General Principles of Exercise Rx for CRF
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
30 Terms
Exercise Rx: Purpose
-Designed to meet individual health and physical fitness goals
*health and PF can be very dif, so talk to patient what want to achieve (easier if understand goals and are motivated)
-This Class: Assist in the development of individually tailored Ex Rx for the “apparently healthy” adult whose goal is to improve physical fitness and health
FITT-VP principle of Ex Rx
-FITT-VP principle of Ex Rx
•Frequency (how often)
•Intensity (how hard)
•Time (duration or how long)
•Type (mode or what kind, ex: Type A,B,C)
•Total Volume (amount)
•Progression (advancement)
-Based on application of existing scientific evidence; Intended as guidelines for apparently healthy adults
Exercise Rx: How Plan
-Comprehensive (but also tailored) exercise program of aerobic and resistance training is important to improve and maintain physical fitness and health (*so start w/ health related components, decrease mortality)
•Health-related components of physical fitness in training regimen or exercise may vary among individuals (*ex goal: get 150 min/week)
-Exercise should be encouraged in inactive or deconditioned individuals (except where there are safety concerns) (*feels safe)
General Considerations for Exercise Rx: SMART Goal
-SMART: specific, measurable (like to see results), achievable, relevant, timely
-Individual goals (ex: lose weight, lower BP, better shape), physical ability, physical fitness, health status, schedule, physical and social environment, and available facilities and equipment
*how become active participants in health
A single exercise training session is typically composed of a…
•Warm-up / initiation
•Conditioning
•Cool-down
-Every session should be designed with a training goal in mind.
-Flexibility either before or after conditioning and/or separately (ex: cool down harder if have HD)
The Warm-Up
-Transitional phase: Allows body to adjust to changing physiologic, biomechanical, and bioenergetic demands of the specific exercise session
*increase HR, cardiac output, “prime the pump”, get moving
-Includes light-to-moderate intensity activities specific to the muscle groups that will be employed during exercise
-Improve ROM and may reduce the risk of injury (*bold statement)
-Dynamic warm-up involving large muscle groups superior to static flexibility
•Specific time may vary depending on the metabolic demands of the activity, but limited to less than 15 minutes
Conditioning Phase
-Training exercises include aerobic, resistance, flexibility, and/or sports activities, depending on the specific goals of the exercise session
-Duration between 10 and 60 minutes, depending on the intensity of the activity and goals
*”where is my bang for the buck?” what goal do I have?; consider intensity for patient (may be dif then us!)
The Cool Down
-Recent evidence suggests cool-downs have limited impact on improving psychobiological markers of recovery.
-The cool down may have added significance in clinical populations. (ex: diabetes benefit from cool down; improve exercise or post-exercise symptoms)
-May be useful to allow the body to return to near-resting levels (VO2 and HR)
-Low-to-moderate intensity flexibility exercises, such as static stretching, to help facilitate a more relaxed physiologic state
CRF: definition
-Capability of the heart, blood vessels, lungs, and skeletal muscles to transport and utilize oxygen to perform physical work
-Ex Rx of moderate-to-vigorous intensity continuous training of rhythmic, aerobic-type endurance exercise
*bc lower intensity= PA (don’t prescribe light exercise)
CRF Standard Recommendation
-All types and combinations of aerobic actives can contribute to meeting the PA recommendations, independent of improvements in CRF
-Standard recommendations of 150 mins/week may not be sufficient to improve CRF in large proportion of population
*but not enough for most students; vig means less minutes, but not for sedentary, start sedentary at moderate
*Picture : type=A,B,C,D; + vol, progression, deconditioning or regression
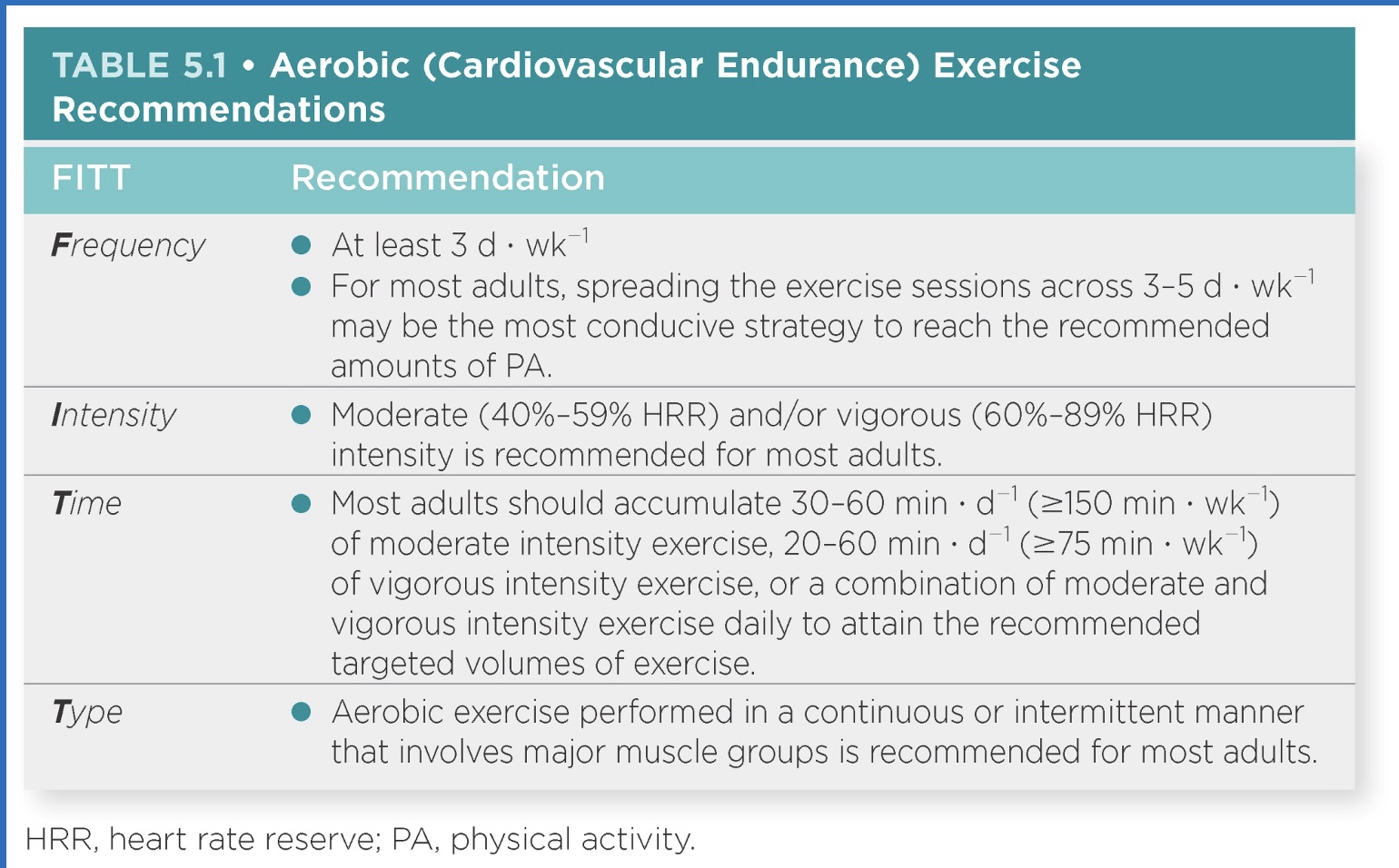
Frequency of Aerobic Exercise
*varies; 1) decrease mortality risk 2) increase fitness
-Spread exercise sessions over 3–5 d · w−1 (*if more active already)
-Frequency of exercise can vary, as can the intensity and duration, as these three variables are interdependent on each other.
-No conclusive evidence on best combination of frequency and duration
-Health and fitness benefits with 1–2 d · w−1 at moderate-to-vigorous intensity, particularly for deconditioned individuals (*to decrease mortality risk; if OW or do low levels of activity already)
Intensity of Aerobic Exercise: overview
*what patients struggle with the most!
-Positive dose response of health and fitness benefits from increasing exercise intensity
-Overload principle
•Minimum threshold seems to vary depending on an individual’s CRF level and other factors such as age, health status, physiologic differences, genetics, habitual physical activity, and social and psychological factors
which should you increase first: intensity, frequency, or time?
1) time
2) frequency
3) intensity
Intensity of Aerobic Exercise: Defining exact threshold (how many METS or HR= moderate or vigorous?)
-Precisely defining an exact threshold to improve CRF may be difficult
-Vigorous intensity exercise (>6 METs; 60%-80% HRR) is more effective at increasing VO2 (and CRF) than moderate intensity (3.0-5.9 METs; 40-59% HRR).
-Must consider subjects health and readiness.
*exceed 80%: “intense exercise” or “near maximal execise”
*mod: duration could extend exercise for longer time (not greater than OBLA, but x3 rest; athletes likely have higher OBLA)
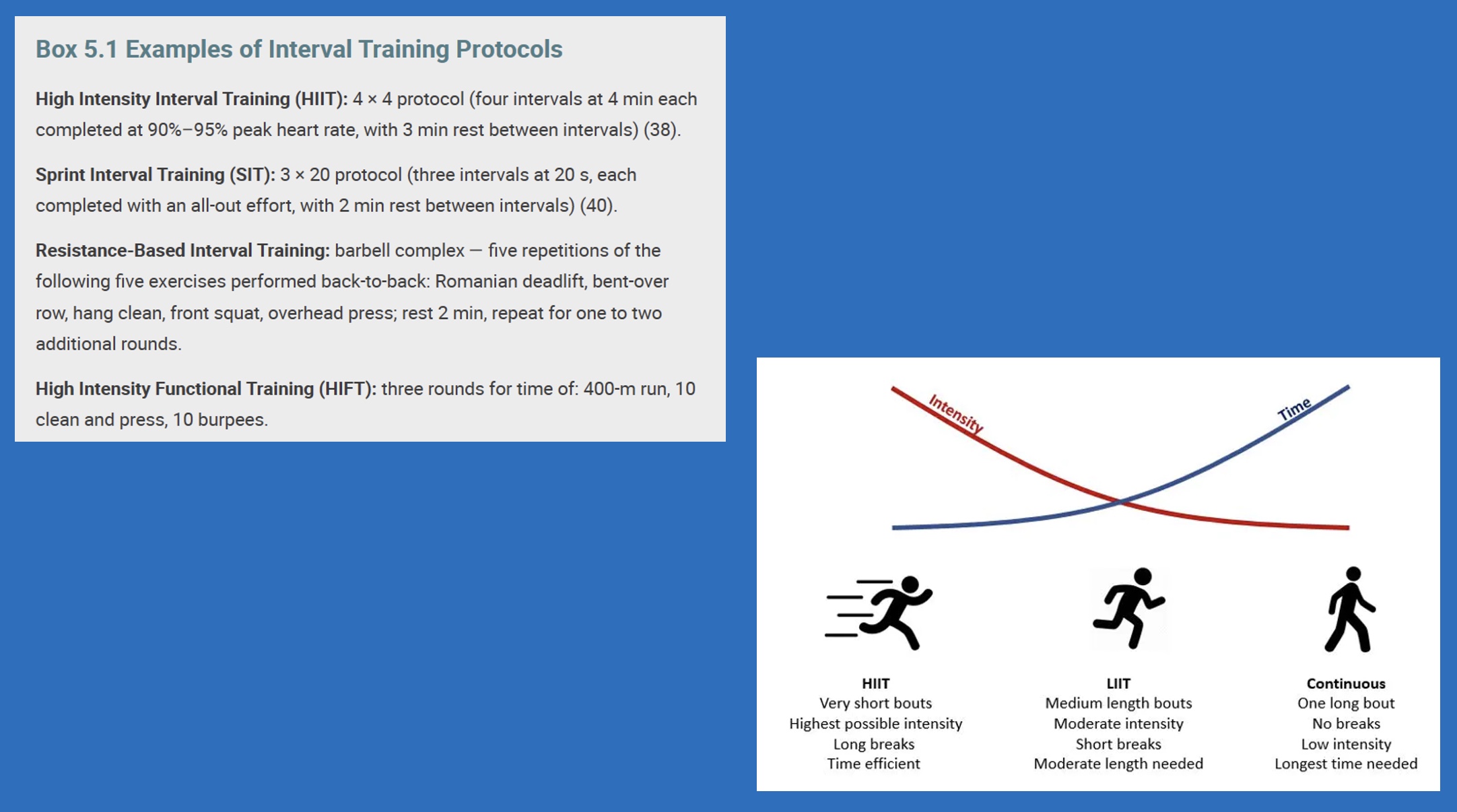
Intensity of Aerobic Exercise: Interval Training (definition, benefits, examples)
-Interval training: alternating bouts of vigorous-to-supramaximal intensity exercise followed bouts of light-to-moderate intensity exercise.
*don’t initiate with, start later on in program; good for kids; do high intensity then rest and repeat
-Elicits physiologic adaptations (CRF) similar to traditional endurance training despite a lower total workload (reduced total volume and time); And superior physiologic adaptations when total exercise dose is matched
Examples
-High intensity interval training (HIIT) or sprint interval training (SIT)
•HIIT: ≥80%-100% peak HR; SIT: ≥100% VO2peak
-Resistance-based interval training via a combination of body weight exercises, plyometrics, and resistance training equipment
Estimating Intensity (gold standard?)
-Determined by various factors: age, habitual PA level, physical fitness level, and health status
-Preferred method for Ex Rx: direct measurement of the physiologic responses to exercise through a GXT= “Graded Exercise Test” (max test; gold standard as know true HR and VO2)
•Ex Rxs based on intensity produce more predictable metabolic responses compared to Ex Rxs based on maximal fixed or predicted variables (i.e., HRmax)
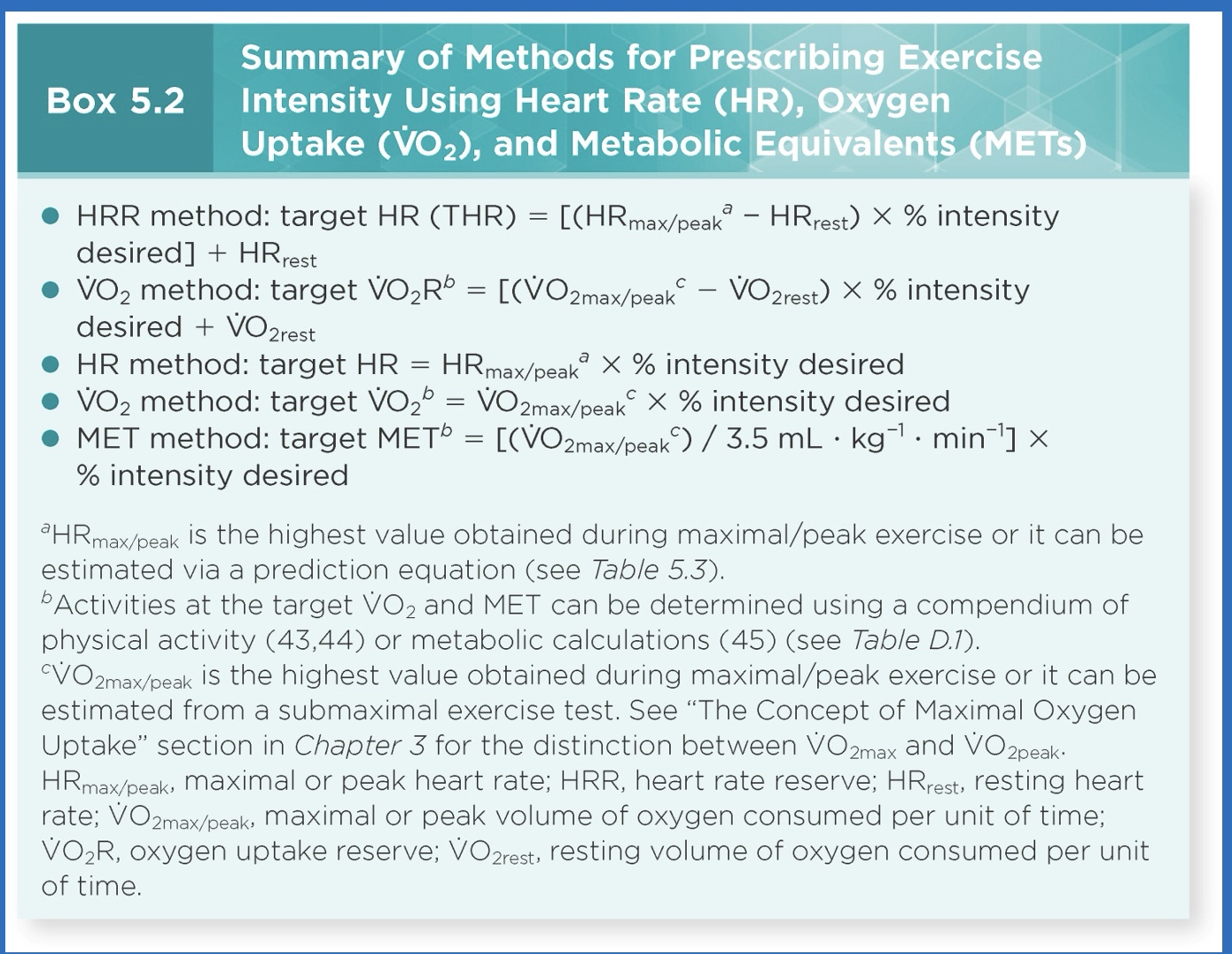
5 common equation estimates for intensity
-First 2= most common, and prob more accurate; take into account resting (so get reserve) and fitness
-Don’t use MET much anymore (has charts)
how do you find estimated HR max?
220-age
Methods of Estimating Absolute Intensity
-Metabolic equivalents (METs) (*not used much anymore, makes no sense to patient)
-Caloric expenditure (kcal · min−1)
-Absolute oxygen uptake (VO2; mL ∙ min−1 or L ∙ min−1)
•Can result in measurement error and misclassification of intensity because no consideration of individual factors (body weight, sex, and fitness level)
•Relative measures of intensity are more appropriate
how get from METs to lb of fat?
*how can prescribe exercise
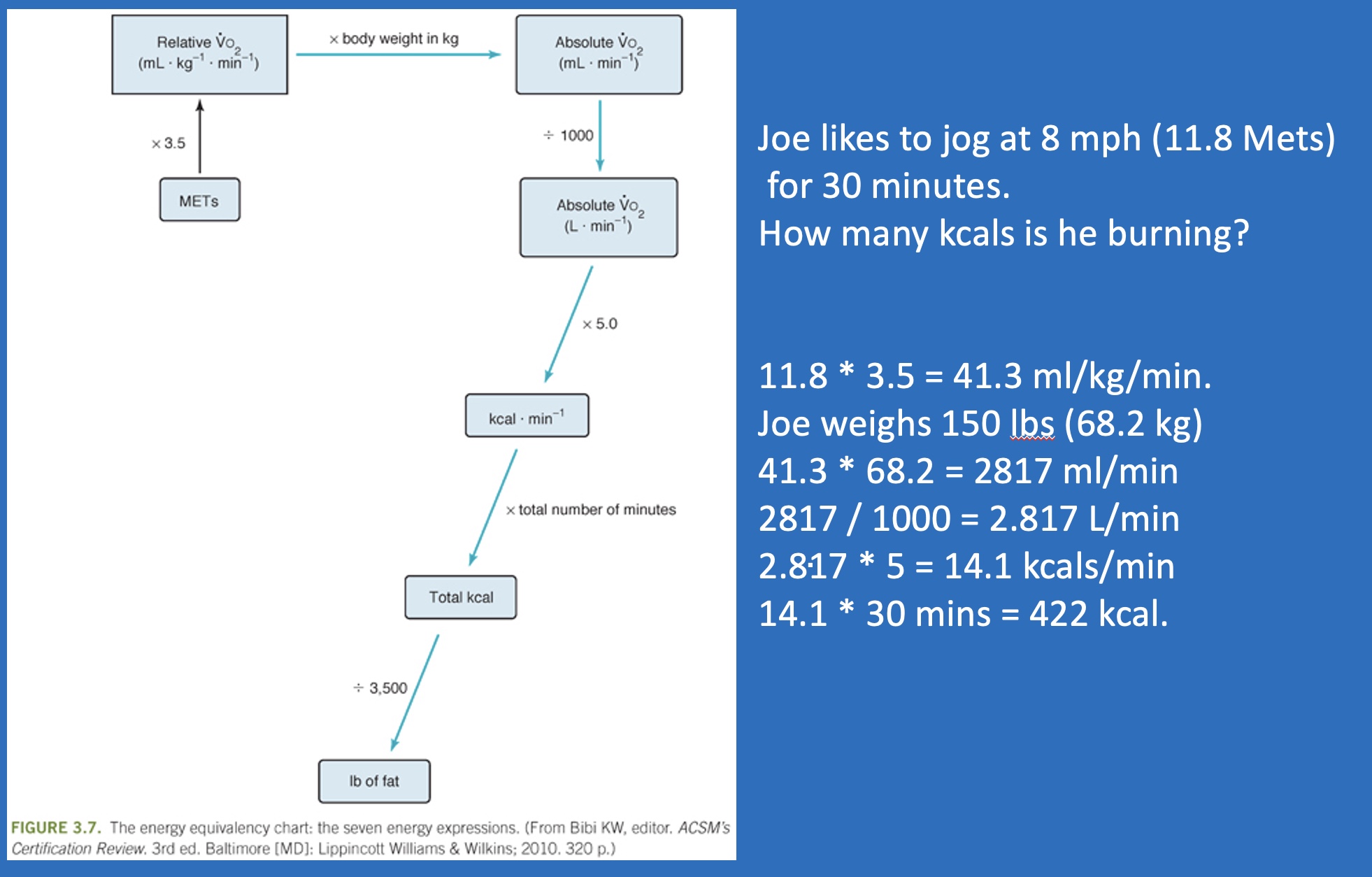
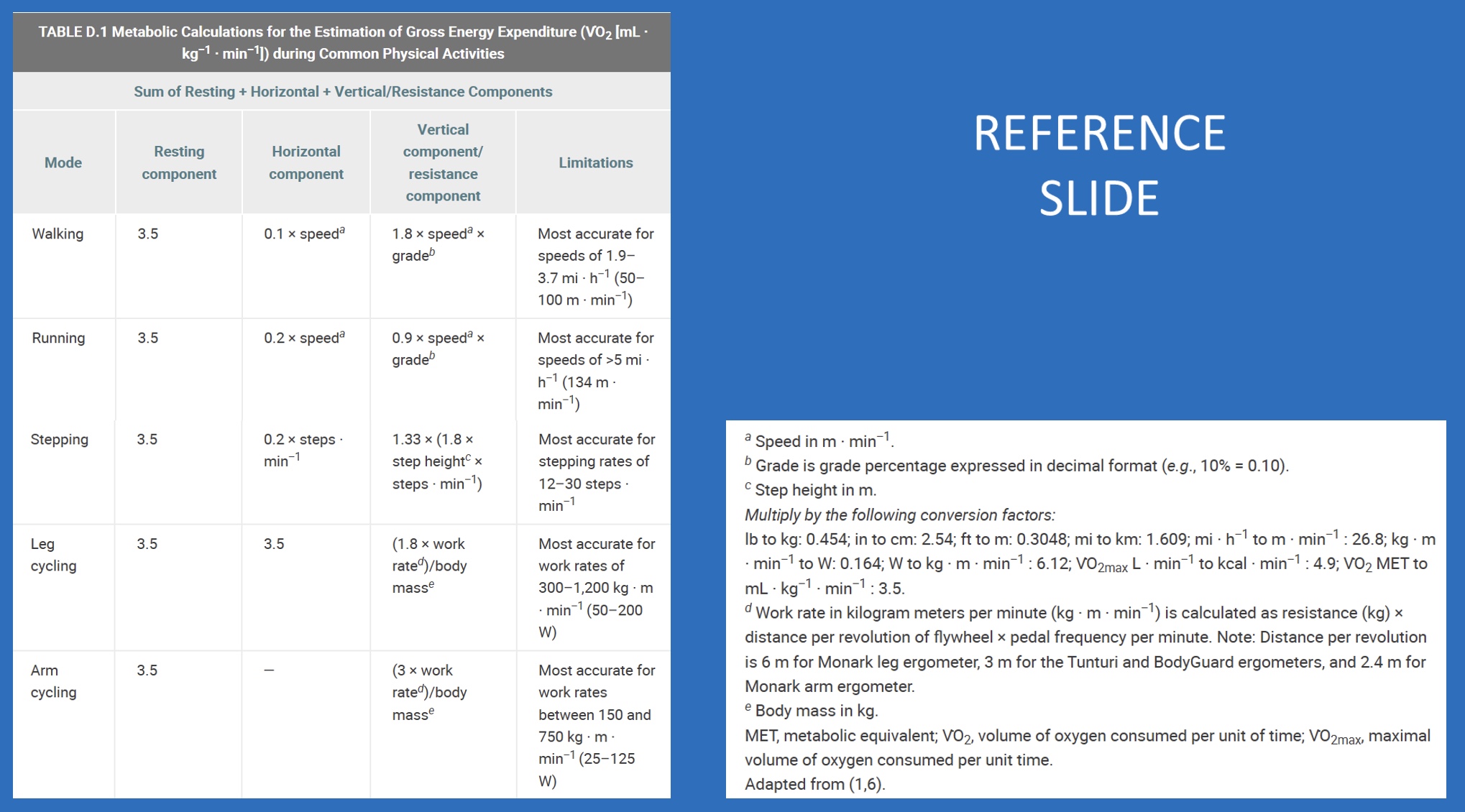
Reminder of ACSM equations
*don’t have to memorize, but know how to use!
Subjective Methods for Estimating Intensity
-Talk Test
•Moderate intensity: individual is able to talk but not sing
•Vigorous intensity: individual is not able to say more than a few words without pausing for breath
-Borg’s RPE Scale (6 to 20)
-Borg’s Category Ratio Scale (CR-10)
•0 to 10
•Moderate intensity: CR 5 to 6
•Vigorous intensity: CR 7-8
Aerobic Exercise Time
-Prescribed as the amount of time PA is performed (*think long term; can get in dif ways)
-Recommendations: 30–60 min ∙ d−1 (≥150 min ∙ wk−1) of moderate intensity exercise, 20–60 min ∙ d−1 (≥75 min ∙ wk−1) of vigorous exercise, or a combination of moderate and vigorous exercise per day
-General guideline for aerobic Ex Rx: 2 minutes of moderate intensity aerobic exercise is equivalent to 1 minute of vigorous intensity aerobic exercise
*2:1 ratio; 1 if limited in time and not at risk, like athletes
Aerobic Exercise Time: Continuous
-May be performed continuously (one session) or intermittently and accumulated over the course of a day in one or more sessions of physical activity that total at least 10 min ∙ session−1
*ex: interval trainging; seperate sessions if needed/can’t handle intensity well
-Exercise bouts of less than 10 minutes are associated with favorable health-related outcomes
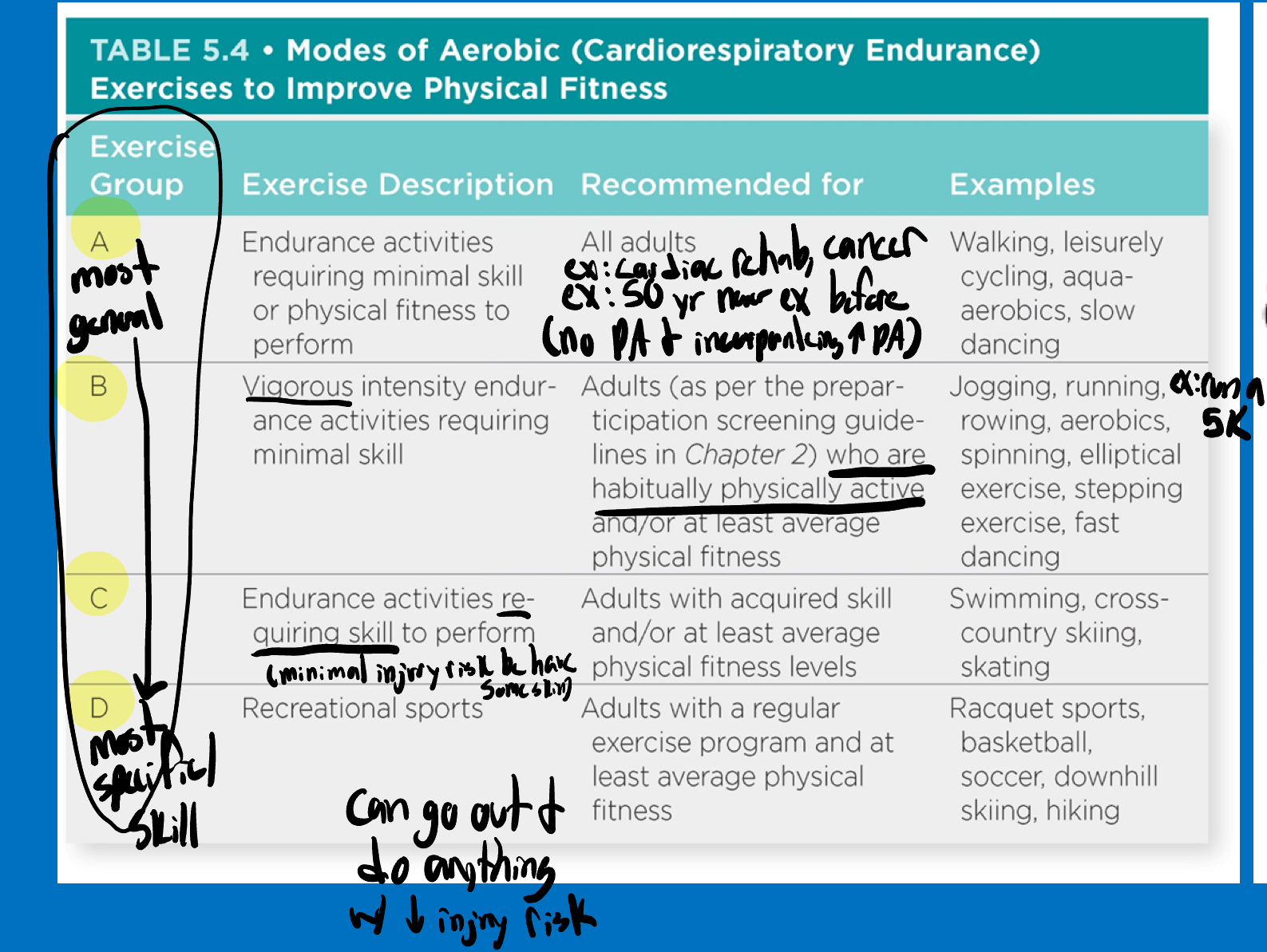
Aerobic Exercise Type/Mode
Type A/most general <-> Type D/most specific/skill required
-Type A: adults, if just doing PA for first time, no skill required
-Type B: vigorous, for those who habitually do PA
-Type C: those with some skills
-Type D: can go out and do anything with out injury risk
Aerobic Exercise: Volume (overview)
*think of patient burden! (realistic?)
-Product of Frequency, Intensity, and Time
-Used to estimate the gross energy expenditure (EE) of an individual’s Ex Rx
-MET-min ∙ wk−1 and kcal ∙ wk−1
Aerobic Exercise Volume (specifics)
-Dose-response association between the volume of exercise and health and fitness outcomes (*more appropriate levels= higher health benefits)
-No clear minimum or maximum (*people all enter at dif spots)
-1,000 kcal ∙ wk−1 of moderate intensity PA (~150 min ∙ wk−1)
*equal to Total EE of ≥500–1,000 MET-min ∙ wk−1 is consistently associated with lower rates of CVD and premature mortality; Exercise intensity of 3-5.9 METs (for individuals weighing ~150-200 lb); 10 MET-h ∙ wk−1
Aerobic Exercise Volume: pedometers
-Pedometers are effective tools for promoting physical activity and can be used to approximate exercise volume in steps per day.
(Achieving a pedometer step count of at least 7,000–8,000 steps · d−1, with at least 3,000 steps at a brisk pace (>100 steps · min−1), is a reasonable minimum daily threshold associated with health benefits)
Aerobic Exercise Progression (overview)
-Rate depends on the individual’s health status, physical fitness, training responses, and exercise program goals
-Increase any of the components of the FITT principle of Ex Rx as tolerated by the individual
Aerobic Exercise Progression (quote + specifics time frame of progression)
-Initial phase of the exercise program: principle of “start low and go slow”
*want them to climitize, but can lead to bordem or no results
*1) are they gaining the benefits they want to gain? 2) habituate them to PA, and then work towards their goal (ex: weight loss)
-An increase in exercise time per session of 5–10 minutes every 1–2 weeks over the first 4–6 weeks of an exercise training program is reasonable for the average adult.
-After the individual has been exercising regularly for at least 1 month, the FIT of exercise is gradually adjusted upward over the next 4–8 months or longer for older adults and very deconditioned individuals.