IMED1004 - Nutritional Guidelines (L10)
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
The Australian Dietary Guidelines are
evidence based
The evidence grading system assesses the literature on 5 outcomes
- Evidence Base: Type of Studies (case report, cohort, randomised control trial, metaanalysis, size of studies)
- Consistency: is the literature in agreement
- Clinical Impact: What impact does it have on morbidity - what do the studies show?
- Generalisability: which population was this research performed on? does it apply to australia
- Applicability: should this be applied to the Australian Dietary Guideline?
Challenges of Dietary Guidelines
- how can we do nutritional studies?
- can we suggest politically controversial things?
- do people take the advice away?
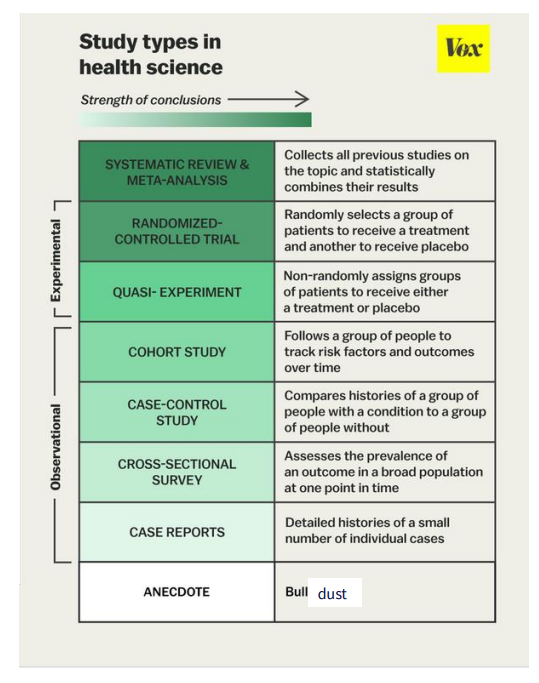
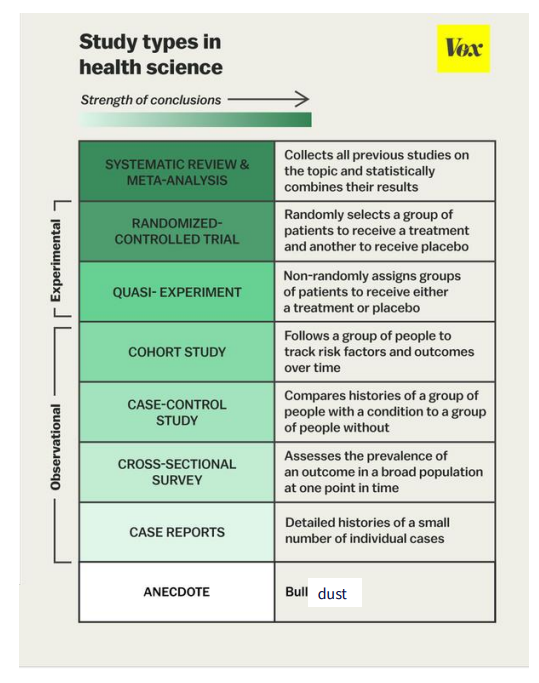
Study Types in Health Sciences
- Anecdote: e.g "my mum ate 3 punnets of strawberries a day and lived to 90 years old"
- Learning outcome says you dont need to know all the different types, just need to know that there are different studioes
- We have Observational which are ones where we don't change anyone's behaviour, we just observe what they're already doing
- We also have experimental, which are ones where we actually do a proper experiment like you would in the lab but with people where we actually have an intervention, where we change their behaviour
Challenges in Nutrition: scientific evidence
- "ideal" study would be randomised, controlled, double blind study and done over people's entire lifetime
- but this is not ethically possible
.
e.g feeding infant chicken nuggets for first half and broccoli for first half. not ethical
Main Challenges in Nutrition: scientific evidence
- Ethical considerations: can't prescribe some diets as "treatment"
- too many other confounding factors affect which "treatment" different individuals receieve
- Can't blind participants (people know what food they're eating most of the time)
- We don't just eat one food - what is the "treatment"
- What is the appropriate population to study? Generalisable?
Observational Studies
- we can do observational studies, usually involving large cohorts
- self reporting is unreliable
- No easy way to assess nutrient intake otherwise
- Can't control for other factors (e.g people say that people who eat fish live longer, so people think taht eating fish = longer life span. but it has been shown that since fish is expensive, higher income people eat fish and hence they can afford to see the doctor more hence they live longer)
Challenges in Nutrition: science doesn't exist in an ahistoric, apolitical vacuum
- The Australian government brought in plain packaging for tobacco in 2012 to discourage smoking
- The tobacco industry sued them, and Australian government legal fees against the tobacco industry case - $39 million
- if we tried to ban alcohol, it wouldnt work since a lot of bars depend on them to survive, and also it would be political outrage (so political reasons means that even thopugh we could ban alcohol and it would be better, we cant do it)
Challenges in nutrition: will people take the advice
A 2004 study found that only a third of middle aged Australian women achieved HALF of the dietary guidelines
Food is
- social, cultural, emotional, economic
- the dietary guidelines are an attempt to compromise between the science of nutrition and other kinds of facts about people
Nutritional research improves health
- folate supplementation prevents neural tube defects
- Trans fat is not good for heart disease
- increased sugar intake increases risk of diabetes, fatty liver disease (these are useful pieces of information whcih result in real changes in health outcomes)
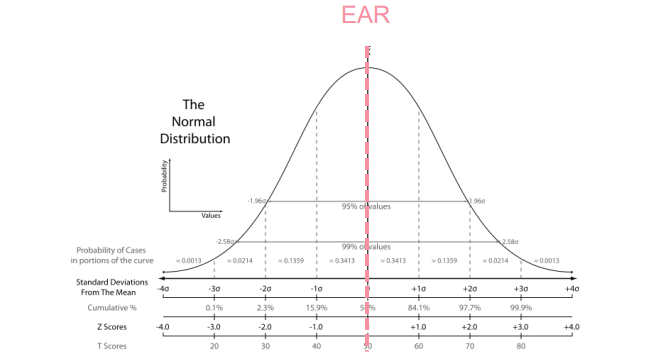
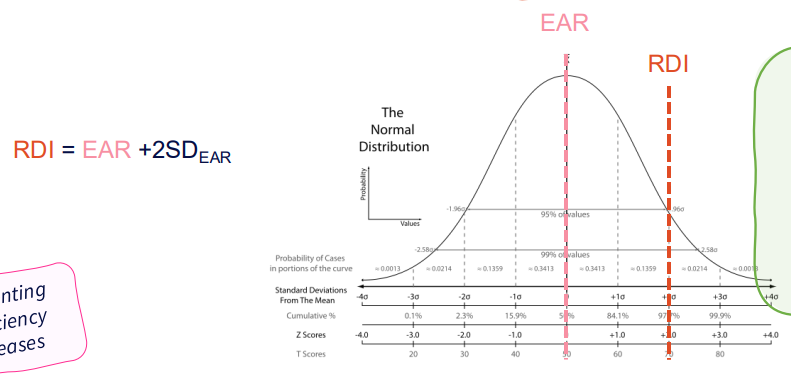
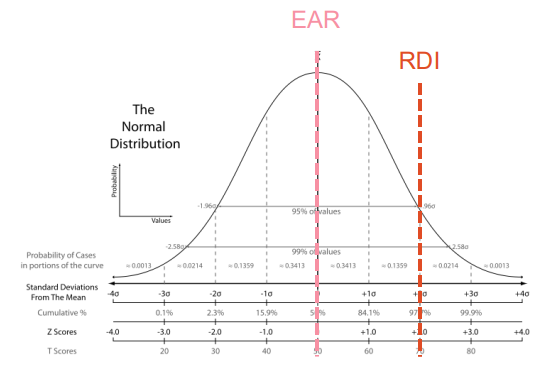
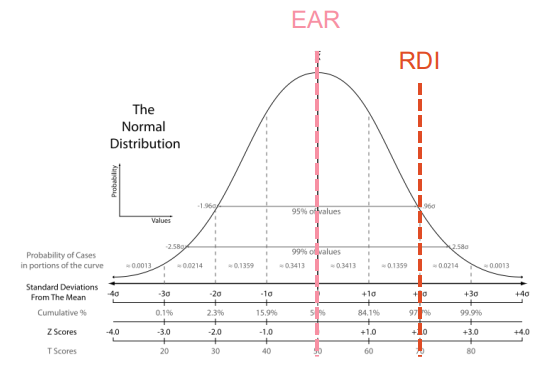
EAR - Estimated Average Requirement
- Nutrient Level required to meet the needs of approximately half the healthy individuals in a sex and particular life stage group
.
- we acknowledge that everyone has different nutritional requirements that are clustered around a mean. so if we take the mean and median the value of the median is going to be enough that half that half the populations needs are going to be
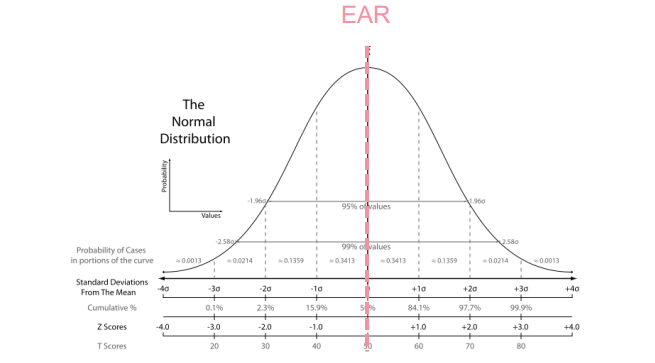
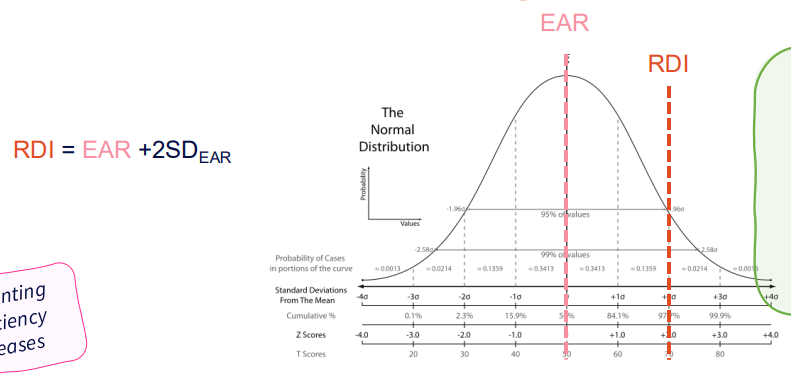
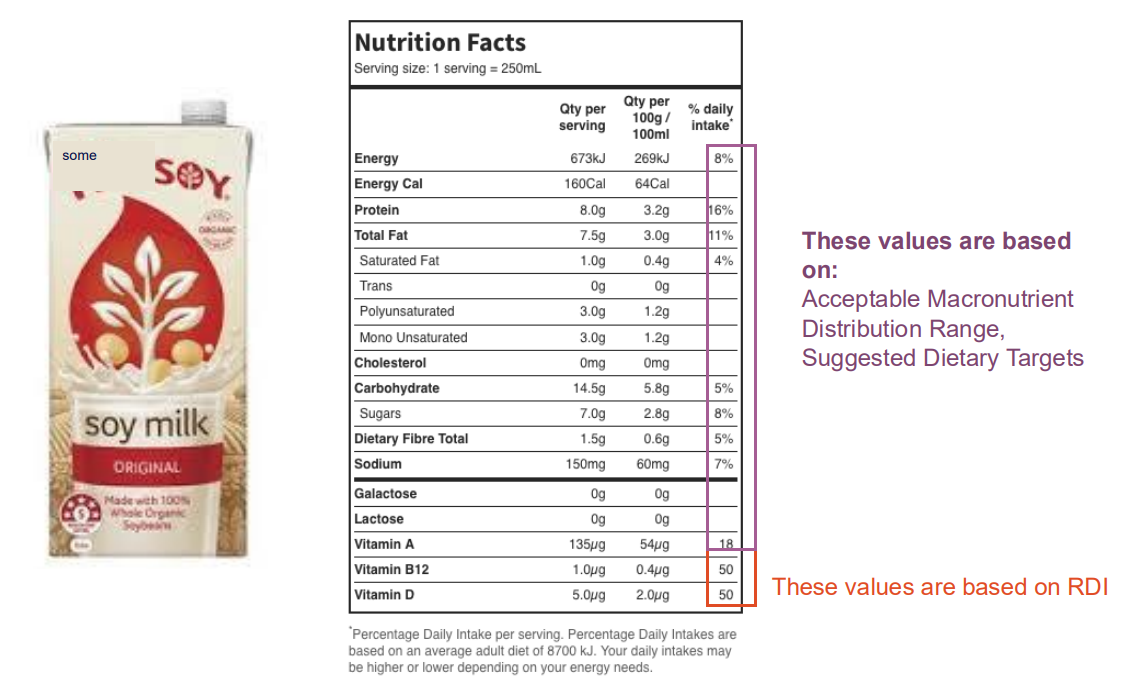
RDI - Recommended Daily Intake
- The average daily dietary intake level that is sufficient to meet the nutrient requirements of nearly all (97-98%) healthy individuals in a sex and particular life stage group
- RDIs exceed the actual nutrient requirements of practically all healthy persons and are not synonymous with individual requirements
.
- RDI = EAR + 2 Standard Deviations
- the interpretations: 97-98% of all individuals will have requirements below the RDI
- what this means is that most people actually need less then the RDI
- what that means is that if someone is consuming the RDI its likely that their particular needs have been met (unless their in that top 2%)
RDI = amount of nutrient sufficient for around 98% of people
- RDI takes into account differences between nutrient absorption in individuals
- But if I am average - I dont need that much to be healthy
- Consuming less then RDI doesn't necessarily mean that I am deficient
- we do know that if u consume the RDI, your nutritional needs have likely been met
Using NRVs: Populations vs Individuals
- its different for individuals and for groups
NRV: EAR (individual vs Group)
- Individual: use to examine the probability that usual intake is inadequate
- Group: use to estimate the prevalence of inadequate intakes within a group
NRV: RDI (Individual vs Group)
- Individual: usual intake at or above this level has a low probability of inadequacy
- Groups: do not use to assess intakes of groups
NRV: AI (Individual vs Group)
- individual: usual intake at or above this level has a low probability of inadequacy
- Groups: Mean usual intake at or above this level implies a low prevalence of inadequate intakes
NRV: UL (Individual vs Group)
- individual: usual intake above this level may place an individual at risk of adverse effects from excessive nutrient intake
- Groups: use to estimate the percentage of the population at potential risk of adverse effects from excessive nutrient intake
Adequate Intake (AI)
- when an EAR and RDI cannot be determined (insufficient evidence)
- AI is an estimate of the average nutrient intake of group(s) of apparently healthy people
Upper Level of Intake (UL)
- the highest average daily nutrient intake level likely to pose no adverse health effects to almost all individuals in the general population
- as intake increases above the UL, the potential risk of adverse effects increases
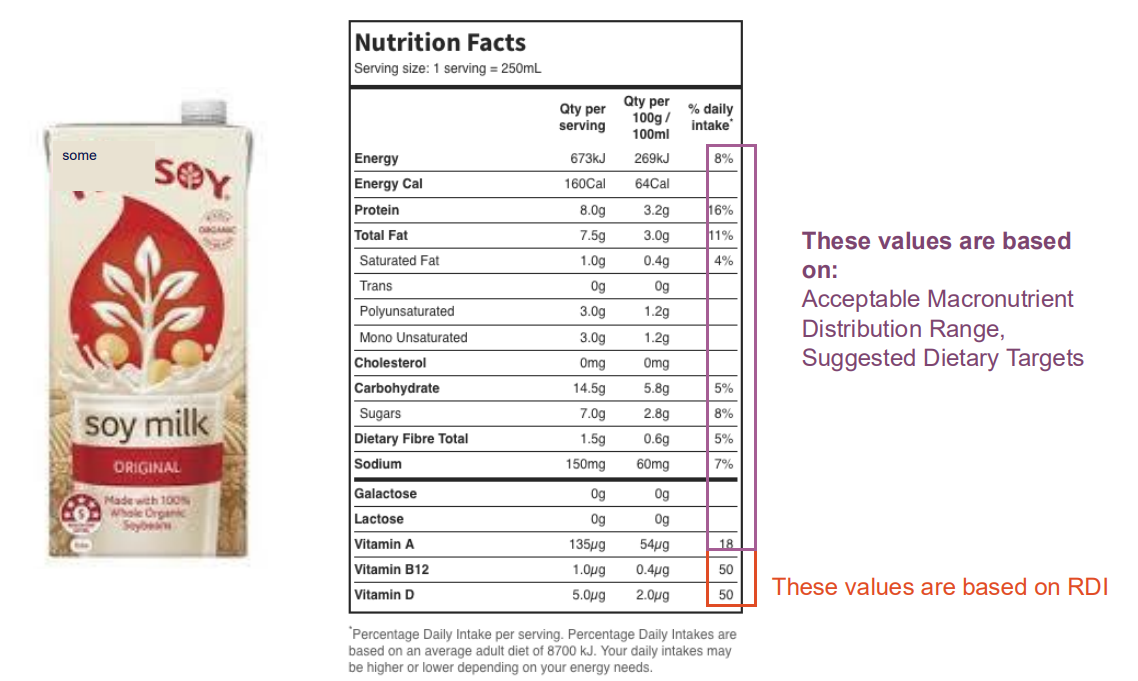
SDT - Suggested Dietary Target
- a daily average intake from food and beverages for certain nutrients that may help in prevention of chronic disease, at levels higher then the EAR or RDI
- average intake may be based on the mean or median depending on the nutrient and avialable data
Nutrients with SDTs (NAMING ONLY)
- Vitamin A, Vitamin C, Vitamin E, Selenium, Folate, Sodium/Potassium, Dietary Fibre, Long Chain Omega-3 Fats
- what this is saying is that some particular nutrients will have some relation to chronic diseases and usually this is defined quite discretely
Macronutrient Balance
- Macronutrients contribute to energy intake
- Need to satisfy both energy requirements and other nutritional requirements
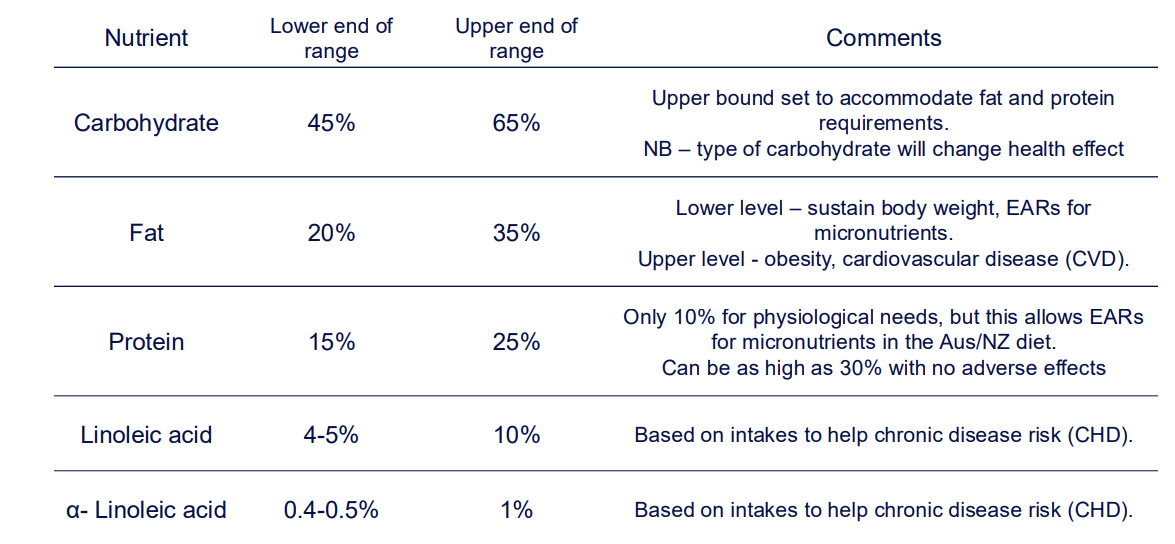
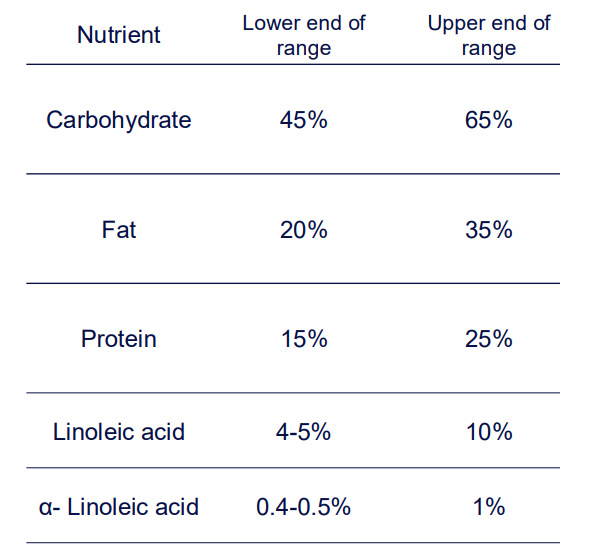
AMDR - Acceptable Macronutrient Distribution Range
- "The AMDR is an estimate of the range of intake for each macronutrient for individuals (expressed as per cent contribution to energy), which would allow for an adequate intake of all other nutrients whilst maximising general health outcome"
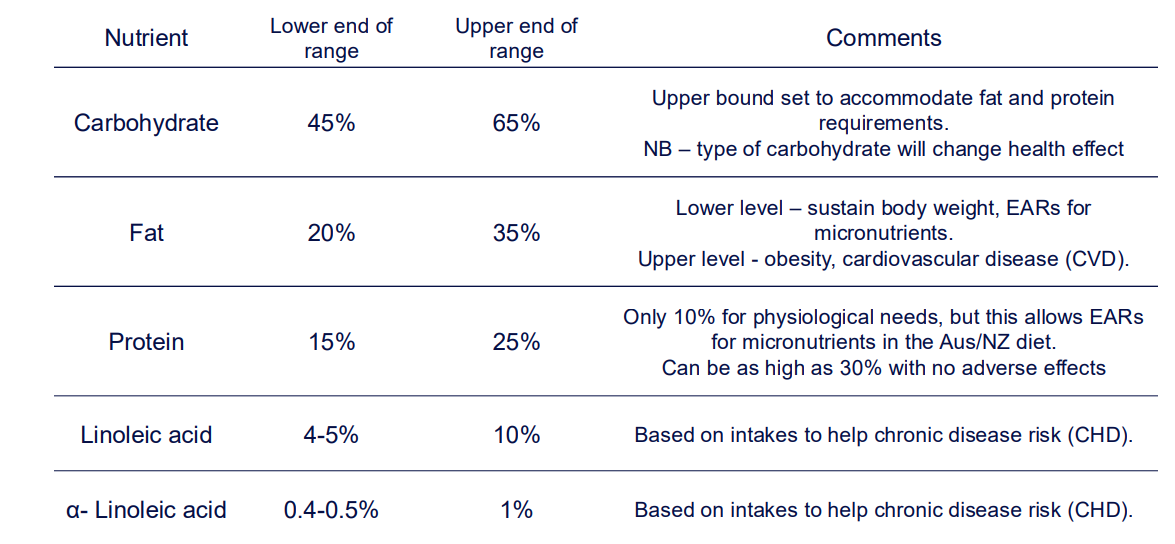
AMDR TABLE
DIAGRAM ON SLIDE 32
Remember
DIAGRAM ON SLIDE 34
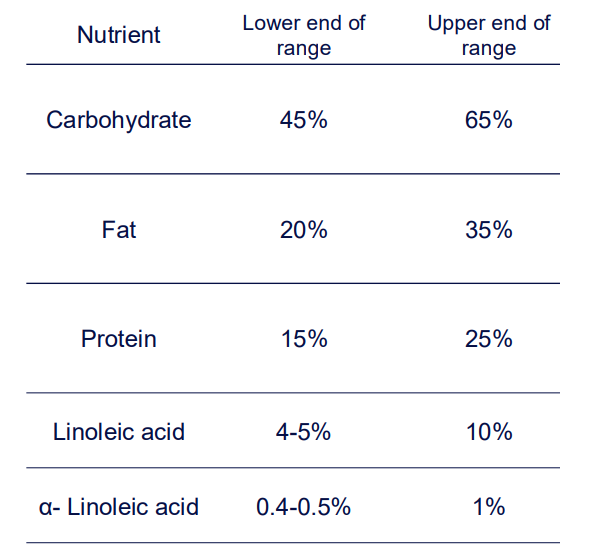
Macromolecule AMDR table
DIAGRAM ON SLIDE 33
RDI, EAR and AI as NRVs set to avoid _______
deficiency diseases
UL as NRVs is set to avoid _________
toxicity and adverse effects
SDT as NRVs to ________
- prevent/reduce chronic disease