Coronary cardiovascular
1/80
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
81 Terms
Systole
Contraction of the ventricles
three layers of blood vessels from outside to inside
three layers of blood vessels from outside to inside
tunica externa:outermost layer, contains collagen fibers
tunica media: middletunic, smooth muscles
tunica intima: endothelium, innermost layer
Nameof vessel supplying blood to larger vessel
Vasa vasorum
Types of blood capillaries
Continuous - gas exchange, found in brain, testes, lungs, etc most common
Fenestrated - active filtration and absorption found in gi and kidneys
Sinusoid- most permeable found in liver, spleen, lymphnodes bone marrow
Vessels hold up to X amount lf blood volume at one time
65%
To be noted when taking oulse
Rate, rhythm, force/volume, does it match heart rate
Major long term bp is controlled by X
Kidneys
Condition in which blood vessel are inadequately filled and blood cannot circulate normally
Circulatory shock
What arteries branch from the celiac trunk
Common hepatic, left gastric and splenic
Superior vena cava is formed by which veins
Left and right braciocephalic
Longest vein and longest nerve
Great saphenous, sciatic
A thrombus in the first branch of the aorta would affect blood flow to the …
R side head and neck and right upper arm
Map calculation
Mean arterial pressure = cardiac output (bpm x ml ejected per beat (stroke volume)) X total peripheral resistance
Stroke volume calculation
End diastolic volume - end systolic volume
What effects stroke volume
Contractility (SNS increasing calcium)
Venous return
Blood amount
Blood pressure e.g. venoconstriction
Frank starling law (higher ventricle stretch = greater ejection
What is ejection fraction
Amount of end diastolic blood ejected during systole (percentage ejected)
What is total peripheral resistance
Diameter of vessel which creates pressure (sum of total resistance in all blood vessels)
What causes total peripheral resistance
Thickness of blood
Blood vessel diameter
Blood vessel length
How does the sns increase stroke volume
Increase power of contraction through extra calcium channels
Vasoconstriction
What are baroreceptors
Stretch receptors in the aortic arch and carotid artery (in carotid sinus) which send notification to medulla for activate autonomic nervous system
What js RR interval and what should be noted
Space between peaks of QRS to show time between contractions
Is it narrow or protracted?
Delays of conduction (scarring, abnormal pathways, age)
How long should atrial depolarisation take
Wothin 3 small squares = <120 milsec
Size of QRS complex
70-100miliseconds or 2 - 2 ½ mini squares
What is PR interval
120-200 ms or 3-5 small squares, has it been a clean and rapid movement or delayed
How to tell the time of a 6 second ecg strip
5 large boxes = 1 second
(times amount if complexes on total strip by 6)
What might signal reduced cardiac output to the body
Impaired perfusion and oxygenation
tachycardia racing pulse, confusion
tachyponeic, fast breathing, i.paired speaking
hypoxia e.g cold hands, weak pulses
Reduced blood to meet body demands
tight feeling chest
Poor activity tolerance
Possible symcope
Fluid imbalance
Nutritional and fluid imbalance
Oedema, improper pumping causing oedema as blood and fluid sits
Loss of appetite (blood diverted to more vital organs)
What actions could be taken for a patient with reduced cardiac output- vital signs
Regular vital signs, if radial pulse is thready due to limited blood output, heart sounds should be auscultated on the left strenal border 4th intercostal space, compare to radial pulse for 1 minute
What actions could be taken for a patient with reduced cardiac output - peripheral perfusion
Colour and warmth, cap refill, assess oedema, daily weight and FBC
Monitor BP manually if machine cant read, orthostatic readings
What actions could be taken for a patient with reduced cardiac output- lung and general care
Position semifowlers,
Medication safety, before and afters of medications i.e. sotolol and digoxin (hr and bp before)
Assess for bleeding especially if on blood thinners
Assess for orthopnea and breath sounds, work of breathing, paroxysmal nocturnal dyspnoea (legs raised during sleep to drain fluid, can put sudden strain on heart and cause palpitations, need increased oxygen)
Possible fall risk on standing, orthostatic bp,
Staging activity to reduce risk of fatigue, cluster care
Assess for ankle or sacral swelling
What is coronary beart disease or coronary artery diseas
Caused by impaired blood flow to the myocardium often by build up of atherosclerotic plaque in the coronary arteries
Common symptos or effects of coronary artery disease/ coronary heart disease/ischemic heart disease
Angina pectoris
Acute Coronary syndrome
Myocardial infarction
Arrhythmias
Heart failure
Sudden death
What affects the coronary circulation
Aortic pressure
Heart rate
Metabolic activity
Tone of the blood vessel
Collateral circulation
Which coronary artery supplies SA node
Right coronary artery, sudden occlusion of arrhythmias and sudden cardiac death
What is the internal lining of an artery and why is this important for atherosclerosis
Intimal layer,
Plaque forms from triglycerides, ldl, etc debris of collagen/smooth muscle cells/phospholipids within this layer and creates narrowing of lumen
calcifies to tear lining of artery causing bleeding of vessel and clot occludes or thrombus
What is angina pectoris and rreatment
Characterised by chest pain usually at exercise and relieved by rest. Mddications such as GTN which dialates artery
Occurs when the myocardial oxygen needs are greater than the partially occluded vessels and myocardial cells become ischemic
Anaerobic metabolism produces lactic acid that stinulates nerve endings causing oain, pain subsides when oxygen supply meets demand
What is an MI and possible treatments
Complete obstruction of coronary artery interrupting blood supply to area of myocardium
Clot disolving drug to break it up
Angioplasty to stretch narrowing with balloon and clot removal and perhaps stent
What is vasospasm
Symptoms of MI
CRUSHING AND SEVERE chest pain
TIGHT BURNING PRESSURE
Fever, hypotension(later stages)/hypertension (Initially)
Unlike normal angina
Sudden onset, not necessarily provoked
Lasts more than 15 minutes
Not relieved by GTN or rest
TACHYCARDIA AND FEAR
Dyspnea
Serum cardiac markers to be considered for MI
Troponin TNI
Creatanine kinase CK
CK-MB
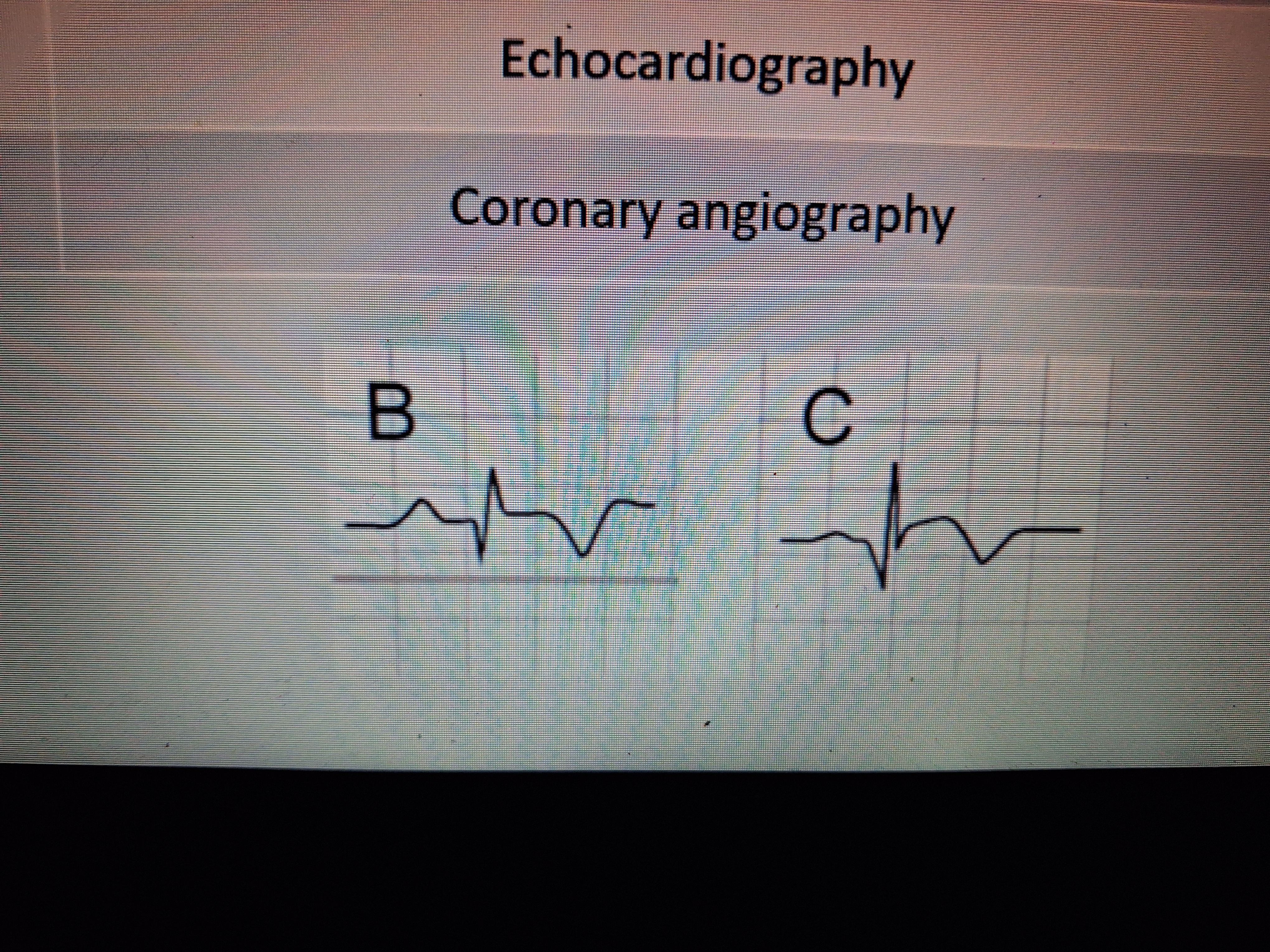
Ecg of angina
Depressed depression (not inverted)
Flattened t wave (or reversed)
ECG of Mi
T wave inversion
ST segment elevation
Formation of Q wave
Examples of cardiac nursing diagnosis during MI
Acute pain
Ineffective tissue perfusion evidenced by low blood pressure
Activity intolerance
Fear/anxiety
Causes of atrial fibrillation
Age
Other heart disease or issues (ischemia,.previous heatt attack, structral, hypertrophy)
Htn
Other medical issues, ckd/thyroid/osa/infection/diabetes
Postop esp. cardiac procedures
Alcohol
Obesity
Family history
Pathophysiology of atrial fibrillation
Randmon electrial signals occur in atria causing out of rhythm twitching, palpitations and less effective pumping
Symptoms of AF
Can lead to clots
Palpitations
dyspnea/feelings of shortness of breath
Lightheaded
Diagnosis and screening of AF
History- signs symptoms
Asymptomatic- can be detected by smart watch,
Symptomatic- fatigue, SOB, palpitations, lightheaded, chest pain, palpate the pulse!!
ECG- chaotic fibrillation instead of p waves, irregular rhythym (RR interval)
Add. Screening- Tt Echo to see e.g size of heart (bigger = more cells to act up) valvular disease/abnormality , se. Electrolytes, hb/anemia, TSH increase, htn, osa, diabetes (if some kf these are managed it can control AfF)
What is paroxysmal (early) AF
Starts and stops suddenly without much provocation
Can last for seconds, minutes, weeks
Will revert spontaneously
What is persistent AF
Episodes last longer than a week
May revert spontaneously
Usually medication or cardioversion treatment needed to revert
Long term persistent AF
Continues uninterrupted for longer than one year
Heart will not return to normal, medications or cardioversion can be tried to revert rhythm
Medications may control symptoms
What is permanent AF
Doctor and patient decide to accept AF and focus on rate rather than rhythm
What medications may be used for medical cardioversion
Flecainide
Amiodarone
Sotolol
Why js anticoagulant therapy important in AF and what is the duration needed pre and post cardioversion
Prevent clot formation
Commonly Apixaban or eliquis
Anticoagulant therapy needed for minimum 4 weeks post to prevent normal sinus rhythm releasing clots later on and 3 weeks prior OR has occured definitely less than 48hrs
Medications used to maintain normal rate in AF
More effective in less symptomatic cases
Beta blockers or Ca channel blockers support heart to have consistent rate, digoxin
Treatments for AF
Medication e.g beta blockers or ca channel blockers, ablation, cardioversion medical or electrical, anticoagulants to prevent complications
Complications of AF
Af with rapid ventricular response
-ventricles unable to fill properly = decreased cardiac output
- bp, pulse volume and rate, resp rate, poor perfusion, pallor, Restlessness, confusion, headache, dec. Appetite, lightheaded
fluid backlog (farigued heart = HF = oedema, lung crackles, resp rate, sacral and ankle swelling
PE or stroke
Physiology of MI
Symptoms and manifestations of AF
Symptoms and manifestations of MI
What is inportant for efficient conduction of the heart
Rapid activation - simultaneous contraction of myocardium- one strong contraction
Sequential activation (following normal sequence- atria - rest- ventricles)- allows atria to fill adequately before ventricle contracts
Diastole
Relaxation of the ventricles
The first heart sound is a closure of these valves
Atrioventricular (tri and bi cuspid)
The second heart sound is a result of these valves closing
Semilunar
Which chambers of the heart are empty during ‘lub’
Atria, ventricles have been filled
Which chanbers of the heart are empty during ‘dub’
Ventricles, the atria will begin filling immediately
Where does the blood flow throughout the cardiopulmonary system
Sup and inf vena cava
R) atria
Tricuspid valve
Pulmonary trunk
Pulmonary Arteries
Lungs
Pulmonary veins (oxygenated)
L) atria
Bicuspid/mitral valve
L) ventrical
Semilunar valve
Aortic arch
Where do the coronary arteries which nourish the myocardium originate
Base of the aorta
The coronary sinus empties into the X
R atrium
The fluid that fills the pericardial sac is to reduce X
Friction during heart activity
The membrane that lines the heart and forms the valve flaps is called the X compared to the external lining which is called X
Endocardium
Epicardium
Staples heart muscle together
Intercalcalated discs with gap junctions to allow for electrical currents to pass simulatenously
Pacemaker of the intrinsic conduction system
SA node
What anchors the flaps of the AV valves
Chordae tendonae
What happens during the P wave
Atrial depolarizations
What happens during the QRS complex
Ventricular depolarizations
Atrial repolarizations
What happens during the T wave
Ventricular repolarization
What is this formula: CO = HR . SV
Cardiac output= heart rate . Stroke volume
Average adult cardiac output per minute
5250ml / roughly 1x blood volume
What is starlings law of the heart
Force of the heartbeat or stroke volume is dependant on the degree of stretch of the muscle just before it contracts, consequentially the force of heartbeat can be increased by an increased return of blood to the heart