week 38 - vulvar cancer and vulvar premalignancies
0.0(0)
Studied by 1 personCard Sorting
1/8
There's no tags or description
Looks like no tags are added yet.
Last updated 4:05 PM on 7/8/26
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
9 Terms
1
New cards
vulvar malignancies intro
* may be around 7% of all gynaecological malignancies
* SCC is the most common type of vulvar malignancy (80-85%)
* vulvar biopsy is essential in most cases to determine the histopathological diagnosis
preferrably taken from the edge of the lesion including a small piece of normal tissue
* SCC is the most common type of vulvar malignancy (80-85%)
* vulvar biopsy is essential in most cases to determine the histopathological diagnosis
preferrably taken from the edge of the lesion including a small piece of normal tissue
2
New cards
vulvar SCC
* 2 types, each with their own premalignancy → HPV dependent and independent
* HPV + → HSIL (high grade squamous intraepithelial lesion) → SCC
mostly HPV 16 and 18
* HPV - → LS (lichen sclerosus) → differentiated VIN (differentiated vulvar intraepithelial neoplasia) → SCC
or
HPV - → LS → SCC
* dVIN seems to have a very short intraepithelial phase until malignancy
* the malignant potential of HSIL appears be lower compared with dVIN but higher than LS
so least to most likely = LS → HSIL → dVIN
* *there is a rise in absolute numbers of vulvar SCC due to both an increase in HPV infections of the genital tract and the proportional increase in the average age of the population*
* recent terminology consists of a two-tier classification for HPV-related lesions to improve reproducibility by the pathologist: low SIL (LSIL) and HSIL
* HPV + → HSIL (high grade squamous intraepithelial lesion) → SCC
mostly HPV 16 and 18
* HPV - → LS (lichen sclerosus) → differentiated VIN (differentiated vulvar intraepithelial neoplasia) → SCC
or
HPV - → LS → SCC
* dVIN seems to have a very short intraepithelial phase until malignancy
* the malignant potential of HSIL appears be lower compared with dVIN but higher than LS
so least to most likely = LS → HSIL → dVIN
* *there is a rise in absolute numbers of vulvar SCC due to both an increase in HPV infections of the genital tract and the proportional increase in the average age of the population*
* recent terminology consists of a two-tier classification for HPV-related lesions to improve reproducibility by the pathologist: low SIL (LSIL) and HSIL
3
New cards
vulvar premalignancies
1. lichen sclerosus:
* most likely autoimmune, chronic genital skin disorder
* might not actually be a premalignancy but since the majority of SCCs develop in a LS background…
* the lifetime risk of vulvar SCC in LS patients is around 2-5%
* can occur in all ages but mainly in prepubertal girls and postmenopausal women
* incidence is unknown
* main symptom → pruritus
other symptoms → soreness, pain, burning, dyspareunia, irritation, urinary or defecation problems, bleeding or blistering
* constipation and/or dysuria due to soreness and itching are generally ==__presenting symptoms in prebubertal girls__==
^ may be mistaken for sexual abuse
* anatomical changes → resorbption of labia minora, clitoris becomes buried under a scarred and fused clitoral prepuce and the introitus (vaginal entrance) is often narrowed
* the entire genital area can be affected with areas of erythema, ecchymosis, pallor, fissures, hyper/hypopigmentation, variable degrees of oedema, ulceration and hyperkeratosis
* the vaginal mucosa is NOT afected (unlike lichen ruber planus)
* 10-20% have extra genital manifestations → eg. white papules or atrophic macules on the trunk, neck, upper legs, wrists and head
* 30% are asymptomatic but the rest may have secondary infection, adhesion of the clitoral hood with formation of a smegmatic pseudocyst and narrowing of the introitus (makes sex and micturition difficult)
* *surgery only relieves these symptoms in some cases; this relief is sometimes temporary and subsequent corticosteroid therapy, applied on a vaginal dilator, is required*
* typically a clinical diagnosis but if therapies dont work or conclusion is not complete a biopsy might be needed
* it often resolves with age but the risk of recurrence later in life is unknown
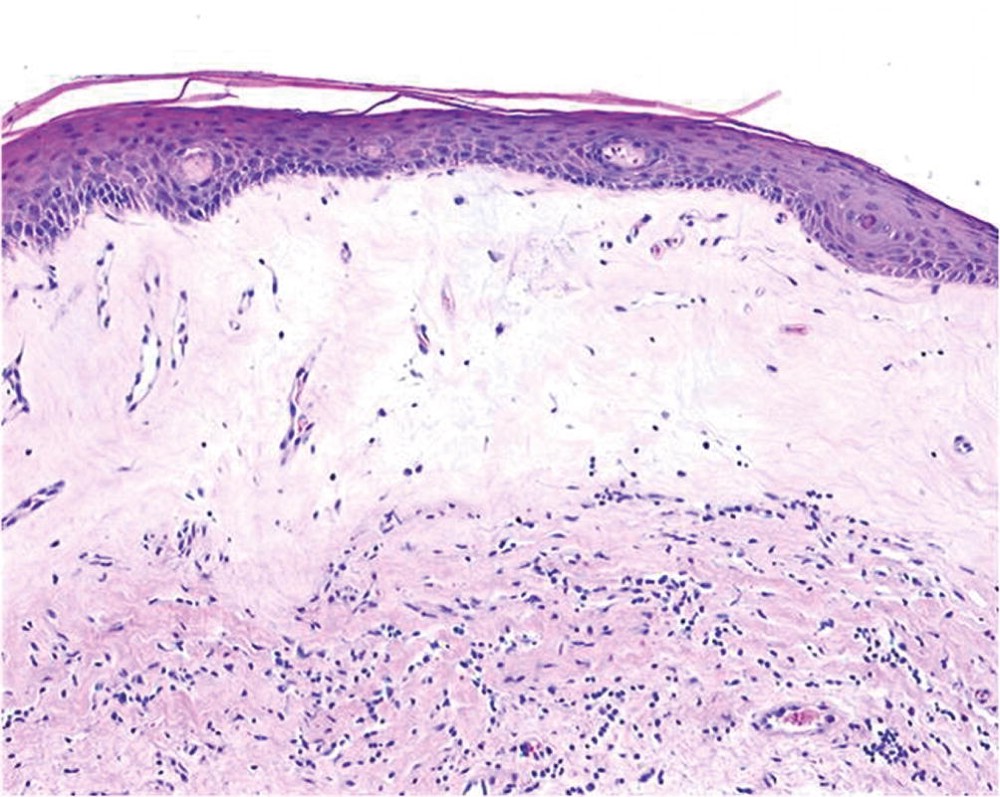
* histology:
* thinned epidermis with loss of normal rete pegs (???), basal layer vacuolar changes, paucity of melanocytes
* band-like lymphocytic infiltrate is often present
* dermis can show variable degrees of oedema, hyalinisation and fibrosis
* hyperkeratosis and follicular plugging can be present
* therapy and follow up:
* topical application of superpotent corticosteroid ointment (class 4), typically short term once daily
corticosteroids appear to decrease the anatomical changes but the influence on risk of malignant progression hasn’t been proven
* use of a skin moisturiser is also adviced on top of ^
* steroid resistant LS? → tacrolimus (anti inflammatory and immunomodulating effects)
* lidocaine or xylocaine cream or ointments can temporarily relieve pain; nocturnal itching can be treated with antihistamines and the use of lubricants to facilitate sexual intercourse is recommended
* since there is no ACTUAL cure, life long follow up and treatment is required
2. differentiated vulvar intraepithelial neoplasia:
* considered to be the precursor lesion of HPV-negative SCC
but the exact process of malignant transformation of LS to dVIN to SCC is not known
* incidence is unknown
* mainly occurs in postmenopausal women often in a background of LS
* different presentations, from grey-white discolorations with a roughened surface to ulcerative lesions unresponsive to intensified steroid treatment or raised white plaques
* diagnosis → punch biopsy for histological examination
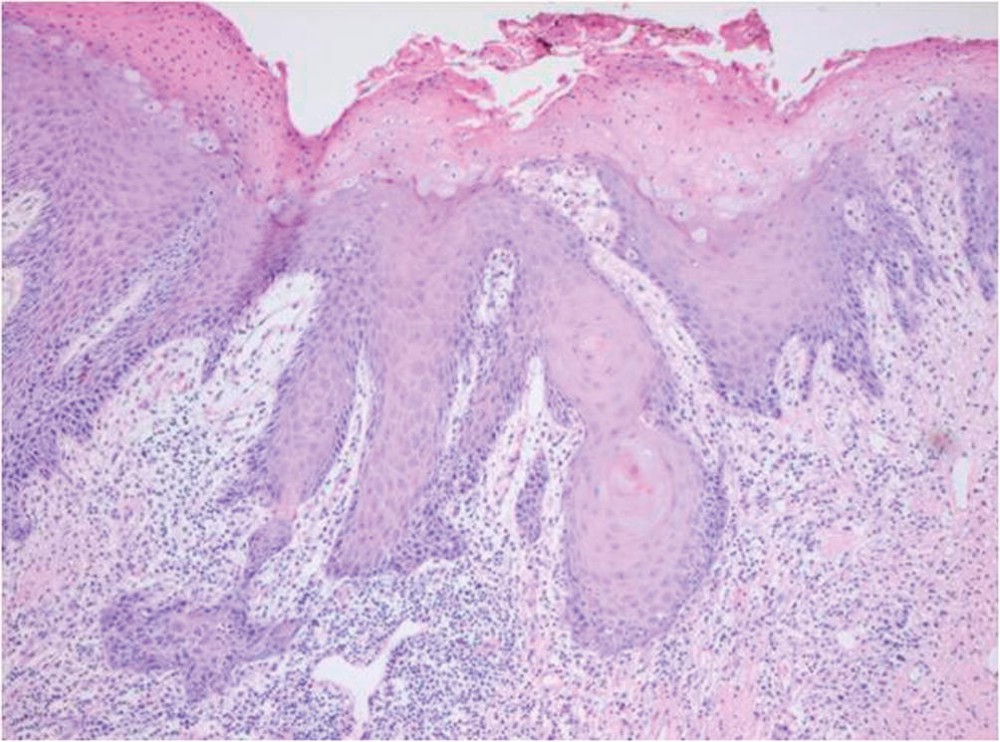
* histology:
* often mistaken for benign dermatosis due to subtle microscopic changes and high degree of differentiation or epithelial hyperplasia or reactive atypia
* atypia is ONLY in the basal and parabasal layers of the epithelium which have abundant cytoplasm → form abortive pearls (???)
* hyperkeratosis and parakeratosis are often seen
* superficial layers of the epithelium have normal maturation and there is NO koilocytosis (sign of HPV infection)
* epithelium exhibits elongation of rete pegs with prominent intercellular bridges, a result of loss of cohesion between cells
* characteristic → large amounts of intracytoplasmic keratin (= abnormal keratinocytes)
* nuclear changes of enlargement, pleomorphism, and hyperchromatism and mitoses
* chronic inflammatory cell infiltrate (same as LS) mainly lymphocytes, plasma cells and sometimes eosinophils
* dVIN lesions are often found ==__adjacent to vulvar SCC__== (but HSIL isnt???)
* *immunohistochemical stains (such as MIB1 or p53, which show different patterns in different entities) can help to differentiate between dVIN and normal vulvar epithelium or dVIN and HSIL*
* therapy and follow up:
* usually unifocal so after diagnosis surgery is advised to excise it and exclude invasive disease (goal is to have no residual disease)
* no systemic or topical medical therapy has proven effective
* close follow up is indicated
3. HSIL of the vulva:
* uncommon premalignant HPV induced skin disorder of the vulva
* mainly affects pre and perimenopausal women (so it can occur at any age but it mainly affects women < 50 y/o)
* used to be called bowens disease (isnt that in men now)
* incidence has increased more than 4x due to the increase in HPV infections
* caused by a persistent hr HPV infection (type 16 in 77%, followed by HPV 33 and 18)
* risk factors → smoking, history of anogenital warts and immunosuppression
* without treatment it can resolve spontaneously (< 2%, associated with younger age and pregnancy) or persist into invasive cancer
→ rate of malignant progression of HSIL is estimated to be 3-4% after treatment and 9% without treatment
what happened to the other 90% lol? just stays as HSIL?
* malignant progression is 50x higher in immunocompromised women
* mostly present with severe and long lasting vulvar complaints → pruritus, pain and dyspareunia → sexual dysfunction and psychological morbidity
* appearance varies but in 50% the lesions are multifocal
in multifocal lesions, the surrounding skin is usually clinically unaffected
* lesions can be elevated or flat, smooth or granular or verrucous surface, white or grey or red or pigmented
* vulvar HSIL is ==__associated with HPV-related disease of the cervix, vagina and anus in approximately 40%__== → regular gynaecological examination and cytological screening is recommended
* diagnosis → histology because there are ==__no certain clinical characteristics to exclude invasive growth__==
* *in case of multifocality or extensive disease, vulvar mapping with multiple biopsies should be performed. Lesions suspicious for malignancy, which do not respond to therapy or grow rapidly, should always be biopsied*
isnt it biopsied anyways???
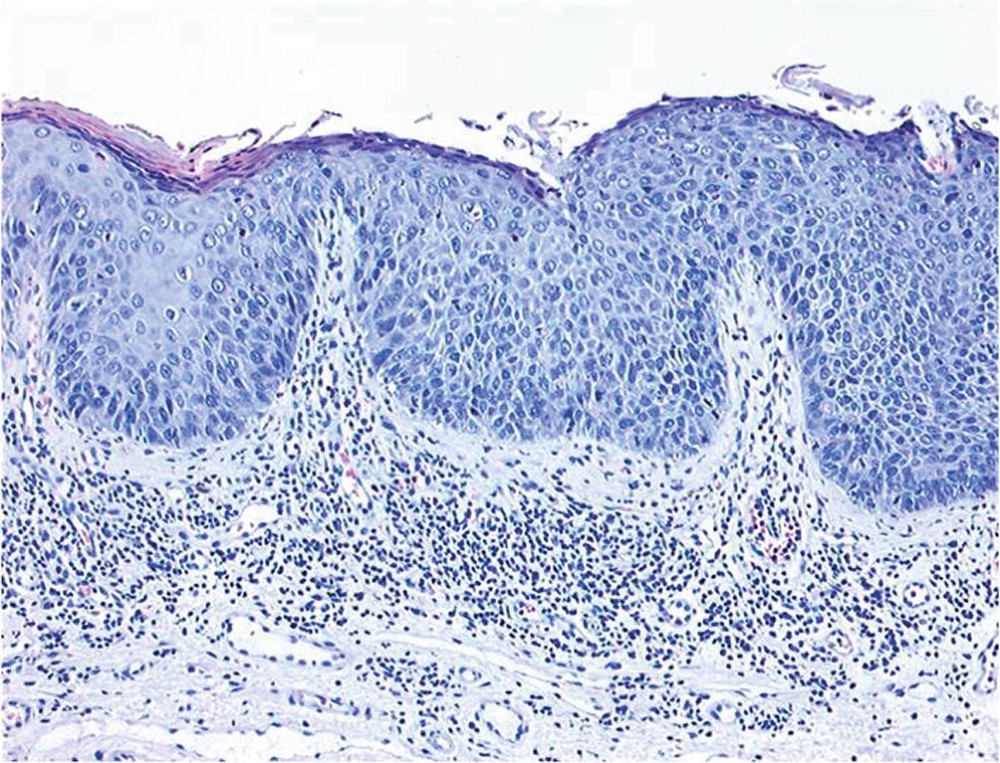
* histology:
* strongly resembles cervical intraepithelial neoplasia
* characterised by atypical cells with enlarged nuclei and mitotic activity + ==__loss of maturation in all layers of the epithelium__==
* classically, rete ridges are elongated and fused, and premature keratinization is often present
* most atypical cells are in the basal layer → irregular, enlarged nuclei and increased mitosis
* ==__P16 is a surrogate marker for high-risk HPV infections and therefore HSIL is often p16 positive, whereas most dVIN lesions are p16 negative__==
* p53 is negative in HSIL but not in most dVIN
* therapy and follow up:
* aimed at symptom relief and prevention of malignant progression
* invasive cancer suspected? → wide local excision even if biopsies show vulvar HSIL
* if invasion is not suspected → treat with topical imiquimod, surgical excision or laser ablation
* *prophylactic vaccination with the quadrivalent vaccine (HPV 6/11/16/18) has been shown to reduce the risk of HPV-related disease including vulvar HSIL*
\
1. medical treatment:
* imiquimod → effective in treating vulvar HSIL with complete responses in 50-60%
* local adverse events (pain, pruritus) are found in the majority of patients as well as systemic events in approximately one-third of them (headache, flu-like symptoms)
2. surgical treatment:
* cold knife surgical excision and CO2 laser vaporisation
* !! local excision has been the treatment of choice for unifocal lesions and in cases of suspicion for malignancy, but is suboptimal for treating multifocal lesions, which are common and more problematic, when invasion is not a concern
* so surgery might not be the best when multifocal or extensive
* some studies have shown higher recurrence rates after laser vaporization compared with surgical excision
4. Pagets disease of the vulva (adenocarcinoma, not squamous):
* rare, slow-growing, usually non-invasive neoplasm of the vulva
* most commonly seen in postmenopausal women (caucasian women >70 y/o)
* mammary pagets disease involves the breasts, extramammary pagets disease has a similar histology but affects the penis, scrotum and vulva
* risk of progression into invasive Paget’s disease seems to be small
* *vulvar Paget’s disease is reported to be associated with other malignancies of the breast (3.2% of patients), colorectal cancers (2% of patients), urological malignancies (4% of patients), and other gynaecological malignancies (2% of patients)*
* most patients present with non-specific symptoms such as itching, burning, or soreness
* lesions are often mistaken for eczema due to erythematous, scaling plaques and desquamation
* sometimes ulceration occurs
* may be extensive and even involve the inguinal folds and perianal region
* diagnosis → paget cells on histological examination
paget cells = large cells with clear cytoplasm and hyperchromatic nuclei, found throughout the epidermis
* *immunohistochemistry can distinguish vulvar Paget disease of a cutaneous origin from Pagetoid cells spreading from an internal malignancy. In general, vulvar Paget’s disease from a cutaneous origin is CK7 positive, and CK20 negative*
* !! the visual borders are often misleading because paget cells may spread along the basal layers of normal appearing skin
* usually treated by surgery but recurrence is common (35-60%)
* invasive vulvar Paget’s disease should be treated as a vulvar malignancy
4
New cards
histology slide of LS
5
New cards
histology slide of dVIN
6
New cards
histology slide of HSIL
7
New cards
SCC of the vulva
* rare
* more common in elderly women, median age of 68
* main route of spread is to the inguinofemoral lymph nodes
haematogenous and direct extension spread can occur but less frequently/more in advanced or recurrent disease
* clinical presentation and diagnostics:
* most present with vulvar mass, there is often a long history of itching associated with lichen sclerosus
* some present with vulvar bleeding, discharge, dysuria or a metastatic mass in the groin
* lesion may have a warty or ulcerating appearance
* !! things to keep in mind during PE → size of the lesion, unifocal or multifocal, distance to the midline, and does the tumour encroach critical midline structures (eg. clitoris, anus or urethra)
* size of the lesion, and whether or not the tumour is unifocal → determines if the patient might be suitable for the sentinel node procedure (why???)
* distance of the medial margin of tumour to the midline determines whether either ipsilateral or bilateral lymph drainage to the groin is to be expected = whether groin treatment should be ipsilateral or bilateral
eg. if within 1 cm from the midline, bilateral groin treatment is advised
* involvement of clitoris, anus, and/or urethra often means that these structures will need to be radically excised together with the primary tumour
* diagnosis → incision or punch biopsy for histology
* excision biopsy is NOT recommended because an accurate treatment plans, the localisation of the primary tumour is important as written above
* multiple lesions → each lesion should be biopsied separately with clear mapping of the vulva
* histology:
* since the most common subtype is HPV INDEPENDENT → typical differentiated keratinising SCC → differentiated cells with NO koilocytosis, frequently shows abundant keratin pearls, and often arises in a background of LS and dVIN
* the HPV dependent type is the warty or basaloid type
* warty type often exhibits keratinisation and prominent koilocytotic like changes
* basaloid type is composed of cells with scanty cytoplasm and little keratinisation
* both are found in the presence of HSIL
* P16INK4a is almost always positive in HPV dependent vulvar cancer (p53 is in HPV independent)
* lesions with a depth of invasion <1 mm require no groin treatment due to negligible risk of lymph node metastasis
* only 30% will have lymph node metastasis
* treatment and follow up:
* main is surgery (which type bruh this book is ASS)
1. sentinel node procedure:
* is included in the standard treatment of selected patients → those with unifocal primary SCC vulvar cancer with invasion >1 mm, smaller than 4cm, and without suspicious groin nodes
what if >4 cm??? never mind check the next bullet point lol
* only those with positive results have an indication for subsequent inguinofemoral lymphadenectomy
2. inguinofemoral lymphadenectomy:
* indicated in all patients with macroinvasive vulvar cancer, who do not meet the inclusion criteria of the sentinel node procedure
==__→__== eg. all primary tumours >4 cm, multifocal tumours, tumours <4 cm with proven lymph node metastasis and recurrent vulvar SCC without earlier inguinofemoral lymphadenectomy
* extent of the dissection is the inguinal ligament cephalad, the adductor longus muscle medially and the sartorius muscle inferolaterally
3. RT:
* indicated postop for those with more than 1 lymph node metastasis or in the presence of extranodal tumour growth
* in advanced → surgery is still the treatment of choice but definitive curative surgery in these cases is generally associated with significant morbidity, and not always possible
→ CT may be an alternative but everything is case by case
* recurrent disease:
* subdivided according to site → local recurrences (recurrences on the vulva), groin recurrences, and distant recurrences (includes pelvic recurrences)
can also occur in multiple sites
* local recurrence is a frequent event after primary treatment, and local recurrences can occur many years after primary treatment
* *many of these recurrences might be second primary tumours in a background of LS and dVIN or HSIL rather than a real recurrence, so called ‘de-novo’ tumours caused by field cancerization*
* local recurrences:
* treated with curative intent → wide local excision if possible
* if not possible → CT
* when local recurrences occur in patients with previously negative sentinel nodes, an elective inguinofemoral lymphadenectomy should be performed too
* groin recurrences:
* difficult to treat and often fatal
* occur mostly within the first 2 years after primary treatment
* preferably treated by debulking or inguinofemoral lymphadenectomy, followed by RT
* addition of CT can be considered in some cases (eg. can be primary CT if debulking is not possible)
* distant recurrences cannot be cured → palliative CT and/or RT
* more common in elderly women, median age of 68
* main route of spread is to the inguinofemoral lymph nodes
haematogenous and direct extension spread can occur but less frequently/more in advanced or recurrent disease
* clinical presentation and diagnostics:
* most present with vulvar mass, there is often a long history of itching associated with lichen sclerosus
* some present with vulvar bleeding, discharge, dysuria or a metastatic mass in the groin
* lesion may have a warty or ulcerating appearance
* !! things to keep in mind during PE → size of the lesion, unifocal or multifocal, distance to the midline, and does the tumour encroach critical midline structures (eg. clitoris, anus or urethra)
* size of the lesion, and whether or not the tumour is unifocal → determines if the patient might be suitable for the sentinel node procedure (why???)
* distance of the medial margin of tumour to the midline determines whether either ipsilateral or bilateral lymph drainage to the groin is to be expected = whether groin treatment should be ipsilateral or bilateral
eg. if within 1 cm from the midline, bilateral groin treatment is advised
* involvement of clitoris, anus, and/or urethra often means that these structures will need to be radically excised together with the primary tumour
* diagnosis → incision or punch biopsy for histology
* excision biopsy is NOT recommended because an accurate treatment plans, the localisation of the primary tumour is important as written above
* multiple lesions → each lesion should be biopsied separately with clear mapping of the vulva
* histology:
* since the most common subtype is HPV INDEPENDENT → typical differentiated keratinising SCC → differentiated cells with NO koilocytosis, frequently shows abundant keratin pearls, and often arises in a background of LS and dVIN
* the HPV dependent type is the warty or basaloid type
* warty type often exhibits keratinisation and prominent koilocytotic like changes
* basaloid type is composed of cells with scanty cytoplasm and little keratinisation
* both are found in the presence of HSIL
* P16INK4a is almost always positive in HPV dependent vulvar cancer (p53 is in HPV independent)
* lesions with a depth of invasion <1 mm require no groin treatment due to negligible risk of lymph node metastasis
* only 30% will have lymph node metastasis
* treatment and follow up:
* main is surgery (which type bruh this book is ASS)
1. sentinel node procedure:
* is included in the standard treatment of selected patients → those with unifocal primary SCC vulvar cancer with invasion >1 mm, smaller than 4cm, and without suspicious groin nodes
what if >4 cm??? never mind check the next bullet point lol
* only those with positive results have an indication for subsequent inguinofemoral lymphadenectomy
2. inguinofemoral lymphadenectomy:
* indicated in all patients with macroinvasive vulvar cancer, who do not meet the inclusion criteria of the sentinel node procedure
==__→__== eg. all primary tumours >4 cm, multifocal tumours, tumours <4 cm with proven lymph node metastasis and recurrent vulvar SCC without earlier inguinofemoral lymphadenectomy
* extent of the dissection is the inguinal ligament cephalad, the adductor longus muscle medially and the sartorius muscle inferolaterally
3. RT:
* indicated postop for those with more than 1 lymph node metastasis or in the presence of extranodal tumour growth
* in advanced → surgery is still the treatment of choice but definitive curative surgery in these cases is generally associated with significant morbidity, and not always possible
→ CT may be an alternative but everything is case by case
* recurrent disease:
* subdivided according to site → local recurrences (recurrences on the vulva), groin recurrences, and distant recurrences (includes pelvic recurrences)
can also occur in multiple sites
* local recurrence is a frequent event after primary treatment, and local recurrences can occur many years after primary treatment
* *many of these recurrences might be second primary tumours in a background of LS and dVIN or HSIL rather than a real recurrence, so called ‘de-novo’ tumours caused by field cancerization*
* local recurrences:
* treated with curative intent → wide local excision if possible
* if not possible → CT
* when local recurrences occur in patients with previously negative sentinel nodes, an elective inguinofemoral lymphadenectomy should be performed too
* groin recurrences:
* difficult to treat and often fatal
* occur mostly within the first 2 years after primary treatment
* preferably treated by debulking or inguinofemoral lymphadenectomy, followed by RT
* addition of CT can be considered in some cases (eg. can be primary CT if debulking is not possible)
* distant recurrences cannot be cured → palliative CT and/or RT
8
New cards
what is almost always positive in HPV dependent vulvar cancer
P16INK4a
(p53 is in HPV independent)
(p53 is in HPV independent)
9
New cards
other vulvar malignancies
1. basal cell carcinoma:
* 2nd most common vulvar malignancies (8%)
* about 2% of all BCCs are in the vulva
* median age of 75%
* unlike vulvar SCCs, they rarely metastasise → treatment is with wide local excision without groin surgery
* prognosis is very good
* apparently, the occurrence of BCC of the vulva does not affect survival
2. melanoma:
* 6% of all vulvar malignancies
* about 3-7% of all melanomas are in the vulva (this makes it a frequent site for extracutaneous melanomas)
* median age of 76
* *the 5-year survival rate was about 35 %, which was significantly lower compared with women with cutaneous melanomas: 50 % after matching for age, tumour ulceration, Breslow thickness, lymph node status and distant metastases*
* !! *cutaneous melanomas and vulvar melanomas appear to arise through a different oncogenic pathway because cutaneous melanomas are associated with sunlight exposure*
==__*NRAS and KIT*__== *mutations are more frequently found in vulvar melanomas compared with cutaneous melanomas*
* main treatment is surgery, there is no evidence of elective inguinofemoral lymphadenectomy
* sentinel lymph node procedure is used to obtain prognostic info but it doesnt show improvement in prognosis
* the premalignancy melanoma in situ is extremely rare (show it is immediately a cancer???)
\
* *Glandular vulvar malignancies are the less common epithelial vulvar malignancies. The most common and ambiguous term for a glandular vulvar malignancy is vulvar adenocarcinoma: invasive vulvar Paget disease and Bartholin’s gland tumours are the most common primary types.*
*Of all vulvar adenocarcinomas, about 45 % are secondary malignancies, most commonly caused by expansion, or recurrences of intestinal malignancies.*
*The 5-year survival of primary glandular vulva malignancies is about 70 %, which is comparable with the prognosis of vulvar SCC. Because the incidence of glandular malignancies is so low, histological samples should be reviewed by an expert gynaeco-pathologist and patients should be treated in specialized oncology centres*