(6) Acid-base balance
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
Average ph of ECF
7.4
Nonvolatile acid production from diet and metabolism is approximately
70 mmole/d
Kidneys reabsorb filtered — and excrete the —-
HCO3- ; nonvolatile acid
CO2 is considered a volatile acid. Why?
it is released by our body via the lungs
Show the net uptake of nonvolatile acid from diet via metabolism
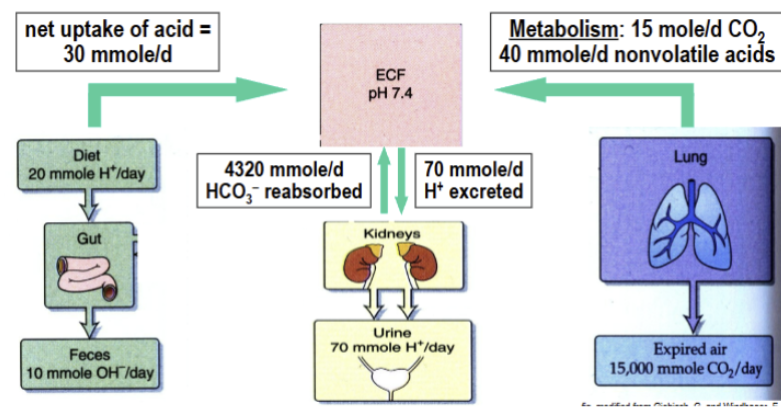
Volatile vs nonvolatile acid
Volatile and non-volatile acids are generated continuously by the body, differing by how they are eliminated. Volatile acids (carbonic acid) are derived from CO2 and exhaled by the lungs. Non-volatile acids (e.g., sulfuric, phosphoric, and lactic acids) are metabolic byproducts and must be excreted by the kidneys.
What 3 primary mechanisms regulate pH of body fluids?
buffering systems (phosphate, CO2/HCO3-, and ammonia which is unique); respiratory system (regulates CO2 levels of the CO2/HCO3- buffering system); kidney system (regulates HCO3- levels and excretes nonvolatile acid)
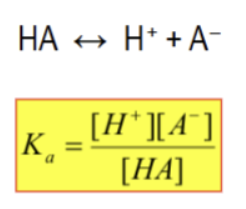
Proton buffer
anything that minimizes a change in pH. Incredibly important to neutralizing acid in the body.
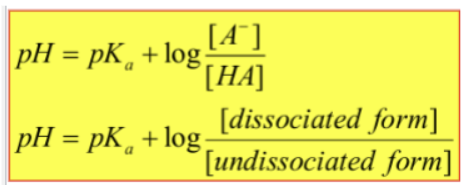
How to calculate Ka for reaction of weak acid
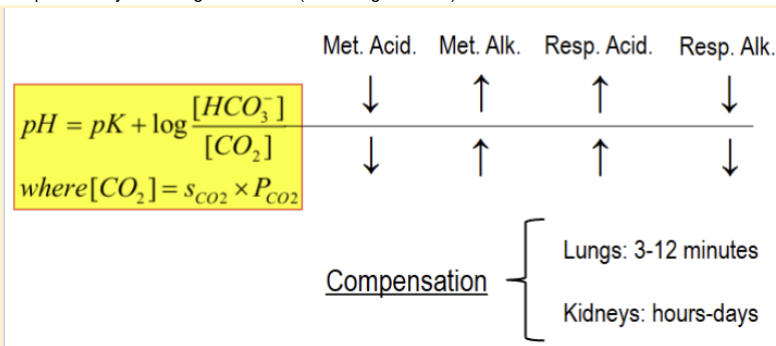
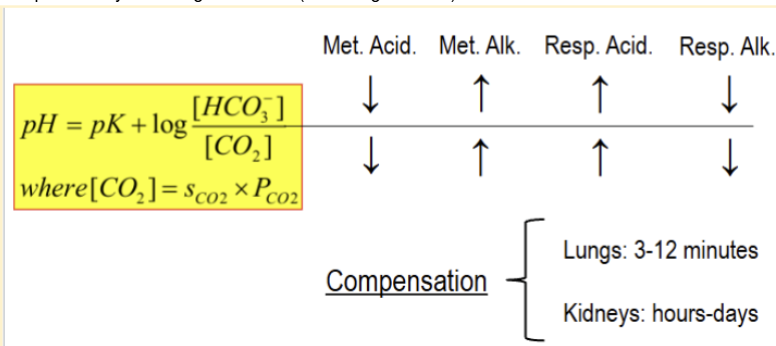
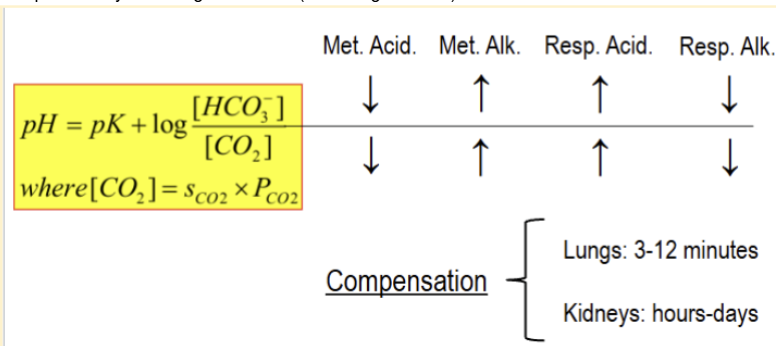
Henderson-Hasselbach equation
pK
pH where you maximal amount of proton buffering (equal amounts of A- and HA form of weak acid)
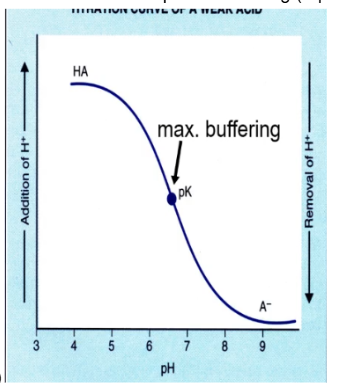
Aspects of a good proton buffer for the body?
pK is in physiological pH range (about 7.4) and needs to be high conc. In plasma,
Phosphate buffer
physiological buffer with a pK=6.8 and 1-2mM in plasma. Contributes significantly to proton buffering
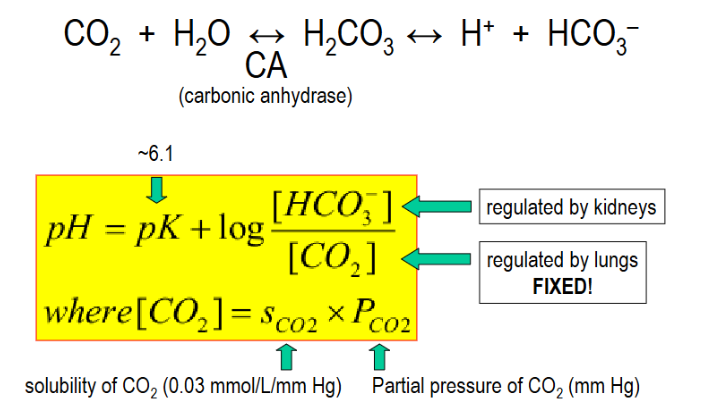
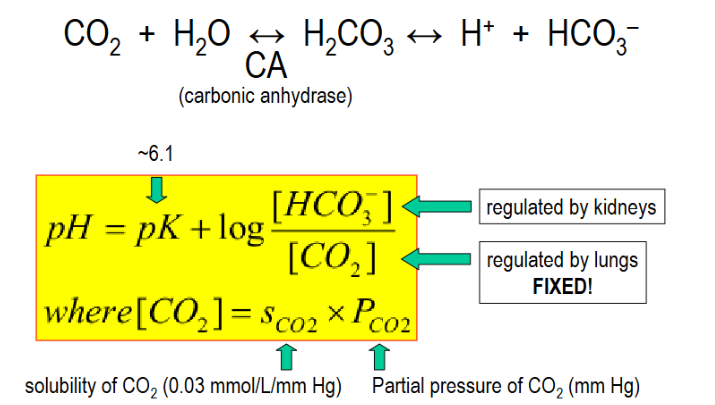
CO2/HCO3- buffer system
most important buffering system in body. pK is about 6.1 but bicarbonate conc. is high and CO2 can be expelled by lungs. This allows the reaction to go from right to left as needed.
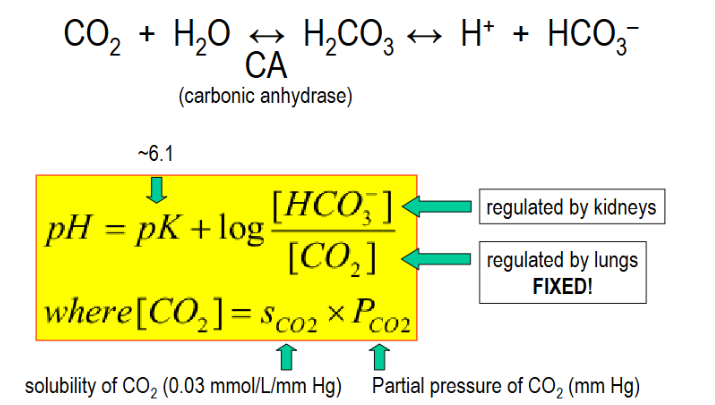
Carbonic anhydrase (in the HCO3- buffering system)
catalyzes reaction of CO2+ H2O into H+ and HCO3- for the CO2/HCO3- buffer system
Role of kidneys in acid/base balance
secreting H+ into the lumen so as to reabsorb filtered HCO3- and excrete net nonvolatile acid and produce an equal amount of new HCO3-
H+ excretion requires the binding of H+ to — which produces —- or — which produces —-
buffers (forming titratable acid) or ammonia/NH3 (forming ammonium/NH4+)
Titratable acid
H+ bound to a buffer that can be excreted
Net acid excretion
equal to the amount of titratable acid in urine plus the amount of ammonium (NH4+) in urine minus the amount of HCO3- in urine
3 essential steps involved in handling an acid challenge
1)bicarbonate and non-bicarbonate buffers neutralize most of the H+ (forming CO2 and BH
HCO3- reabsorption involves H+ —- not —-. What does this mean?
secretion not excretion; secretion means that the protons are not part of the final urine (which would be the case in excretion). They are recycled back into the cell as part of the HCO3- reabsorption mechanism
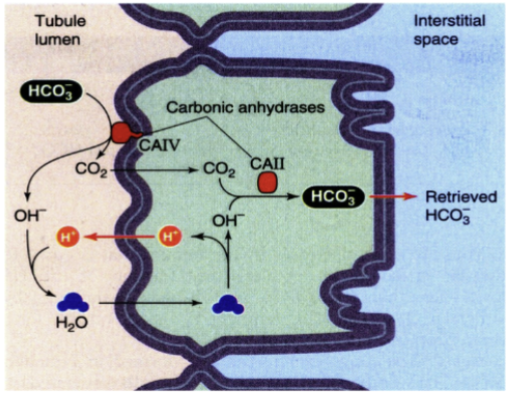
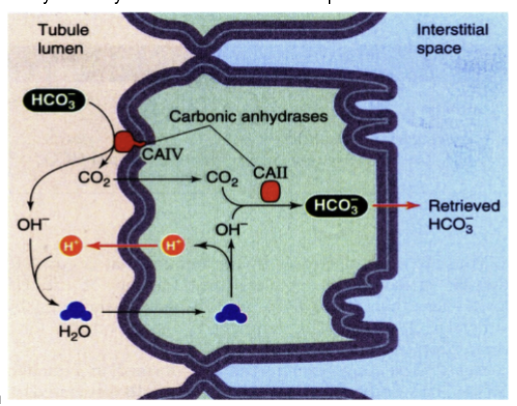
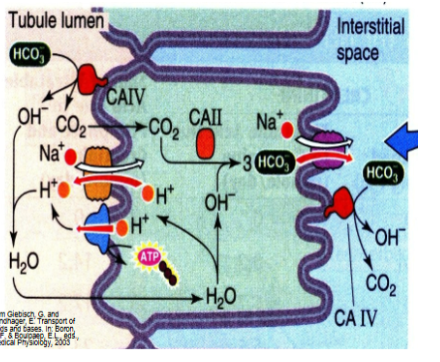
Show how HCO3- is reabsorbed. where does most HCO3- reabsorption occur?
CAIV tethered to apical membrane breaks HCO3- into CO2 and OH-, the OH- is protonated into water and enters the cell where it breaks back down to H+ and OH-. the CO2 also enters the cell where CAII catalyzes the reaction to reform HCO3- which then moves across the basolateral membrane. mostly (80%) occurs in proximal tubule
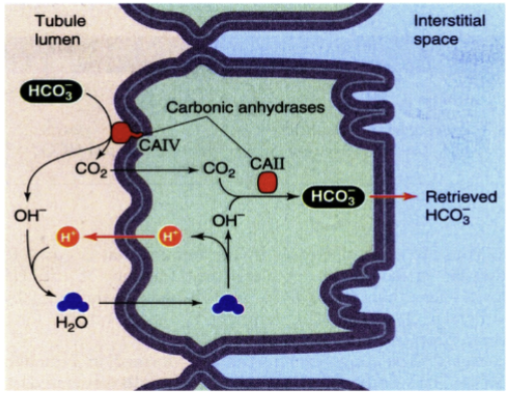
CAII vs CAIV
CAII is a intracellular carbonic anhydrase that forms HCO3- from OH- and CO2 while CAIV is extracellular and is involved in breaking HCO3- into CO2 and OH- in the lumen in order to transport it into the epithelial cell
t/f carbonic anhydrases are some of the fastest enzymes in biology
true
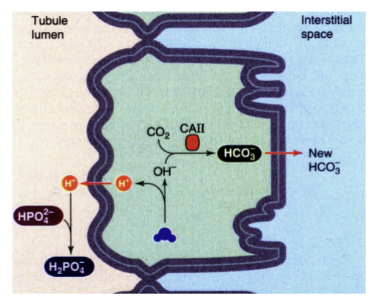
Show how H+ is excreted as a titratable acid in the kidney
H+ in lumen is bound to some buffer. excretion of 1 H+ as a titratable acid = 1 new HCO3- generated
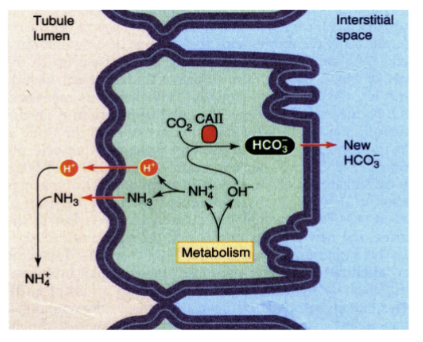
Show how H+ is excreted as ammonium in the kidney
glutamine metabolism leads to production of NH4+ and OH-. excretion of 1 H+ as a NH4+ = 1 new HCO3- generated
—% if HCO3- reabsorption takes place in the proximal tubule. –% occurs in the TAL and –% occurs in the distal nephron
80; 10; 10
~-- % of new HCO3- is generated from NH4+ excretion
60
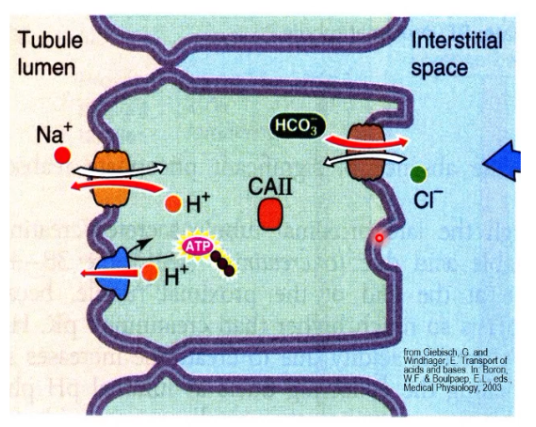
Show how both sodium and bicarbonate are reabsorbed in the proximal tubule. (Note any difference between early and late PT)
A basolateral Cl-HCO3 exchanger also contributes to bicarbonate reabsorption in the late PT.
Show how HCO3- is reabsorbed in the thick ascending limb (TAL)
less luminal CA in the nephron segments after the PT
t/f there is more expression of the luminal carbonic anhydrase as you move down the nephron
false, it is expressed less as most HCO3- reabsorption occurs early in the nephron
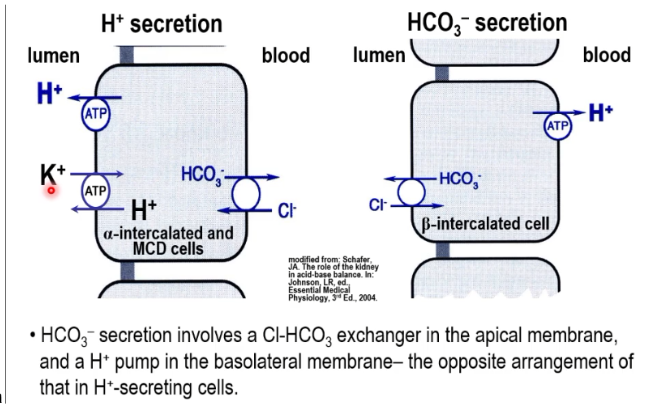
Show the difference in acid-base handling by alpha intercalated cells vs beta intercalated cells
alpha is involved in H+ secretion while beta is involved in HCO3- secretion. The expression of the Cl-HCO3 exchanger is flipped from basolateral on alpha to apical on beta
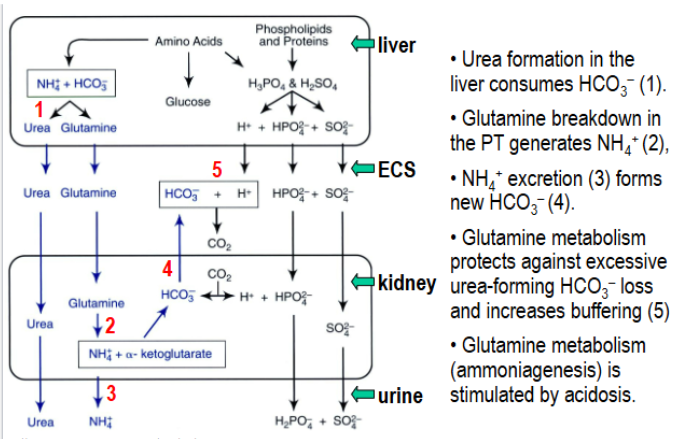
Show the role of urea and glutamine metabolism in acid/base balance
both paths rid the body of nitrogenous waste but differ in how they affect bicarbonate balance. Urea is formed from the liver as a way to package nitrogenous waste products. Glutamine breakdown in the PT generates ammonium and new bicarbonate. Because urea is made from bicarbonate and is lost in urine, it represents a loss of some base from the body. Glutamine metabolism protects against this HCO3- loss and increases buffering. This is why ammoniagenesis is stimulated by acidosis.
Ureagenesis (consumes or produces) HCO3- while ammoniagenesis (consumes or produces) it
consumes; produces
Respiratory acidosis
caused by increased PCO2. this can be caused by decreased alveolar ventilation or lung diffusion capacity or a ventilation-perfusion mismatch

Respiratory alkalosis
caused by decreased PCO2. This can be caused by increased alveolar ventilation such as in cases of hypoxia, anxiety, aspirin intoxication, etc.

Metabolic acidosis
caused by addition of other acids than CO2 or H2CO3 or removal of alkali (fixed PCO2). This can be caused by lowered urinary secretion of H+, ketoacidosis, lactic acidosis or HCO3- loss (as in severe diarrhea)

Metabolic alkalosis
caused by removal of other acids than CO2 or H2CO3 or addition of alkali (fixed PCO2). This can be caused by HCO3- load or loss of H+ (as in severe vomiting)

Compensation in an acid-base disorder
With an acid-base disorder caused by a metabolic or respiratory disturbance, the other system will attempt to compensate and minimize the change in pH
How does the body compensate in the case of Metabolic acidosis
lungs will compensate by releasing more CO2 (breathing hastens)
How does the body compensate in the case of Metabolic alkalosis
lungs will compensate by releasing less CO2 (breathing slows)
How does the body compensate in the case of Respiratory acidosis
kidneys will compensate by reabsorbing more HCO3-
How does the body compensate in the case of Respiratory alkalosis
kidneys will compensate by excreting more HCO3-
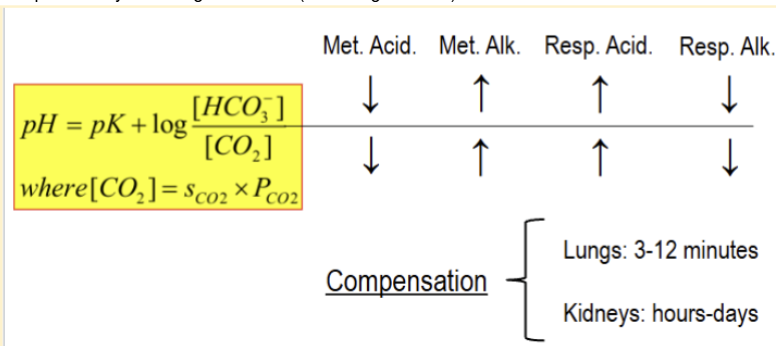
Difference in how long it takes the lungs vs kidneys to compensate in an acid-base disorder
lungs can compensate in about 3-12 minutes while kidney can take hours-days
How can you determine if the cause of an acid-base disorder is respiratory or metabolic?
if the PaCO2 is abnormal and consistent with the disorder, it is respiratory. If the HCO3- is abnormal and consistent with the disorder, it is metabolic. Both can be abnormal, but the one most consistent with the disorder is the main cause.