive equipment
Assistive Technology
Hearing aids, voice-activated & text-to-speech software
Demonstrate Exercises
Teach back method
Design a marketing brochure or written home exercise program to accommodate older eyes.
Bruh she asking for too much fr (Not on ashley’s)
Distinguish between macular degeneration, cataracts, diabetic retinopathy, and glaucoma.
macular degeneration: Blurriness of central vision.
cataracts: Opacity of the lens reduces visual acuity. Complaints of “glare” from bright lights.

glaucoma: Increased intraocular pressure to the optic nerve that causes a slow loss of visual field

diabetic retinopathy: Damages the blood vessels in the retina, usually complains of floaters or dark spots.

What are eye floaters?
How should the PT respond if the patient described an increase of floaters or a flash of light with the onset of floaters?
Eye floaters: are tiny spots that appear to move within your field of vision.
The PT should refer out → advise the patient to seek prompt medical attention from an ophthalmologist or retina specialist.
How would you assist your patient with vision or hearing loss?
How do these sensory deficits relate to overall patient safety?
What accommodations would be necessary to promote patient function and safety?
Vision Loss
Speak before touching the patient
Use high-contrast colors
Use large-print instructions or verbal explanations
Recommend magnifiers, bright lighting, night lights
Make sure they are wearing their glasses
Hearing Loss
Face the patient so they can read lips or see facial expressions
Speak clearly, not loudly, and at a moderate pace
Use written instructions or visual cues
Reduce background noise
Encourage use of hearing aids and verify if they are working properly
Accommodations to Promote Function and Safety
Visual cues
Assistive technology
Grab bars
Non-slip flooring
Adaptive lighting
Personal emergency response systems
Regular caregiver or family education
What safety considerations would need to be made for a patient with diminished smell or touch?
Diminished Smell (Hyposmia/Anosmia)
Cannot detect smoke, gas leaks, spoiled food
Install visual fire/smoke alarms
Encourage use of electric stoves over gas
Regular food checks for freshness
Diminished Touch (Neuropathy)
Higher risk of burns, pressure injuries, and injuries from falls
Use thermometers for bath water and food
Encourage protective footwear
Perform regular skin checks for injury or breakdown
Pressure-relieving cushions and mattresses
What considerations would be necessary when designing residential facilities or a PT clinic?
Wide, clear hallways and doorways
Non-slip, low-glare flooring
Bright, even lighting without harsh glare
Large-font, easy-to-read signage
Visual and auditory emergency systems
Inclusive design for mobility and sensory impairments
What intrinsic or extrinsic factors would place a patient at risk for falls?
Musculoskeletal
Weakness, decreased range of motion, pain
Cardiopulmonary
Blood pressure issues, decreased oxygenation, heart arrhythmias, limited endurance
Vision
Acuity, depth perception, glare recovery
Balance
Visual, vestibular and somatosensory systems
Medications
Side effects (postural control, cerebral perfusion, and/or cognition) and multiple medications (polypharmacy/ +5)
Environmental Factors
Obstacles, Poor design of home, Inappropriate use of assistive devices, Lack of safety equipment
Diseases
Neurological disorders, Cardiovascular disorders, MSK disorders, Psychological disorders (depression), Visual disorders (glaucoma, cataracts, macular degeneration, diabetic retinopathy), Incontinence
Based upon a patient’s risk factors, design strategies to minimize functional loss
What questions should you be asking?
History of Falls: Have you fallen in the past year
Balance Issues: Do you feel unsteady when standing or walking?
Fear & Trauma: Do you worry about falling?
Be familiar with the ICF model, especially as related to fall prevention and mobility restrictions.
For each part of ICF, give examples.
Assessment and treatment should consider all ICF domains, not just physical impairments
How they affect activities, participation, and how environment/personal factors contribute
Health Condition
Parkinson’s disease
Osteoporosis
Post-stroke
Body Functions and Structures
Decreased strength
Poor balance
Visual deficits
Vestibular dysfunction
Joint limitations or pain
Activity Limitations
Walking on uneven surfaces
Rising from a chair
Climbing stairs
Maintaining balance during turns
Participation Restrictions
Avoiding community outings due to fear of falling
Unable to work
Attend social gatherings
Exercise with others
Environmental Factors
Poor lighting, loose rugs (barriers)
Use of grab bars, walker, handrails (facilitators)
Personal Factors
Fear of falling
Motivation and confidence
Age
Previous fall history
Cognitive status
What examination procedures can be utilized to assess fall risk? For each of the following state what they are and the scoring for increased fall risk
Berg Balance Scale
Tinetti performance oriented mobility fall risk
Functional Reach Test
Four Square Step Test (FSST)
Timed Up and Go (TUG)
Walking While Talking Test
Dynamic Gait Index (DGI) or Modified DGI
Berg Balance Scale (BSS): 4-item test assessing static and dynamic balance (standing, reaching, turning)
Score <45/56 = increased fall risk
Tinetti Performance-Oriented Mobility Assessment (POMA): Evaluates gait and balance components
Score <19/28 = high fall risk
Functional Reach Test: Measures limits of stability (how far a person can reach forward without losing balance)
Reach <6 inches = high fall risk
Four Square Step Test (FSST): Assesses ability to step over objects in multiple directions quickly
Time >15 seconds = higher risk of falls in older adults
Timed Up and Go (TUG): Measures mobility, balance, and fall risk. Can add dual-task component
Time >13.5 seconds = increased fall risk
Walking While Talking Test: Assesses dual-task performance
Delays or stops while talking suggest increased fall risk
Dynamic Gait Index (DGI) or Modified DGI: Assesses gait under varied conditions (head turns, obstacles)
Score <19/24 = predictive of falls
Explain each of the following:
Independent
Supervision
Close guarding
Contact guarding
Minimum assistance
Moderate assistance
Maximum assistance
1. Independent: Patient is able consistently to perform skill safely with no one present.
2. Supervision: Patient requires someone within arm’s reach as a precaution; low probability of patient having a problem requiring assistance.
3. Close Guarding: Person assisting is positioned as if to assist, with hands raised but not touching patient; full attention on patient; fair probability of patient requiring assistance.
4. Contact Guarding: Therapist is positioned as with close guarding, with hands on patient but not giving any assistance; high probability of patient requiring assistance.
5. Minimum Assistance: Patient is able to complete majority of the activity without assistance.
6. Moderate Assistance: Patient is able to complete part of the activity without assistance.
7. Maximum Assistance: Patient is unable to assist in any part of the activity.
How do functional balance tests relate to determining fall risk?
Functional balance grades? (5)
Identify Fall Risk Level
Low, moderate, or high risk for falling
Guide Intervention Planning
Balance, strength, dual-task training
Results reveal specific balance, strength, or coordination deficits
Track Progress Over Time
Repeat testing shows objective changes, helping assess the effectiveness of treatment and adjust goals
MDC and MCID
Support Referrals or Justify Needs
Assistive devices
Home modifications
Functional Balance Grades:
1. Normal: Patient able to maintain steady balance without support (static). Accepts maximal challenge and can shift weight easily and within full range in all directions (dynamic)
2. Good: Patient able to maintain balance without support, limited postural sway (static). Accepts moderate challenge; able to maintain balance while picking object off floor (dynamic)
3. Fair: Patient able to maintain balance with handhold support; may require occasional minimal assistance (static). Accepts minimal challenge; able to maintain balance while turning head/trunk (dynamic)
4. Poor: Patient requires handhold and moderate to maximal assistance to maintain posture (static). Unable to accept challenge or move without loss of balance (dynamic)
5. No balance
Shorter version:
Normal:
Static: No support
Dynamic: maximal challenge
Good:
Static: No support
Dynamic: moderate challenge (maintain balance picking up object from floor)
Fair:
Static: Handhold support, occasional min assistance
Dynamic: minimal challenge (maintain balance with head/trunk turning)
Poor:
Static: Handhold support and mod to max assistance
Dynamic: No challenge
None:
No balance
Based upon a case scenario, select the most appropriate balance tests and measures. For each of the following state the population and when to use:
Berg balance scale
Tinetti performance oriented mobility assessment
Functional reach test
Four square step test
Timed up and go
Walking While Talking Test
Dynamic Gait Index (DGI) or Modified DGI
Berg Balance Scale (BBS): Older adults, stroke patients, patients with static and dynamic balance deficits
Use when: You need a comprehensive balance profile (14 tasks). The patient can stand and follow directions safely
Tinetti Performance-Oriented Mobility Assessment (POMA): Older adults at risk for falls, patients with gait deviations and poor postural control
Use when: You want to assess both gait and standing balance, You have moderate time available, and Patient ambulatory
Functional Reach Test: Frail older adults, patients with limited time, space, or endurance
Use when: You want a quick snapshot of limits of stability and patient is able to stand unsupported
Four Square Step Test (FSST): Community-dwelling older adults, patients who report tripping, poor coordination, or difficulty changing directions
Use when: You want to assess dynamic balance and stepping in multiple directions
Timed Up and Go (TUG): General fall risk screening in older adults, patients who are ambulatory
Use when: You want a fast, functional measure of mobility and you can add TUG-cognitive to assess dual-task ability
Walking While Talking Test: Older adults with cognitive decline or distraction-related falls
Use when: You want to evaluate dual-tasking and attention while walking
Dynamic Gait Index (DGI) or Modified DGI: Community-dwelling adults, especially those with vestibular, neurological, or sensory issues
Use when: You need to assess walking under varied conditions (head turns, obstacles)
How can we help patients prevent falls?
Treatment of acute or chronic conditions
Consult with MD regarding medications
Exercise programs
Gait training
Balance training
Strength training
Proper fit and use of assistive devices
Proper footwear
Daily Activity
Repetition and practicing functional movements
Referrals
PT
OT
Orientation and Mobility Specialist (low vision)
Given a case scenario, design physical therapy interventions related to fall prevention.
What exercise programs?
What gait and balance activities?
What type of tech?
Exercise Programs: Strength training, Endurance, Flexibility, Posture, Attention to precautions, Safety, Aerobic training
Gait and Balance: Specificity (home and community), Dual tasking, Directional changes, Obstacle course, Response strategies to perturbations
High Tech: Virtual reality, Computerized balance training, Gaming systems
Perform an environmental assessment and be able to recommend adaptive equipment.
Safety training
Environmental Modifications: Recommend lighting upgrades like bright, non-glare lights in hallways and bathrooms
Remove trip hazards like Rugs or Cords. Suggest grab bars in the bathroom, non-slip mats, and clearly marked steps
Assistive Device Prescription: Assess need for a cane or walker based on balance testing. Train in safe use of the device on different surfaces and with dual-tasking
Dressing assistance
Elastic shoe laces
Reacher
Home Safety Assessment: Recommend changes like handrails, bathroom aids, nightlights, decluttering
Be able to determine the best fall recovery strategies for a given patient
What systems can be use?
Encouraging the patients to keep what within reach?
Teach patients how to do what safely?
Educate patients and caregivers on?
Emergency Alert Systems: Devices (worn or installed) that let the patient quickly call for help after a fall, especially useful for those living alone.
Portable or Cell Phone: Encouraging the patient to keep a phone within reach at all times so they can call for help if needed.
Floor Transfer Training: Teaching patients how to safely get up from the floor or reach a stable position after a fall to prevent long periods on the ground.
Education: Informing patients and caregivers about fall risks, safe movement techniques, and what to do after a fall to reduce fear and improve response.
How does fear of falling impact behavior and fall risk?
Causes what and leads to what?
Increased risk of failing that leads to a vicious cycle, what is the cycle?
Patient education?
Behavioral modification?
Causes social isolation, limited mobility, and weakness → activity avoidance, physical deconditioning, loneliness and depression.
Increased risk of falling that leads to a vicious cycle: Fear → inactivity → weakness → instability → higher risk → more fear
Patient Education: Teach about safe movement strategies, fall prevention, and how activity builds strength and confidence.
Behavioral Modification: Gradually increase challenging activities to rebuild trust in mobility. Incorporate positive reinforcement and goal-setting
When would vibrating insoles or hip protectors be appropriate to prescribe for a patient? How do they work?
When to Prescribe Vibrating Insoles
For older adults with balance impairments but who are still ambulatory. Especially useful for peripheral neuropathy and age-related sensory decline
Vibrating insoles deliver subsensory vibratory noise to enhance sensory input, which can improve gait stability, postural control, reduced sway
When to Prescribe Hip Protectors
Do not prevent falls, they might be helpful in preventing fractures. Appropriate if the patient has low bone density, a history of hip fractures, is frail or in a long-term care setting
Help protect the greater trochanter from impact during a fall. May include hard plastic shields or soft foam pads
Be familiar with the evidence-based approaches to fall prevention.
Matter of balance
STEADI (What is it? Consists of? Three questions to screen for fall risk)
Matter of Balance: Program that emphasizes practical strategies to reduce fear of falling and increase activity levels.
Participants learn to view falls and fear as controllable, set realistic goals to increase activity, change their environment to reduce fall risk factors, and exercise to increase strength and balance.
STEADI: “Stopping Elderly Accidents, Deaths and Injuries”
Tool Kit for Health Care Providers: offers educational brochures and resources for patients and caregivers
Look for OH (BP irregularities such as hypertensive crisis)
Falls, screening options, medications linked to falls, standardized gait and balance assessment tests, online trainings that offer continuing education
Three Questions to Screen for Fall Risk
Have you fallen in the past year?
Do you feel unsteady when standing or walking?
Do you worry about falling?

Compare and contrast the normal gait pattern with typical gait changes in older adults.
What would you see decrease and increase?
Decreased gait speed
Decreased step or stride length
Increased stance time and double limb support time
Increased variability of gait
Decreased excursion of movement at the hip, knee, and ankle
Decreased reliance on ankle kinetics and power
Less upright posture
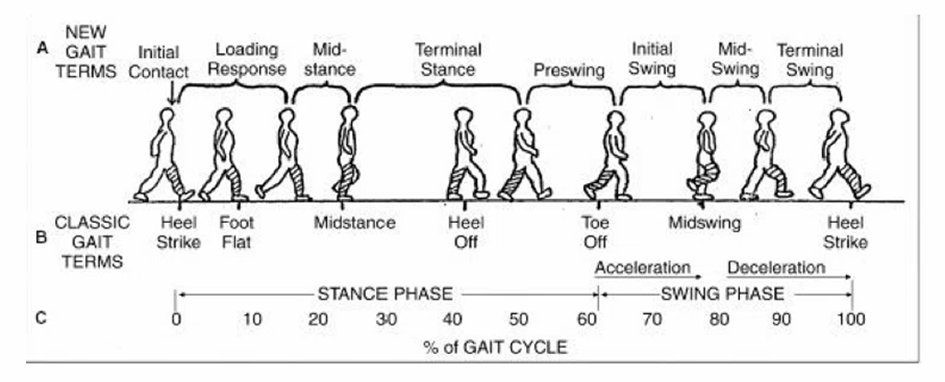
Be familiar with the phases of normal gait. What are the three primary tasks of gait?
Three primary tasks of gait: weight acceptance, single limb support, limb advancement
What sensory systems are related to postural control and balance? How does the CNS relate to these systems?
Visual System: Provides information about the environment, orientation, and movement relative to surroundings
Somatosensory System (Proprioception): Detects body position, movement, and surface contact
Vestibular System: Detects head position and motion relative to gravity
The central nervous system integrates input from all three systems to maintain balance. If one system is compromised, the others must compensate.
Describe recovery strategies related to balance perturbations.
Ankle strategy
Muscle sequence?
Hip strategy
Muscle sequence?
Stepping strategy
Reaching/Grasping strategy
Important for fall prevent in what population?
Suspensory strategy
Ankle Strategy: Small, slow perturbations on a firm surface
Distal to proximal muscle sequence
Hip Strategy: Larger, faster perturbations or when the ankle strategy is insufficient. Rapid hip flexion or extension moves the center of mass over the base of support
Proximal to distal muscle sequence
Stepping Strategy: Very large or fast perturbations when balance cannot be regained with ankle or hip movements. A step is taken in the direction of the instability to widen the base of support
Reaching/Grasping Strategy: Stabilize by grabbing an object
Important for fall prevention in older adults
Suspensory Strategy: Lowering the center of mass to be closer to the base of support. Bending the knees during standing or ambulation
What skills would be necessary for community ambulation?
Starts and stops
Acceleration and deceleration
Sideways stepping
Backward stepping
Changing directions
Obstacle clearance and avoidance
Picking up, carrying, or putting down objects
Turning around
Pushing and pulling doors
Managing displacement forces
Terrain changes
Lighting changes
Weather changes
Stepping up and down curbs, stairs, and ramps of different heights and grades
What activities would be included when training patients to resume community ambulation?
Varying Terrain Practice: Grass, gravel, ramps, curbs, uneven surfaces
Crossing Streets: Timed walking (simulate traffic signals), increased gait speed
Car Transfers: Practice entering/exiting vehicles safely
Stair Navigation: With and without handrails, practice ascent and descent
Dual Tasking: Walking while talking, holding objects, or counting
Carrying Items: Practice with shopping bags or small loads
Endurance Training: Extended walking sessions to simulate real distances
Navigating Obstacles: Walking around cones, stepping over objects, changing directions
Be able to prescribe an appropriate assistive device for a patient, based on a case scenario.
Single point cane
Quad cane
Standard walker
Front wheel walker (2WW)
Four wheel walker (Rollator)
Hemi walker or Narrow base quad cane
Single-Point Cane: Mild balance loss, needs occasional support. Increases base of support, minimal assistance
Quad Cane: Moderate balance deficits, slower gait speed. More stable than a single-point cane
Standard Walker: Prescribed when a patient needs maximum stability and support for walking but still has enough upper body strength and balance to lift the walker safely
Front-Wheeled Walker (2WW): Bilateral lower extremity weakness, needs moderate support. Provides continuous support without needing to lift the walker
Four-Wheeled Walker (Rollator): Poor balance, history of falls, needs maximal support. Offers high stability, includes a seat and storage for independence
Hemi-Walker or Narrow-Base Quad Cane: Significant one-sided weakness or asymmetry (post-stroke). More support than a cane but still unilateral
How do concentric and eccentric contractions relate to stair climbing?
Stair ascent and descent. What muscles fire for each?
Stair Ascent (Going Upstairs) → Concentric Contractions Dominate
Quads, glutes, calves contract concentrically to lift the body upward.
Muscles shorten as they generate force to extend the knee, hip, and ankle.
Stair Descent (Going Downstairs) → Eccentric Contractions Dominate
Quads and glutes contract eccentrically to control the lowering of the body.
Muscles lengthen under tension to prevent a rapid or uncontrolled descent.
Why would gait speed be considered a functional vital sign?
What gait speed is considered “dead”?
serves as a highly reliable, objective summary of an individual's overall physiological health and functional capacity. It is clinically useful and flexible
<2 MPH = dead. A commonly used threshold that delineates older adult community ambulators from those who are more limited is 1 m/s
Be able to prescribe a gait training program based on the patient’s functional impairments.
Consider how to progress the patient during gait training and how to use a task specific approach during physical therapy treatment sessions.
Nothing on ashleys
How does dual tasking relate to gait training activities?
Dual Tasking: Walking while talking, holding objects, or counting
Gait and Balance: Specificity (home and community) dual tasking, directional changes, obstacle course, response strategies to perturbations
Be able to perform an examination/evaluation on an older patient/client.
What is crucial to understand?
Environmental assessment include what modifications?
For adaptive equipment, what is important to remind them about?
Assess support includes? Take into consideration what 2 things?
Cognitive and psychological functioning
What are three assessments that can be used to assess mental status?
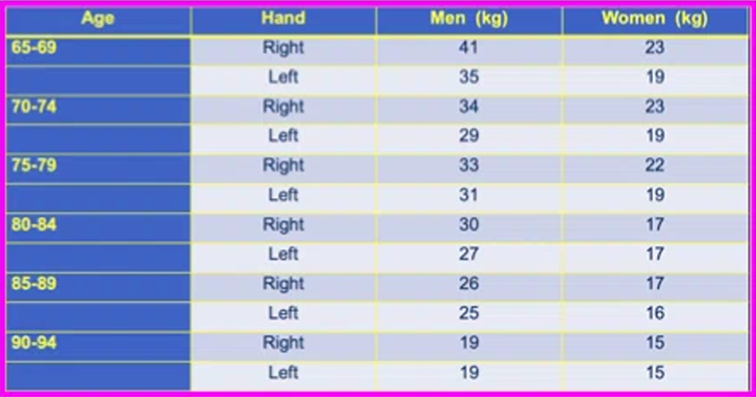
Grip strength test
Lower grips strength is associated with?
CRUCIAL to understand their home or environmental situation
Environmental Assessment: home modifications
Adaptive Equipment Needs: Remind them this will not make them dependent on something, but rather help them stay INDEPENDENT!
Assess Support: family, friend, financial resources
▪ Take into consideration patient AND family goals
Cognitive and Psychological Functioning
Depression, dementia, how many command can they follow at once
Take into consideration: mental status, orientation, learning style, ability to follow directions, psychosocial functioning
Geriatric Depression Scale
Montreal Cognitive Assessment (MoCa)
Short Blessed Cognitive Test: Sensitive to early cognitive changes associated with Alzheimer’s disease
Grip Strength Testing
Lower grip strength is associated with a higher risk of mortality
What is the purpose of the Senior Fitness Test?
Assess the physical abilities in relation to everyday functional tasks of older adults (typically 60+ years) in comparison to others in their age category
How would you perform the various components of the Senior Fitness Test?
Chair stand test
Risk Zone?
Arm curl test (how weight for men and for women)
Risk Zone?
6 minute walk test
Risk Zone?
2 minute step test
Risk Zone?
Chair Sit-and-Reach test
Risk Zone (for men and for women)?
Back stretch test
Risk Zone (for men and for women)?
8 foot up and go test
Risk Zone?
Height and weight
Normal BMI range for older adults?
Chair Stand Test (Lower Body Strength): Sit in a chair with arms crossed over chest. Stand up and sit down as many times as possible in 30 seconds.
a. Risk Zone: < 8Arm Curl Test (Upper Body Strength): Seated, curl a dumbbell (5 lbs women / 8 lbs men) as many times as possible in 30 seconds.
a. Risk Zone: < 116-Minute Walk Test (Aerobic Endurance): Walk as far as possible in 6 minutes
a. Risk Zone: < 350 yards2-minute Step Test (Alternate for Aerobic Endurance): March in place for 2 minutes, raising knees
a. Risk Zone: <65 stepsChair Sit-and-Reach test (lower body flexibility): sit on edge of chair, extend one leg forward with heel on floor. Reach toward toes with both hands for 2 seconds
a. Risk Zone: Men = 4 inches; Women = 2 inchesBack scratch test (upper body flexibility): one hand over shoulder, other up the back; try to touch fingertips (+ if overlap, - if gap)
a. Risk Zone: Men = 4 inches, Women = 2 inches8-foot up-and-go test (agility/dynamic balance): from seated position, stand up, walk 8 feet, turn around, and sit back down
a. Risk Zone: > 9 secondsHeight and Weight (Body Composition): BMI = weight (kg) / height² (m²)
a. Normal BMI range for older adults = 18.5-24.9
Case Study: When performing the Senior Fitness Test, your patient did only 5 unassisted stands during the 30 - second chair stand component which puts him in the risk zone. Why is this score significant and what impact does this information have on your physical therapy intervention?
Falls into the “risk zone” (<8): This indicates marked lower body weakness, especially in the hip and knee extensors
Therapy: Focus on quadriceps, glutes, hamstrings, and core stabilization. Begin with assisted sit to-stands, mini-squats, step-ups, and resistance band work. Practice tasks like transfers, toilet/bed mobility, and stairs in therapy
Be familiar with patient examination procedures. Have an understanding about the mentioned tests and measures and how the scores impact your physical therapy intervention.
Vital Signs → At rest and following an activity
Strength → Functional strength, grip strength, MMT might not be the best
Circulatory Status → Capillary refill, rubor of dependency, venous filling time
Sensation → Monofilament testing, protective sensation, diabetes
Be able to select the appropriate tests and measures based upon a case scenario.
Timed up and go
Functional reach
Berg balance scale
Tinetti assessment tool
Dynamic gait index
Toe tap test
Walking while talking test
Rhomberg test
Occiput to wall test
Timed Get Up and Go: Quick measure of basic mobility and balance
Most adults walk 10 ft (3 m) in 10 seconds → More than 30 seconds indicates dependency with mobility and ADLs
If an assistive device is required, the type is recorded
TUG cognitive and TUG manual can also be utilized to assess the ability to perform dual tasking. Slower time with these is expected because of dual tasking.
Functional Reach: Examines limits of stability for individuals with balance disorders at high risk of falls
Greater than 10 inches = not likely to fall
6 to 10 inches = 2 times more likely to fall
1 to 6 inches = 4 times more likely to fall
Unwilling to reach = 28x more likely to fall
Berg Balance Scale: Status and dynamic balance with functional tasks
Maximum score: 56 points
Less than 45 points is associated with a high risk of falls
Tinnettii Assessment Tool: Also called Performance-Oriented Mobility Assessment (POMA), assesses a person's perception of balance and stability during activities of daily living and their fear of falling
Scores less than 19 = a high risk for falls
Scores between 19 and 24 = moderate risk for falls
Dynamic Gait Index: Ability to perform variations in walking on command
Maximal possible score = 24
Score below 19 = increased fall risk
Toe Tap Test: Assess motor speed and coordination of the dorsiflexors, may also reflect basal ganglia or cerebellar dysfunction if impaired
Young (av. 32 yr): 47 taps per 10 seconds
Older adults (av. 72 yr): 34 taps per 10 seconds
Walking While Talking Test: Walk at self-selected comfortable speed 20 feet and then return, for a total of 40 feet
Simple (recite the alphabet): ⩾ 20 seconds = high fall risk
Complex (recite every other letter): ⩾ 33 seconds = high fall risk.
Rhomberg Test: Assess balance, particularly the role of proprioception
Feet Together: Eyes Open, Eyes Closed
Sharpened Rhomberg with Feet in Tandem: Eyes Open, Eyes Closed
Occiput to Wall Test: Postural Assessment
Standing with buttocks and midback against the wall, eyes focused straight ahead. Inability to touch the wall with the back of the head (occiput) is a positive finding for flexed posture
Given specific components of a test, be able to prescribe a physical therapy intervention.
TUG
Functional reach test
Berg balance scale
Tinetti assessment tool
Dynamic gait index
Toe tap test
Walking while talking test
Rhomberg or sharpened Rhomberg
The balance outcome measure for elder rehabilitation (BOOMER)
Timed Up and Go (TUG): Gait training with/without assistive device (AD), sit-to-stand and turn practice, strengthening of LE (quads, glutes)
Functional Reach Test: Static & dynamic balance training (reaching outside BOS), core and trunk stability exercises, standing weight shifts, reaching tasks
Berg Balance Scale (BBS): Stepping over obstacles, reaching
Tinetti Assessment Tool: Gait training, practice safe transfers, use mirrors or visual feedback for posture correction
Dynamic Gait Index (DGI): Walking while turning head, changing speed, stepping over obstacles, dual-task gait training (counting, carrying objects)
Toe Tap Test: Ankle dorsiflexion strengthening, fast alternating foot movements (marching, quick steps), rhythmic coordination drills (metronome-based)
Walking While Talking Test: Cognitive-motor training, community simulation (crossing street, navigating while talking)
Rhomberg or sharpened Rhomberg: balance exercises with reduced vision (eyes closed, foam surface), tendem stance or narrow BOS activities
The Balance Outcome Measure for Elder Rehabilitation (BOOMER): Assesses standing balance and functional mobility in the elderly population
Your patient scored a 20 on the Mini-Mental State exam. How would you modify your treatment?
Maximum points is? A score below ___ indicated cognitive impairment?
What condition may affect the score of the MMSE?
The MMSE is _______ and must be _______ for clinical use
Simplify instructions ➔ Use visual and verbal cues ➔ Increase repetition ➔ Create a structured routine ➔ Tie exercises to functional tasks to improve relevance and engagement ➔ Monitor safety closely
Maximum points is 30: A score below 24 indicates cognitive impairment, not considered normal for an older adult
Depression may be reflected on the MMSE. As the depression improves, the MMSE score will also increase.
The MMSE is copyrighted and MUST be purchased for clinical use
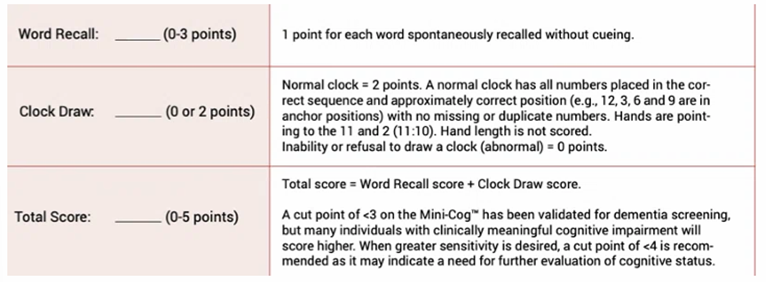
What are the components of the MoCA and Mini-Cog?
MoCA: Assesses what? What does it consist of? You must be what to use MoCa? Time to administer is? Total score is? A score of __ or above is consider normal.
Mini-Cog: Quick screening for what and the results help determine what? What three things does it consist of? Total score of? Cut point of ___ has been validated for dementia screening.
Montreal Cognitive Assessment (MoCA): Assesses cognitive domains
Attention and concentration, executive functions, memory, language, visuoconstructional skills, conceptual thinking, calculations, and orientation.
You must be certified to use the MoCa
Time to administer: 10 minutes.
The total possible score is 30 points
A score of 26 or above is considered normal.
Mini-Cog: quick screening for early dementia detention → identify possible cognitive impairment in older people, results help determine when it might be time for more in-depth testing.
Three Word Registration, Clock Drawing, Three Word Recall
Cut point of <3 has been validated for dementia screening
Total possible score is 5
Your patient scored a 380 on the Holmes and Rahe Life Events Scale. Why is this significant? Scoring?
Indicates your patient is experiencing significant stress, which may impact healing, motivation, immune function, and treatment adherence
Score greater than or equal to 300 → High risk of illness or health breakdown due to stressful life events
Score of 150 to 299 → Moderate to high chance of a serious illness
Score below 150 → Indicates mild stress of a lot to moderate risk of serious illness in the near future
Your patient scored a 17 on the Tinetti Gait and Balance test. What does this score indicate? Scoring?
HIGH fall risk
Indicates your patient is at a significantly increased fall risk and suggests balance and gait impairments that require immediate intervention
Maximum score = 28
Score < 19 = High risk for falls
Your patient scored a 48/56 on the Berg Balance test. How does this information relate to fall risk?
48 = Borderline fall risk → patient may be functionally independent but still at moderate fall risk, especially with more complex or dynamic tasks
Score ≤ 45 = Increased fall risk
Your patient scored a 33 on the Fullerton Advanced Balance Scale. What does this mean? Scoring?
Indicates your patient is not at high risk for falling but may have some difficulty with advanced balance tasks (turning, stepping over obstacles, tandem walking)
Test of both static and dynamic balance under varying sensory conditions.
Designed to measure balance in higher-functioning active older adults.
Score of 33: Below the optimal cutoff for high-functioning balance
Cutoff for fall risk: Typically ≤25 suggests high fall risk in older adults
Max score of 40 (google)
Your patient was able to complete the Four Square Step Test in 19 seconds. What does this mean? Scoring?
Increased risk of falls and likely has reduced dynamic balance and coordination
>15 seconds = Increased fall risk
≤15 seconds = Lower fall risk (normal mobility)
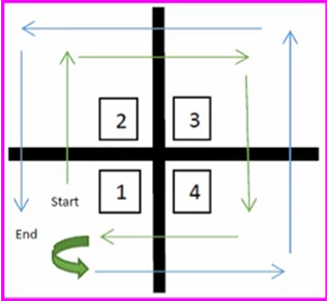
When does the timing begin and end with the Four Square Step Test? The Timed Up and Go?
The Four Square Step Test:
As soon as the first foot touches the floor in square 2. It’s not when the command is given or when they start moving in square 1, it starts when they step into square 2.
Timing ends: both feet return to square 1 after completing the full sequence
The Timed Up and Go:
On the command “Go,” when the patient’s back leaves the chair. Do not start the timer on the verbal cue alone; it's triggered by movement initiation.
Timing ends: patient sits back down and their back touches the chair again.
How does grip strength relate to predicted functional decline?
It is a simple yet powerful indicator of overall muscle strength, physical function, and even mortality risk.
Low grip strength is associated with weakness in other major muscle groups, making it a quick screen for global sarcopenia (age-related muscle loss)
What are the components of the AFIT? What is it used to identify?
Components: General health history, vital signs, posture, flexibility, balance, endurance, and strength
“Adult Functional Independence Test”: This performance-based functional assessment tool identifies potential problems early so they can be addressed using an individualized exercise program prescribed by a PT
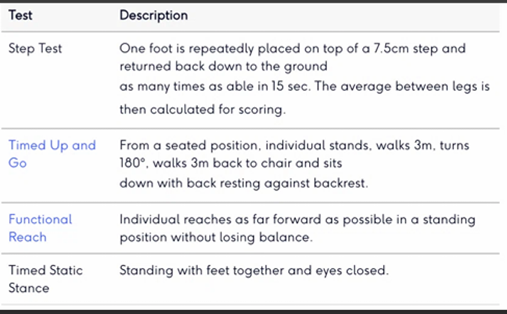
What are the components of the BOOMER? Scoring?
Components: Step Test, Timed Up and Go, Functional Reach, Timed Static Stance
“Balance Outcome Measure for Elder Rehabilitation”: For older adults with deficiencies in standing balance
Maximum score is 16. Each item (4 items) can score between 0 (unable to perform the test) to 4 (excellent). A minimum clinically significant change in the BOOMER is 3 points over its 16-point scale range
How is the Walking While Talking test administered? What do the scores indicate?
Walk at a comfortable speed 20 feet and then return, for a total of 40 feet
Simple (recite the alphabet): 20 seconds or longer = high fall risk
Complex (recite every other letter): 33 seconds or longer = high fall risk.
What is polypharmacy? Increases risk of? What is a critical element in comprehensive care?
The use of FIVE or more medications at once
It increases the risk of drug interactions, side effects, confusion, falls, and medication non adherence
Optimization of the medication regimen is one of the critical elements in comprehensive geriatric care.
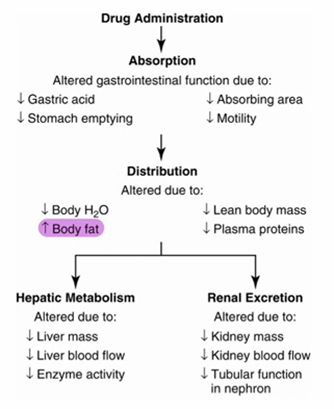
How does aging impact drug absorption, distribution, metabolism, and excretion?
Calcium is a ____ _____ vitamin and can become what?
Absorption: Slower gastric emptying and reduced blood flow may delay absorption onset
Distribution: Increased body fat leads to increased storage of fat-soluble drugs (diazepam) which leads to prolonged action. Decreased lean body mass and total body water leads to increased plasma concentration of water-soluble drugs.
Calcium is a fat soluble vitamin and can become toxic!
Metabolism (Liver): Reduced hepatic blood flow and enzyme activity leads to slower metabolism of certain drugs which leads to longer half-lives and risk of drug accumulation
Excretion (Kidneys): Decreased glomerular filtration rate (GFR) leads to reduced clearance of renally-excreted drugs. This slower excretion raises the risk of overdose and toxicity
What are some of the common adverse drug reactions in older adults?
Cognitive & Central Nervous System (CNS) Effects
Balance, Falls, and Mobility
Gastrointestinal (GI) and Urinary Issues
Metabolic/Electrolyte Imbalances
Cognitive & Central Nervous System (CNS) Effects
Confusion, delirium (from anticholinergics, opioids, benzodiazepines)
Sedation (opioids, benzodiazepines, antipsychotics)
Depression (beta-blockers, corticosteroids, sedatives)
Fatigue & weakness (CNS depressants, antihypertensives, diuretics)
Extrapyramidal symptoms → movement disorders, tremors, rigidity, bradykinesia (antipsychotics, metoclopramide)
CNS effects → hallucinations, cognitive decline (anticholinergics, corticosteroids)
Balance, Falls, and Mobility
Falls & dizziness (sedatives, benzodiazepines, antihypertensives)
Orthostatic hypotension (antihypertensives, diuretics, nitrates)
Fatigue & general weakness (diuretics, statins, beta-blockers)
Peripheral effects → numbness, tingling (chemotherapy agents, antidiabetics)
Gastrointestinal (GI) and Urinary Issues
GI bleeding (NSAIDs, corticosteroids, anticoagulants)
Nausea and vomiting (opioids, antibiotics, digoxin)
Constipation (opioids, calcium channel blockers, anticholinergics)
Urinary retention (anticholinergics, antihistamines, tricyclic antidepressants)
Metabolic/Electrolyte Imbalances
Electrolyte disturbances → hyponatremia, hypokalemia (diuretics, laxatives)
Dehydration (diuretics, laxatives, poor intake due to cognitive decline)
How would you recognize depression in an elderly patient?
Hopelessness and helplessness
Anxiety and worry
Memory problems
Weight loss
Loss of feeling pleasure
Slowed movement
Irritability
Lack of interest in personal care
Tiredness, listless
Unexplained aches or pain
How is depression treated?
Pharmacotherapy: mostly biochemical, sometimes situational
Psychotherapy: maybe talking is not for them, but maybe it is!
Exercise and Physical Activity: endorphins
Sidenote: emotional support animals
How would depression or social isolation impact your physical therapy intervention?
Patient may lack?
What is the suicide and crisis lifeline number?
Reduced adherence to?
Loneliness is a public health threat!
Patients may lack the energy, interest, or hope to attend sessions or complete exercises
988: Suicide and crisis lifeline
Reduced adherence to home programs or follow-through on care plans.
How would you recognize caregiver stress? What coping strategies could you suggest?
Signs: Denial, anger, social withdrawal, anxiety, depression, exhaustion, sleeplessness, irritability, lack of concentration, health problems
A few simple steps can help prevent exhaustion:
Plan ahead to be sure you have the supplies and resources you need.
Take one day at a time.
Develop contingency plans for emergencies and obstacles.
Accept help, don’t take on more than you can handle.
Make YOUR health a priority. Get enough rest and eat properly.
Make time for leisure.
Be good to yourself!
Share your feelings with others, it’s okay to be tired and frustrated
What would be considered normal cognitive aging?
Abilities That Remain Stable or Decline Minimally
Implicit memory?
Emotional regulation often?
Long term autobiographical memory is?
Cognitive Functions That Typically Decline Gradually
Processing speed?
Word finding and name recall?
Executive function?
Cognitive flexibility?
Working memory (short-term retention and manipulation of information)?
Encoding information?
Abilities That Remain Stable or Decline Minimally
Implicit (procedural) memory remains stable → riding a bike, brushing teeth, social/emotional responses
Emotional regulation often improves or remains intact
Long-term autobiographical memory (recall of meaningful past events) is generally preserved
Cognitive Functions That Typically Decline Gradually
Processing speed slows (tasks take longer)
Word-finding and name recall may become slower or more difficult
Executive functions decline → includes planning, multitasking, switching tasks, and problem solving.
Cognitive flexibility is reduced → may struggle to adapt if routines or familiar strategies fail
Working memory (short-term retention and manipulation of information) becomes less efficient.
Encoding new information becomes harder, especially under distraction
In general, how do personality traits relate to aging?
What two personality traits tend to increase with age? What three decrease?
These changes are often seen as part of the _____ principle.
Agreeableness and Conscientiousness tend to increase with age
Extraversion, Neuroticism, and Openness to experience tend to decrease
These changes are often seen as part of the "maturity principle" → people become more emotionally stable and less open to new experiences
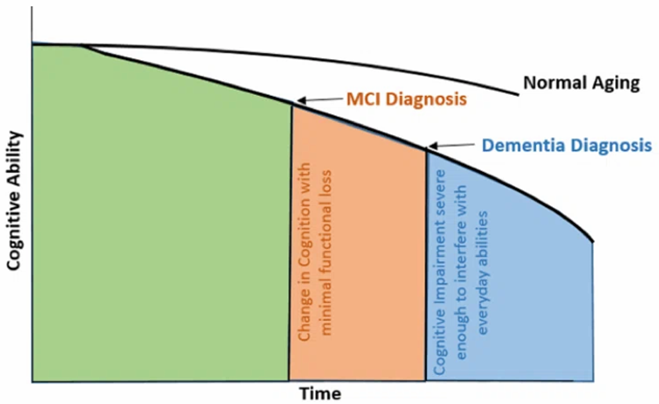
Describe the continuum of cognitive change as we age.
The continuum spans from normal aging to severe cognitive impairment, and reflects a gradual spectrum (not an all-or-nothing process)
What is cognitive reserve?
The brain's ability to withstand the negative effects of aging or brain damage, and maintain cognitive function despite such challenges.
It's a measure of the brain's flexibility and efficiency in adapting to changing circumstances, essentially acting as a buffer against cognitive decline.
Helps individuals maintain function and live longer with minimal cognitive decline
Describe the four types of memory.
Working
Episodic
Semantic
Remote
Working memory: Remembering bits of information
Episodic memory: Memory of an event or episode
Semantic memory: Language based, memory for facts and words
Remote memory: Past events