MEDL350L Urinalysis Exam #2
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
Cerebrospinal fluid (CSF): Production by, absorbed by
Produced by ependymal cells of the brain in choroid plexus
Absorbed into circulation by cells in the arachnoid villi of CNS
Serous intermembrane fluids: Definition (secreted & absorbed by) & Types (5)
Small amount of fluid secreted & absorbed from mesothelial cells lining a double membrane system surrounding the lungs, heart & peritoneal cavity
fluids accumulate under following processes:
Transudative (transudate), Exudative (exudate), Pleural (thoracentesis), Pericardial, Peritoneal
Transudative (transudate): Definition/pathology & Total protein level
clear, acellular fluid accumulates due to cardiac/vascular conditions that cause heart failure & inefficient venous return to the heart → disabling absorption of fluid back into circulation
Total protein < 3.0 g/dL
Exudative (exudate): Definition/pathology & Total protein level
cloudy, hemorrhagic, cellular fluid accumulates because of infection, inflammation (SLE for example) or metastatic malignancy
Total protein level >3.0 g/dL
Pleural vs Pericardial vs Peritoneal (Anatomy of each)
thoracentesis: double membrane system surrounding lungs
Pericardial: surrounding the heart
Peritoneal: surrounding the visceral organs
Synovial fluid: Anatomy & Produced/reabsorbed by
from joint space; elbow & knee
Produced and reabsorbed by synovial lining cells
Handling & Appearance of Body fluid analysis: Volume documented & Appearance
Volume in mL should be documented
Appearance: clear, colorless, turbid, xanthochromic (bilirubin color tinge), bloody, etc. noted
CSF: Indications of lumbar puncture (8)
Meningitis, Encephalitis, Leukemia with or without CNS involvement, Metastatic tumors especially breast and lung, CNS abscess, hemorrhage, syphilis, and Multiple sclerosis
CSF Formation & Reabsorption: Plasma ultrafiltrate (protein concentration, types of proteins, glucose concentration)
1% of plasma protein concentration
at least 500 different proteins
60-70% of plasma glucose concentration
CSF Formation & Reabsorption: Produced & secreted by
Produced and secreted by the choroid plexus
Ependymal lining of the ventricles and subarachnoid spaces (anatomical blood-brain barrier)
CSF Formation & Reabsorption: Functions (2) & Absorbed by
Bathes, lubricates & cushions the brain & spinal cord
Circulates nutrients and removes wastes
Absorbed by the arachnoid villi
Normal CSF Values: Appearance & Total Volume
appearance: clear & colorless (occasionally is xanthochromic in jaundiced neonates)
vol: 90-150 mL in adults; 10-60 mL in neonates
Normal CSF Values: Turnover, Total protein (& albumin), & Glucose
50-500 mL/day
protein: 15-45 mg/dL
albumin 10-30 mg/dL
glucose: 50-80 mg/dL
Normal CSF Cell counts in Adults: Mononuclear, RBCs, lymphs, monocytes, neutrophils
0-5 mononuclear cells/microL
Few RBCs noted especially after a “traumatic tap”
60±20% lymphs
30±15% monocytes
2±4% neutrophils in adults
Normal CSF Cell count in Neonates: Monocytes, lymphs, neutrophils
70±20% monocytes
20±15% lymphocytes
4±% neutrophils
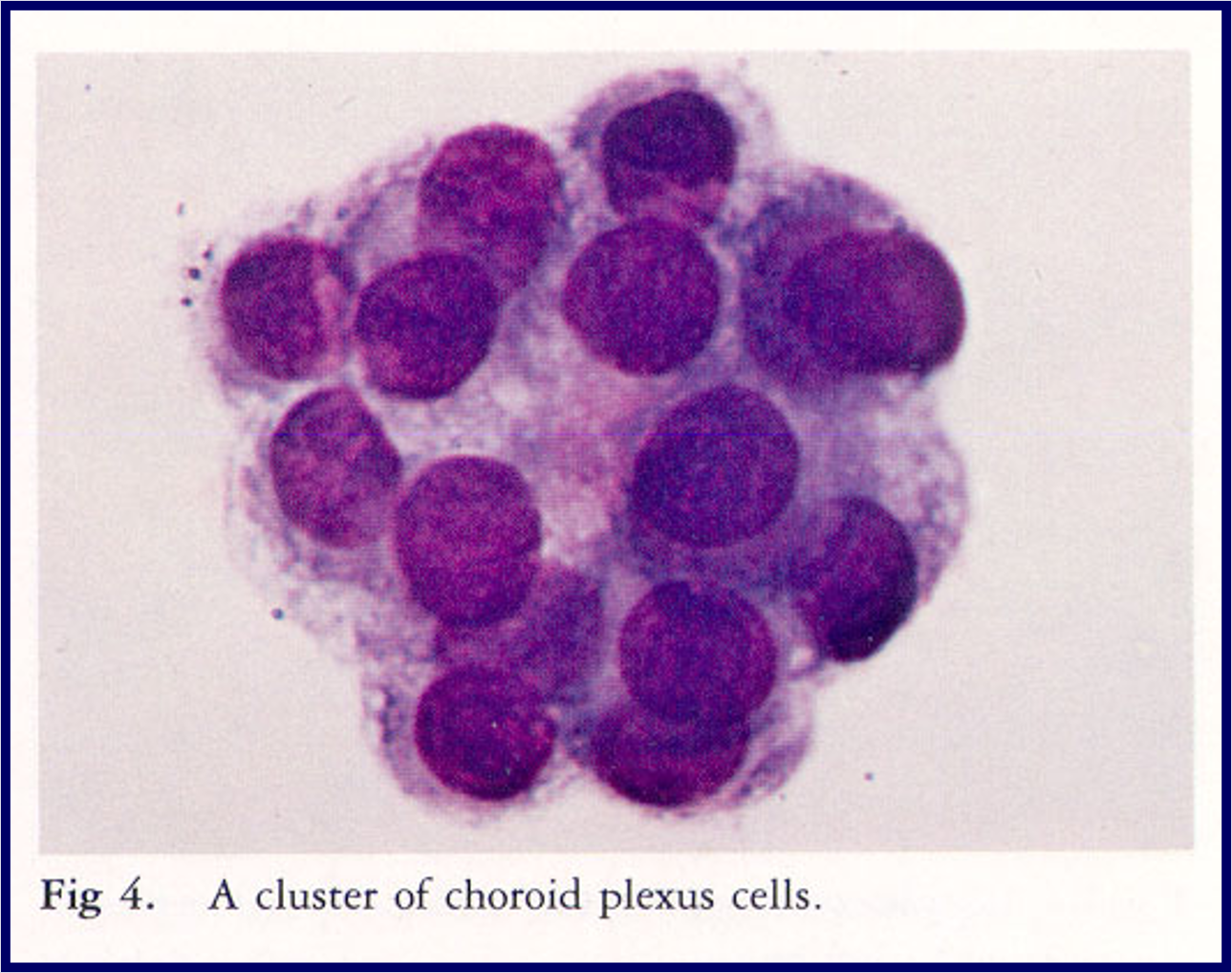
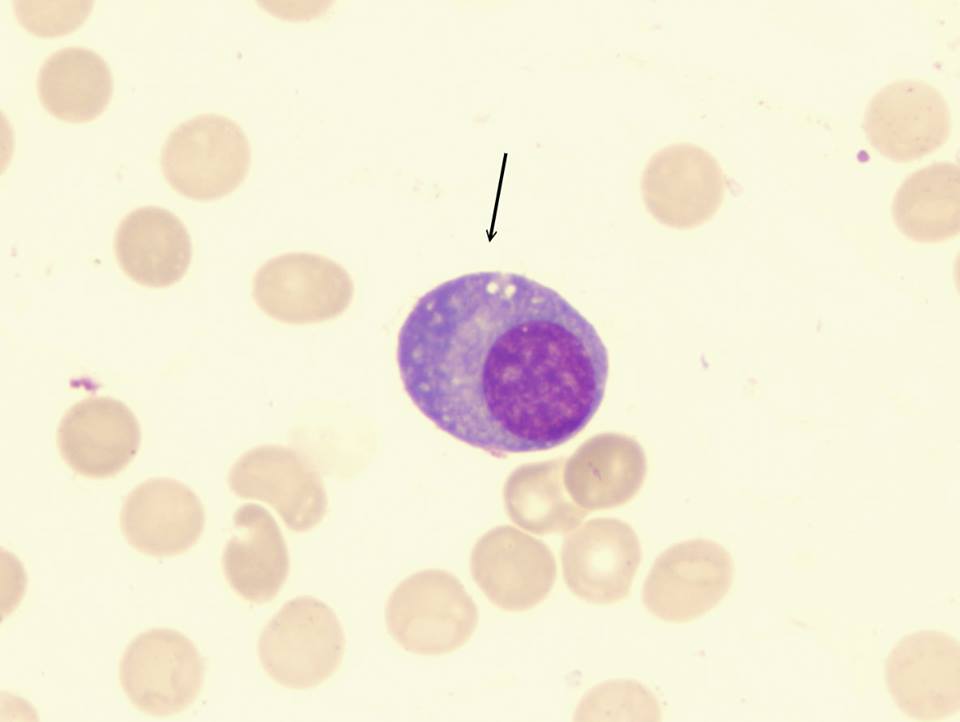
Ependymal Cells: Other name, anatomy, morphology, associated with
Also called choroid plexus cells line the ventricles & stain as uniform, lymphocyte-like cells with abundant gray-blue cytoplasm (found in clusters)
are associated with trauma, surgery, encephalography & ischemic infarct in CNS
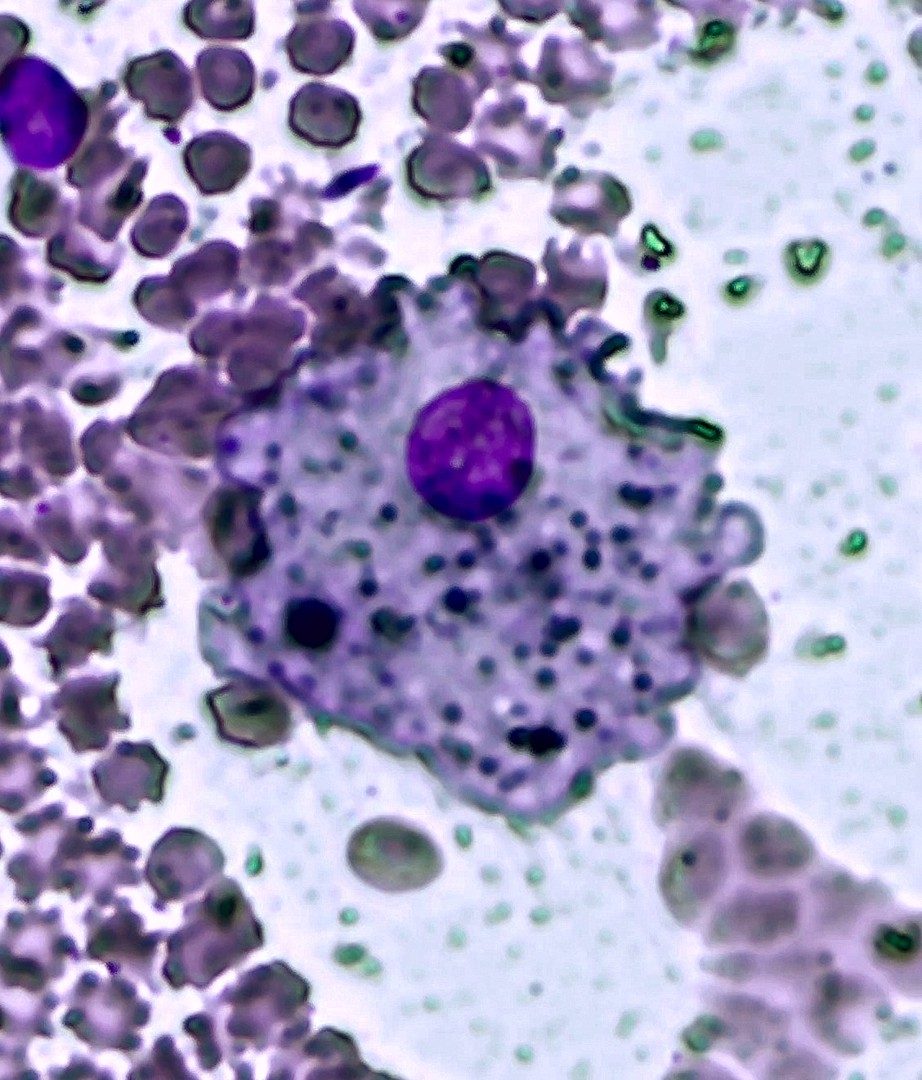
CSF pathology of Hemorrhage (CVA): Appearance, Presence of
Appearance: bloody, pink, brown, xanthochromic
Presence of RBCs & phagocytic WBCs (including signet-ring macrophages & Hemosiderinophages)
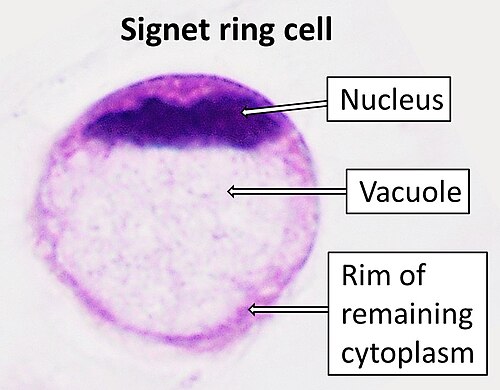
Hemosiderinophage vs Signet-Ring Macrophage
Hemo: macrophages that have ingested hemosiderin; have iron deposits in cytoplasm
Signet: macrophages that contain large, clear cytoplasmic vacuoles that push the nucleus to the periphery → “signet-ring” appearance
CSF pathology of Hemorrhage (CVA): Hemorrhage vs Traumatic Trap (Appearance of CSF)
hemorrhage: xanthochromic or brown supernatant after centrifugation
trap: clear supernatant after centrifugation, decreasing amount of RBCs in tubes 2 & 3 (if obtained)
CSF Pathology of CNS Infection/Inflammation: Diseases, Appearance, Presence of
Meningitis, encephalitis, syphilis, TB, MS, etc.
Appearance: turbid (cloudy)
Presence of WBCs
CSF Pathology of CNS Bacterial Meningitis: WBC count, WBCs as disease progresses vs after treatment, CSF glucose & total protein levels
WBCs often > 50,000/microL
as disease progresses: neutrophils can make up >90% of WBCs
after treatment/resolution: monocytes & lymphs make up majority
CSF glucose decreased (microorganism interfere with glucose transport)
total protein = markedly increased
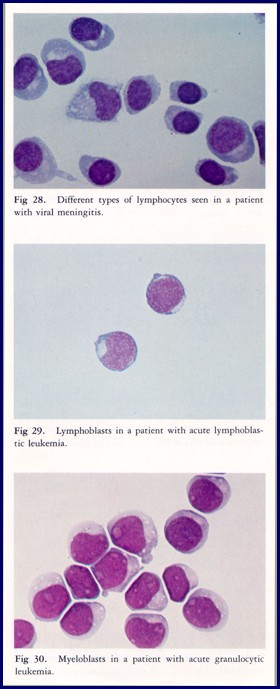
CSF Pathology of Viral Meningitis: WBC count, acute response, conditions associated with
Mild to severe leukocytosis present in CSF
Acute response: increase of neutrophils then increase predominantly in monocytes & lymphocytes including plasma cells
Fungal, parasitic infections, syphilis, TB, MS, & inflammatory conditions: associated with the presence of variant lymphs, eosinophils & basophils
CSF Malignancy of Malignancy: Leukemia (ALL & AML), WBC in CSF & Tumor cells
80% of ALL has CNS involvement
60% of AML has CNS involvment
leukemic cells including basophils may be present in CSF
Breast, lung, and other metastatic tumor cells
Serous intermembrane fluids: Type of system, type of cell that lines, covers/protects 3 organs
Double membrane system, lined with mesothelial cells
Covers and protects heart (pericardium), viscera (peritoneum) & lungs (pleural membranes)
Transudates: Appearance, total protein level, WBC count, LDH activity, pathology
clear & colorless
< 3 g/dL of total protein
< 1000 WBC/microL
LDH activity < 200 U/L
Accumulation due to alteration of normal hydrostatic pressure in circulatory failure
Increased capillary permeability or decreased reabsorption of fluids
Exudates: Appearance, total protein level, LDH activity, WBC count, accumulation in/pathology
turbid & purulent
> 3 g/dL of total protein
LDH activity > 200 U/L often >1000
WBC/μL > 100,000 RBC/μL
Accumulation in infection, inflammation, abscess, SLE, malignancy, hemothorax
Pleural Pathology: Presence of & Diseases
Presence of WBCs including PMNs, lymphocytes, monocytes, eosinophils, variant lymphocytes
bacterial infections, pneumonia, infarct, pancreatitis, tuberculosis, RA, pulmonary embolus, pneumothorax, malignancy
Pericardial Pathology: Presence of & Disease
Presence of WBCs including PMNs, lymphocytes, monocytes, eosinophils, variant lymphocytes
infection, malignancy, CHF, hypoproteinemia
Peritoneal Pathology: Presence of & Diseases
Presence of WBCs including PMNs, lymphocytes, monocytes, eosinophils, variant lymphocytes
trauma, malignancy, infection, ruptured spleen, cirrhosis, nephrotic syndrome, MS, TB, SLE, pancreatitis
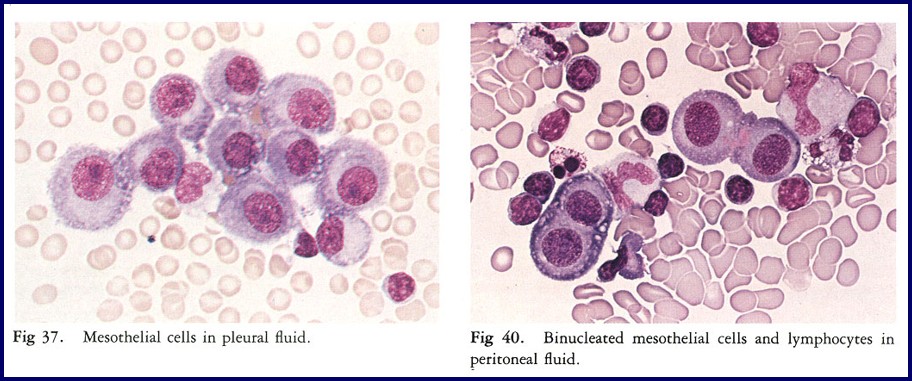
Mesothelial cells: Anatomy & Infectious/Inflammatory effusions
Cells forming lining of pleural, pericardial & peritoneal membranes
Infectious and inflammatory effusions: proliferation and desquamation
Mesothelial cells: Morphology
Appear as sheets or clusters of cells
12-30 μm with “fried egg” appearance
May be bi- or multinucleate (>20 nuclei/cell) with small vacuoles
Synovial Fluid: Synovium & Plasma ultrafiltrate
Synovium: cells lining space between joints
Production and secretion of plasma ultrafiltrate enriched in hyaluronate (proteoglycan)
Synovial Fluid: Appearance, should not have, total protein value, WBC count, cell differential (mono & neutrophils)
Appearance: light yellow, clear, viscous
Should not clot upon standing nor contain crystals
1-3 g/dL total protein
0-200 WBC/μL; 65% monocytes; < 25% neutrophils
Synovial fluid pathology of Gout: Appearance & WBC count
Milky, greenish with intracellular (neutrophils) & extracellular uric acid crystals present
WBCs 65-100,000/μL with > 90% neutrophils are common
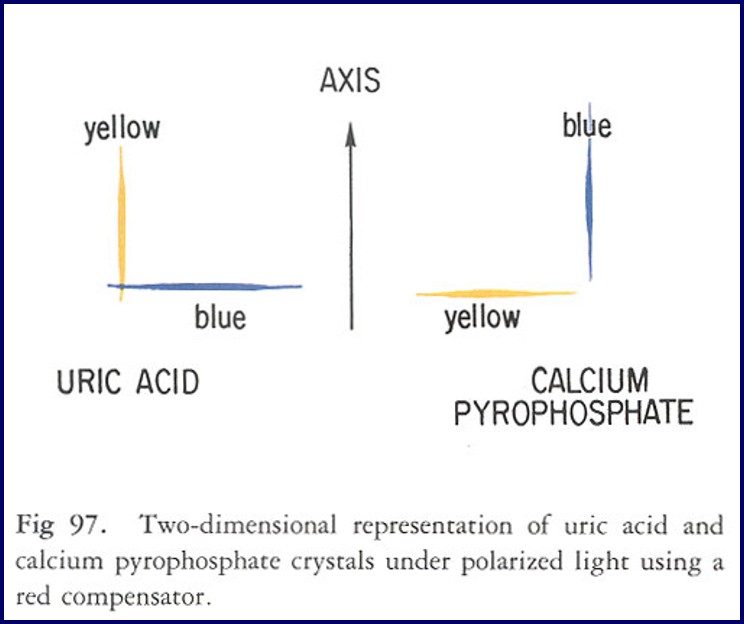
Uric Acid Crystals: Morphology & Polarized Light
1-20μm, needle-like
Yellow when parallel to the slow component of the compensator (negative birefringence)
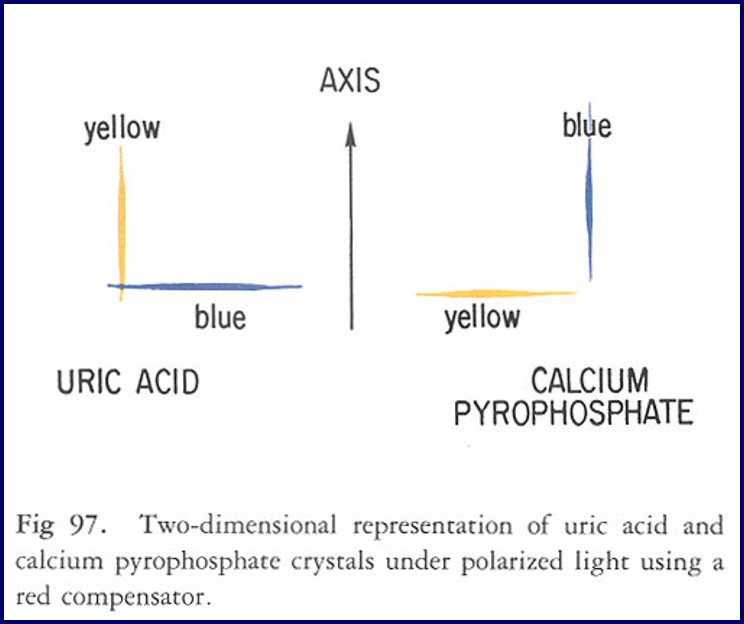
Calcium pyrophosphate: Morphology & Polarized light
pale rod, rhomboid, plate-like crystals
that are weakly and positively birefringent (blue when long axis is parallel to the slow component of the compensator)
Synovial fluid pathology of RA (Morphology)
Lymphocytes may predominate & ragocytes or RA cells (neutrophils containing immune complexes)
RBC morphology: Freshly Voided vs Crenated
freshly: normal biconcave shape
crenated: spiky/scalloped shape
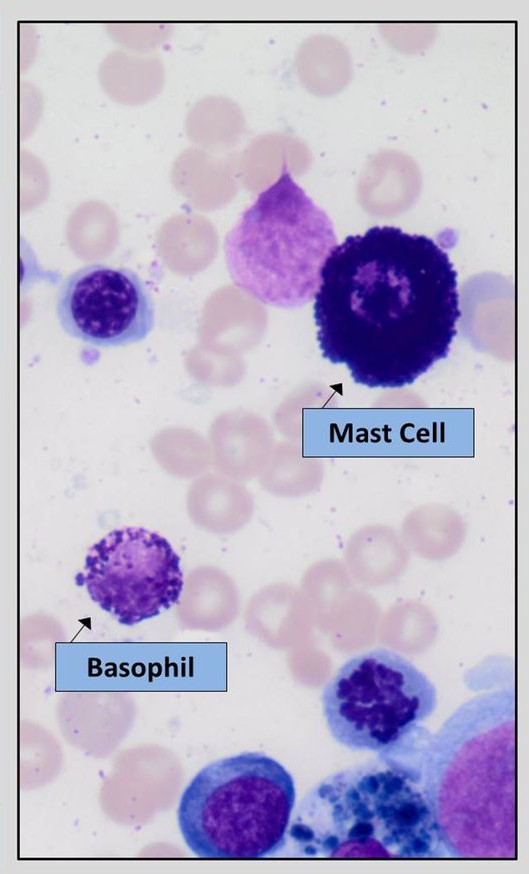
Mast cell Morphology
Plasma cell morphology
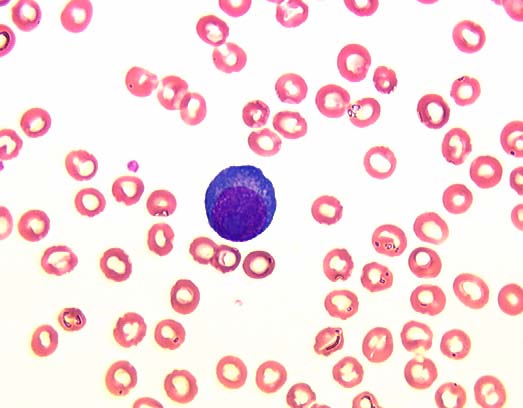
Blasts (morphology & indication)
indicates malignancy & hematologic
