Pathophysiology of Venous Thromboembolism
1/21
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
22 Terms
Secondary Hemostasis
Begins simultaneously with platelet plug formation - Process is slower (~minutes)
Initiated by internal and/or external vessel injury - platelets enhance activation of coagulation system which release and concentrate clotting factors and provide surface for clotting factors to assemble
Termed the “coagulation cascade”
Coagulation Cascade
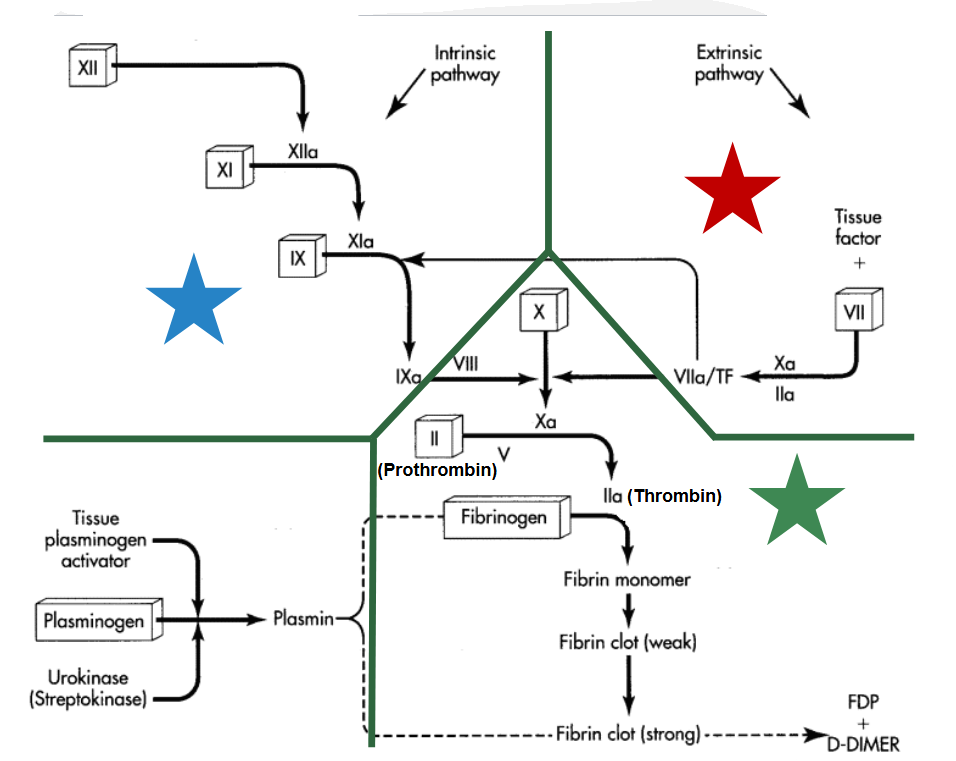
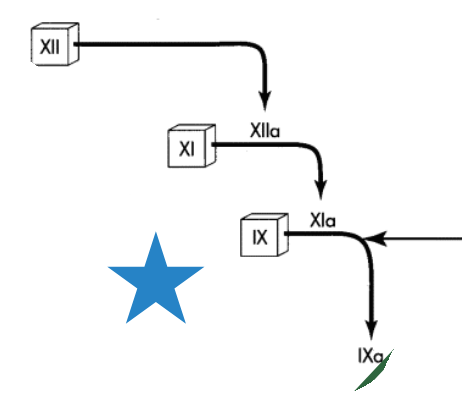
Intrinsic Pathway
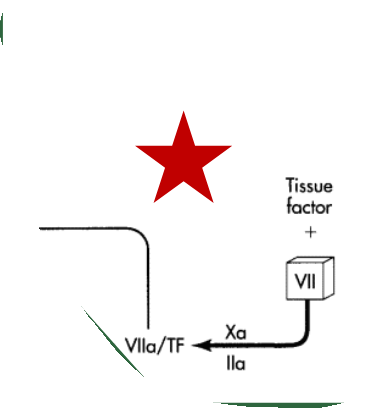
Extrinsic pathway
Common pathway
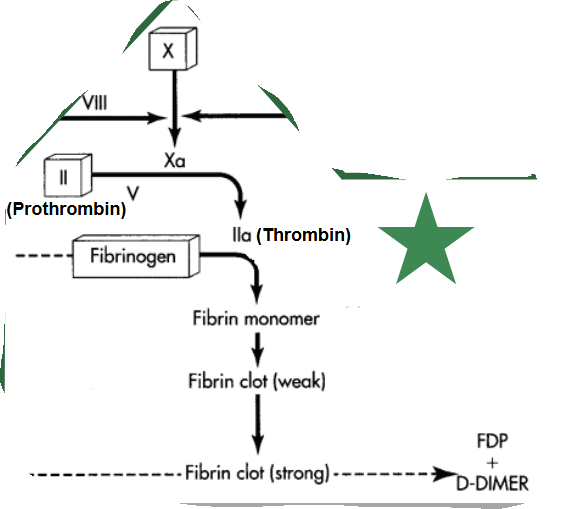
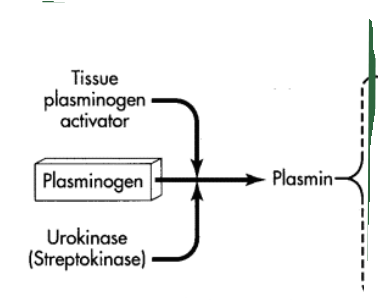
Fibrinolytic system
Virchow’s triad - Etiology
Thombosis is caused by 3 factors that enhance eachother:
Endothelial injury
Abnormal Blood flow - “stasis”
Hypercoagulability
Risk Factors for VTE
Age >40 Acquired (A)
History of VTE (A)
Risk Factors for VTE - Abnormal Blood Flow
Acute medical illness requiring hospitalization (T - transient)
Immobility (A/T)
Obesity (A/T)
Risk Factors for VTE - Endothelial Injury
Major orthopedic surgery (T)
Trauma (T)
Indwelling venous catheters (T)
Hypercoagulability
Malignancy (A)
Antiphospholipid antibodies (A)
Pregnancy (T)
Hormone therapy (T)
Protein C/S deficiency (I - inherited)
Antithrombin III deficiency (I)
Factor V Leiden (I)
Factor VIII/XI excess (I)
Deep Vein Thrombosis (DVT): Clinical Presentation
Signs/Symptoms - Leg edema, usually unilateral
Warmth, erythema/discoloration
Local tenderness or pain
Palpable cord
Homan’s sign
Some patients may be asymptomatic
Location of signs/symptoms may not be at location of thrombus
Pulmonary Embolism: Clinical Presentation
Chest Pain
Dyspnea
Tachypnea
Tachycardia
Hemoptysis
other s/s: cough/wheezing, calf/thigh pain, diaphoresis, fever, hypotension
Severe: cardiovascular collapse
Diagnosis of VTE: Overview
Patient scoring system - Well’s Score
Laboratory Marker - D-dimer
Diagnostic Imaging - DVT: Compression ultrasound (CUS) or venography
PE: computerized tomography pulmonary angiography (CTPA) or ventilation-perfusion (V/Q) scan
Hypercoagulable work-up
D-Dimer
Clot degradation product formed when cross-linked fibrin is lysed by plasmin
Levels are significantly elevated in patients with acute VTE - Reference “normal” value for most assays is <500 ng/mL
However, many non-VTE conditions associated with inc. d-dimer - Surgery/trauma, advanced age, pregnancy, cancer, etc.
Useful adjunctive test for patients with questionable VTE
An elevated (+) D-dimer, by itself, is not diagnostic for VTE
A normal (-) D-dimer can “rule out” an active thrombosis
Diagnostic Imaging for DVT: Compression Ultrasound
A probe placed on the skin uses soundwaves to visualize veins in the lower extremity
Pros: Non-invasive, Inexpensive, Can be performed at bedside, Sensitive to detect large thrombi that occlude proximal veins
Cons: Relatively insensitive to smaller, non-occlusive thrombi and calf vein thrombosis
First-line diagnostic test for DVT
Diagnostic Imaging DVT: Venography
Contrast dye is injected into the peripheral veins, providing visualization of the lower extremity venous system
Pros: Most definitive test to assess for thrombosis within the veins (“gold standard”)
Cons: Invasive (IV contrast), Expensive, Contrast may cause adverse effects
Rarely used in clinical practice
DVT Well’s Criteria
≤0 Low/unlikely 5%
1-2 Moderate 17%
≥3 High/likely 17-53%
PE Well’s Criteria
≤4 PE unlikely (rule out with D- Dimer)
≥5 PE likely (confirm with CT)
Diagnostic Imaging PE: Computerized Tomography Pulmonary Angiography (CTPA)
Uses CT scanning technology and contrast dye to visualize the pulmonary arteries
Pros: Increased sensitivity to detect emboli in smaller vessels, More widely available
Cons: Invasive (IV contrast), Higher doses of radiation (5x V/Q)
First-line diagnostic test in most patients
Diagnostic Imaging PE: Ventilation-Perfusion (V/Q) Scan
Radioactive tracers are inhaled (ventilation) then injected (perfusion) and a gamma camera visualizes airflow; mismatches (V>Q) indicate a blockage
Pros: Lower doses of radiation, No absolute contraindications
Cons: Invasive (radioactive tracer), Not widely available
Usually reserved for pregnant patients or those with contraindication to CTPA (e.g., contrast allergy, renal dysfunction)
Hypercoagulable Work-up
Indications: Idiopathic VTE or no overt risk factors, < 40 years old
Laboratory panel components: Antiphospholipid antibodies, Factor V Leiden, Protein C, Protein S, Antithrombin III