PTE 762: exam 3
1/137
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
138 Terms
what is the endocrine system?
a network of glands and organs that produce and release hormones directly into the bloodstream to act on target tissues located some distance awat from the original secreting gland or organ
list the major physiological functions of the endocrine system.
maintain internal homeostasis
reproduction
growth and development
energy metabolism
fluid/electrolyte balance
stress/injury response
what is the role of the hypothalamus within the endocrine system?
master regulator → controls/regulates pituitary gland and coordinates endocrine activity
what is the role of the pituitary gland within the endocrine system?
master gland the directs and controls peripheral glands
what is the role of the thyroid gland within the endocrine system?
aids in metabolism, growth, and development
what is the role of the peripheral glands within the endocrine system?
produces final hormones that affect target tissues (bone, breasts, gonads, adrenals, uterus, etc.)
describe the pathway of the endocrine system.
hypothalamus releases hormone → hormone stimulates pituitary to release another hormone → anterior pituitary releases hormone → travels to targeted tissue
pituitary hormones are secreted from the ______ pituitary.
anterior
what’s the difference between the mechanisms of the anterior and posterior pituitary?
anterior: signals delivered hematogenous (through blood stream) via hypophyseal vascular plexus
posterior: signals delivered via direct neuron innervation
what type of feedback does the endocrine system “run” on?
negative feedback
increasing hormone levels → inhibit hormone production
decreasing hormone levels → stimulate hormone production
describe the mechanisms of hormone action on intracellular receptors.
hormones enter cells, bind to intracellular receptors, alter gene transcription, and produce relatively slower but long-lasting effects on the target tissues
describe the mechanisms of hormone action on cell surface receptors.
activate second messenger systems and produces rapid cellular responses
hypothalamus releasing hormone to pituitary hormone flowchart
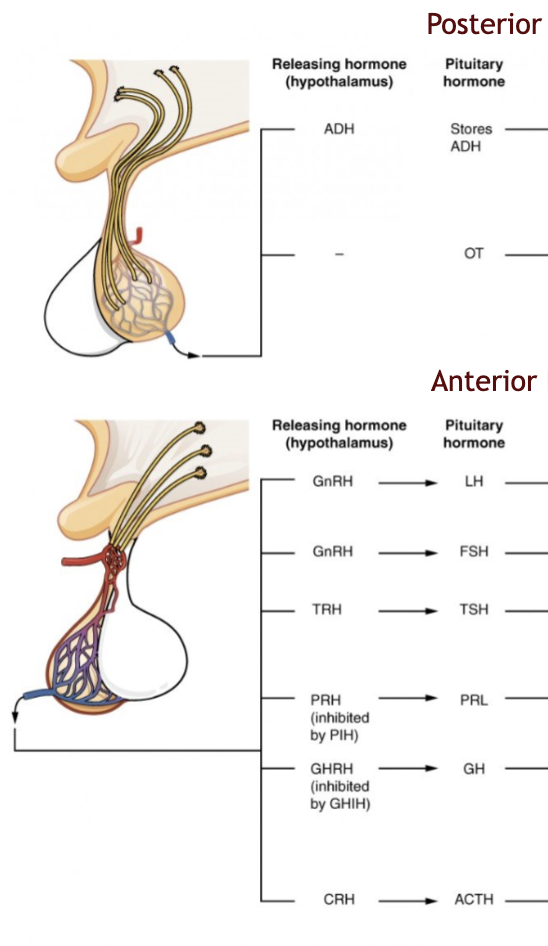
__ is a posterior pituitary hormone that acts on the kidneys, sweat glands, and circulatory system to conserve water and regulate blood pressure
ADH (antidiuretic hormone)
__ is a posterior pituitary hormone that acts on the female reproductive system to trigger uterine contractions during child birth and signals for milk let down (milk flows down the ducts and out of the nipple).
OT (oxytocin)
__ is an anterior pituitary hormone that acts on the reproductive system to stimulate production of sex hormones by the gonads.
LH (luteinizing hormone)
what’s the difference in LH function between males and females?
LH in males stimulates testosterone
LH in females stimulates ovulation, estrogen, and progesterone
___ is an anterior pituitary hormone that acts on the reproductive system to stimulate production of sperm and eggs.
FSH (follicle-stimulating hormone)
FSH =
follicle development + estrogen and sperm production
__ is an anterior pituitary hormone that acts on the thyroid gland to stimulate the release of thyroid hormone (T3/T4).
TSH (thyroid stimulating hormone)
__, triiodothyronine, is the active form of TH as it binds to intracellular receptors to increase metabolic activity.
T3
__, thyroxine, is the storage form of TH and is available for conversion to triiodothyronine within the liver, kidneys, and skeletal muscle via deionization and allows adjustment of thyroid activity tissue-by-tissue.
T4
__ is an anterior pituitary hormone that acts on the mammary glands to promote the production of milk.
PRL (prolactin)
__ is an anterior pituitary hormone that acts on the liver, bones, and muscles to produce insulin-like growth factors (IGF) which stimulate tissue growth and development.
GH (growth hormone)
____ is an anterior pituitary hormone that acts on the adrenal glands to stimulate the adrenal cortex to produce glucocorticoids which regulate metabolism and the stress response and to regulate the production of sex hormones.
ACTH (adrenocorticotropic hormone)
___ is produced by the parathyroid gland and raises blood calcium levels by stimulating bone resorption, increasing calcium reabsorption in the kidneys, and increasing activation of vitamin D.
PTH (parathyroid hormone)
_______ is produced by the parafollicular cells of the thyroid and lowers blood calcium levels by inhibiting osteoclast activity and reducing bone resorption
calcitonin
what are the three axises associated with the endocrine system?
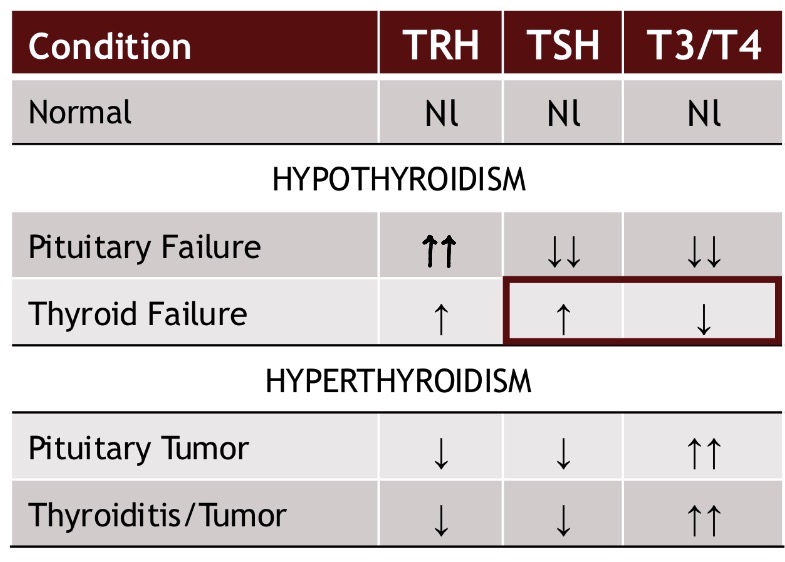
hypothalamus (TRH) → pituitary (TSH) → thyroid (T3/T4)
hypothalamus (CRH) → pituitary (ACTH) → adrenal (cortisol)
hypothalamus (GnRH) → pituitary (LH/FSH) → gonadal (sex hormones)
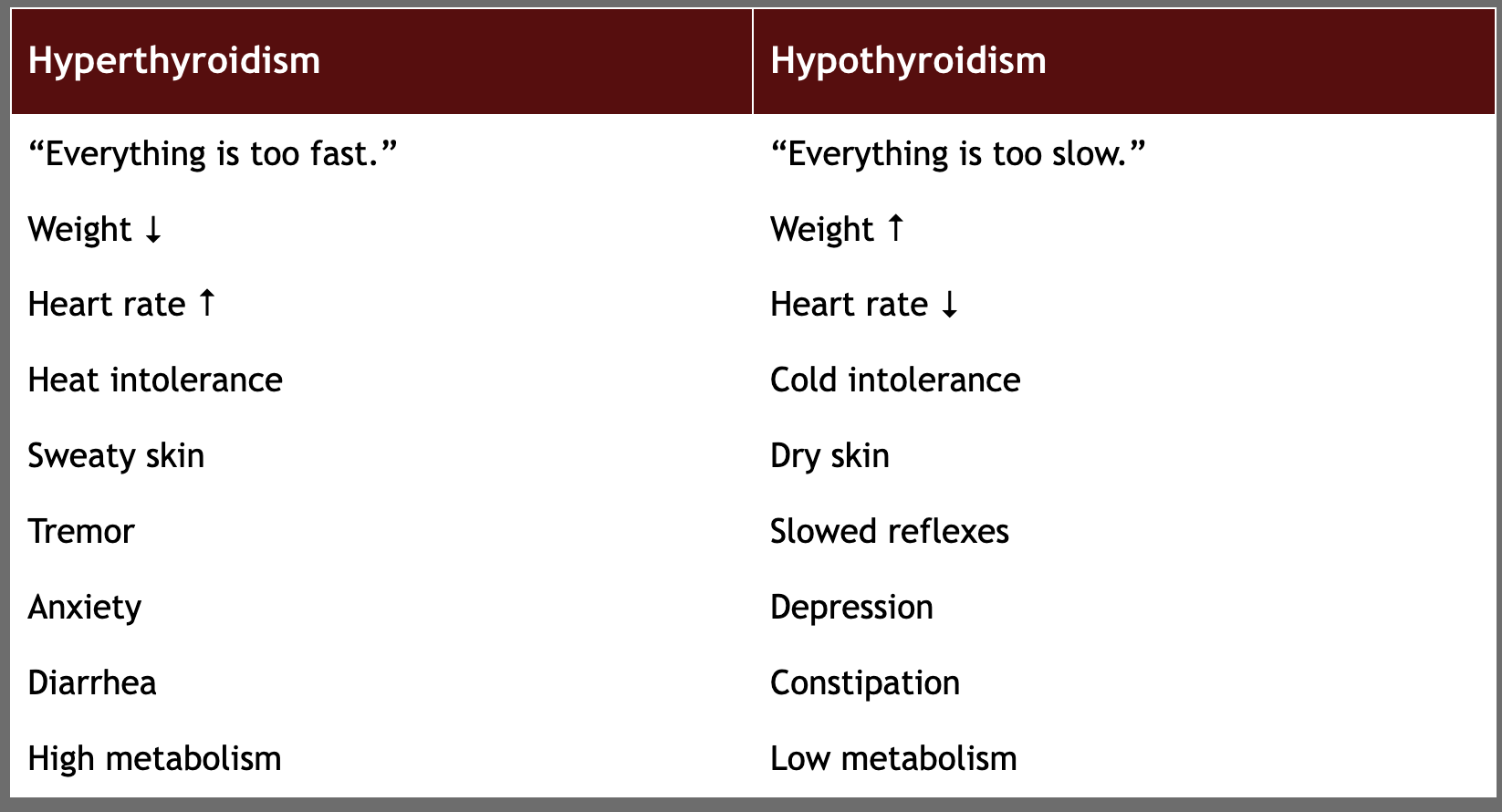
hypothyroidism vs hyperthyroidism chart
T or F: endogenous hormones can be viewed as naturally occurring drugs.
T
how can pharmacologic agents play a role in endopharmacology?
replace deficient hormones
mimic hormones
enhance hormone effects
block excessive hormone activity
regulate normal endocrine function
what are the hormones released by the adrenal cortex?
glucocorticoids: cortisol and cortisone
mineralocorticoids: aldosterone and cortiocsterone
androgens: estrogen and testosterone
catecholamines: epinephrine and norepinephrine
peptides: somatostatin and substance P
what are the major physiological functions of cortisol (glucocorticoids)?
regulates carbs, fat, and protein metabolism, physical/emotional response, potent anti-inflammatory, suppresses immune function, and maintains vascular response
Hydrocortisone (Cortef, Prednisone) is a drug therapy used for replacing cortisol. what are some things PTs should monitor in patients taking this drug?
osteoporosis, infection, muscle weakness, hyperglycemia, and delayed wound healing
what is a test used by medical professionals to rule in/out excess cortisol?
Dexamethasone Suppression Test
what are the major physiological functions of aldosterone (mineralcorticoids)?
increases Na+ reabsorption, water retention, K+ excretion, and H+ ion excretion; maintains blood pressure and blood volume levels
Fludrocortisone (Florinef) is a drug therapy used for replacing aldosterone. what are some things PTs should monitor in patients taking this drug?
hypertension, edema, weakness, and cramping (from hypokalemia)
what are the major physiological functions of sex hormones (adrenal androgens)?
contribute to pubic and axillary hair, source of androgens in females, can be converted to testosterone or estrogens in peripheral tissues, minor role in adult males compared with testicular testosterone
list some changes seen due to fluctuations in hormone levels.
fatigue, muscle weakness and wasting, gait impairment, neuropathy, delayed wound healing, increased facture risks, fragility fractures, abnormal CV responses
a patient presents to the therapy clinic following a distal tib-fib fracture. he demonstrates decreased stance time with limited ankle dorsiflexion during heel strike and swing phase. upon inspection of the ankle, the therapist notices dry skin, hyperpigmentation, and a lot of bruising. aside from the obvious MSK disorder, what other system should be checked?
endocrine system for a disorder
a pateint presents to the ER with complaints of cold intolerance, unexplained weight gain within the past two weeks, and peeing large amounts but only a few times a day. she thinks she is dehydrated because she also experiences muscle cramps and occasional tremors. aside from hydration levels, what system should be checked?
endocrine for a disorder
a routine patient presents to the clinic for generalized weakness and exercise intolerance. the therapist notices the patient appears to have lost a lot of weight in a short period of time and has patchy hair distribution along his BLEs with dry skin. aside from a CV disorder, what other system should be checked?
endocrine
why do endocrine disorders appear similarly to cardiovascular disorders?
hormones act as the master regulators of heart rate, blood pressure, and vascular tone leading to abnormalities that mirror those found in CV disorders
what is the main function of the thyroid gland?
control metabolism
a patient presents to the ER with complaints of SOB, high HR, bulging eyes (exopthalamus), and a sweaty appearance. during the examination, the patient reveals a family history of HTN, recent weight loss, and an anxiety diagnosis. upon further testing, the ER nurse finds heat intolerance, tachycardia, tachypnea, and a goiter. the patient most likely presents with _____________.
hyperthyroidism
a patient presents to the ER with complaints of recent unexplained weight gain, fatigue, increased depression, and hair loss. during the examination, she reveals a new onset of menstural irregularities and constipation. upon further testing, the ER nurse finds bradycardia, hypotension, and an abnormal puffiness of the her face. the patient most likely presents with _____________.
hypothyroidism
thyroidism chart
what is Graves’ disease?
an autoimmune disorder in which the immune system mistakenly attacks the thyroid gland (stimulating TSH receptors) causing the gland to overproduce thyroid hormones → resulting in hyperthyroidism
what physical presentation is associated with Graves’ disease?
tachycardia, fine tremors, warm moist skin, hyperreflexia, possible goiter and exophthalamus, fatigue, and muscle weakness
what are three drugs to “treat” hyperthroidism?
Methimazole (Tapazole)
Propylthiouracil (PTU)
Potassium Iodine
what is Hashimoto disease?
an autoimmune disorder where your immune system mistakenly attacks your thyroid gland (targeting the follicular cells that produce T3/T4) damaging the gland and reduces its ability to produce thyroid hormones → resulting in hypothyroidism
what physical presentation is associated with Hashimoto disease?
bradycardia, dry skin, puffy face, delayed reflex relaxation, hoarse voice, slowed movements, and generalized weakness
what are three drugs that “treat” hypothroidism?
Levothroxine (T4)
Liothyronine (T3)
Desiccated thyroid
T or F: thyroid medication should be taken at the same time of day and on an empty stomach.
T
what’s the difference between type 1 and type 2 diabetes?
type 1: autoimmune destruction of B-cells (no insulin production)
type 2: insulin resistance with B-cell dysfunction
an elevated HbA1c of ___ indicates a diabetes diagnosis.
≥ 6.5%
an elevated fasting plasma glucose level of ____ indicates a diabetes diagnosis.
≥ 126 mg/dL
________, an alpha pancreatic cell, raises blood glucose by stimulating glycogen breakdown, glucose production, and fat breakdown.
glucagon
______, a beta pancreatic cell, lowers blood glucose by increasing glucose uptake into muscle and fate, promoting glycogen synthesis, and inhibiting glucose production by the liver.
insulin
_________, a delta pancreatic cell, inhibits the release of insulin and glucagon and slows gastrointestinal motility and secretion; acts as a local regulator within the pancreas.
somatostatin
______, an epsilon pancreatic cell, stimulates appetite, promotes growth hormone release, and may influence glucose homeostasis.
ghrelin
__________ __________ regulates pancreatic exocrine secretion, gallbladder contraction, and may influence appetite and gastrointestinal function.
pancreatic polypeptide
what is the primary treatment of type 1 diabetes?
insulin
what is insulin’s effects on carbohydrate metabolism?
stimulates: glycogen synthesis and glycolysis
inhibits: glycogen breakdwon, hepatic glucose production, and gluconeogenesis
what is insulin’s effects on lipid metabolism?
stimulates: lipid stimulation and triglyceride storage (may cause obesity)
inhibits: lipolysis and ketone production
what is insulin’s effects on protein metabolism?
stimulates: amino acid uptake and protein synthesis
inhibits: protein breakdown
what stimulates the release of insulin?
elevated blood sugar, GI hormones, amino acids, and parasympathetic (vagus nerve) activity
describe the biphasic secretion of insulin.
rapid 1st phase: response to sudden increase in blood sugar as in after a meal
sustain 2nd phase: response to prolonged blood sugar elevation
how does excess insulin cause hypoglycemia?
too much insulin forces your body to process glucose faster than it can be replaced resulting in dangerously low levels due to accelerated sugar absorption and blocked glucose release
list some common complications of insulin therapy?
hypoglycemia
injection site pain
infection and/or allergic reactions
weight gain
describe the mechanism of action of Insulin.
treats type 1 diabetes
stimulates GLT-4 transporters to cell membrane and allows glucose to enter cells
inhibits glucose production in liver
describe the mechanism of action of Biguanides → Metformin (Glucophage).
treats type 2 diabetes
lowers liver glucose production with renal protection
decrease hepatic gluconeogenesis and increases insulin senstitivity
high incidence of nausea and diarrhea
describe the mechanism of action of GLP-1 Agonists → Semaglutide (Ozempic).
treats type 2 diabetes
mimics gut hormones to affect insulin release; increase glucose-dependent insulin secretion
proven CV protection
risk of catabolizing other organs leading to decrease muscle mass, pancreatitis, and gastroparesis
describe the mechanism of action of SGLT2 Inhibitors → Dapagliflizon (Farxiga).
treats type 2 diabetes
flushes sugar out through urine, blocking renal glucose reabsorption(glycosuria)
risk of Fournier’s disease and orthostasis but proven CV protection
describe the mechanism of action of Sulfonylureas → Glipizide (Glucatrol) and Glyburide (Diabeta).
treats type 2 diabetes
stimulates pancreatic beta cells to make insulin regardless of blood glucose concentrations
high incidence of hypoglycemia and obesity
describe the mechanism of action of Meglitinide → Repaglinide (Prandin) and Nateglinide (Starlix).
treats type 2 diabetes
short-acting stimulation of pancreatic insulin secretion, primarily around meals
risk of hypoglycemia
describe the mechanism of action of Thiazolidinediones → Pioglitazone (Actos) and Rosiglitazone (Avandia).
treats type 2 diabetes
increase insulin sensitivity
risk of fluid retention
describe the mechanism of action of DPP-4 Inhibitors → Sitagliptin (Januvia) and Linagliptin (Tradjenta).
treats type 2 diabetes
blocks incretion breakdown to increase endogenous insulin and decrease glucagon
risk of nausea, vomiting, diarrhea, and constipation but NO risk of hypoglycemia
a patient presenting with excessive thirst (polydipsia), frequent urination (polyuria), fatigue, blurred vision, increased appetite (polyphagia), and/or unexplained weight loss may be exhibiting signs and symptoms of ________.
hyperglycemia
a patient presenting with palpitations, tachycardia, tremors, anxiety, sweating/cold chills, intense hunger, nausea, change in cognition (confusion), difficulty concentrating, and/or changes in vision may be exhibiting signs and symptoms of ________.
hypoglycemia
a blood glucose level under ___ needs treatment in the form of fast-acting carbs.
70 mg/dL
T or F: the combined effects of exercise and insulin may produce an exaggerated dcrease in blood glucose, thus leading to hypoglycemia.
T
why does a patient with diabetes avoid exercise-induced hypoglycemia?
decrease his/her insulin does proportionally to the type, intensity, and duration of the physical activity (because the body needs sugar instead of inuslin to perform exercise)
what is diabetic ketoacidosis?
a complication related to diabetes where the body cannot use glucose for energy due to lack of insulin causing the body to break down fats and proteins instead. this breakdown causes acidic end-products, making the blood more acidic
a patient in the ICU suddenly presents with a high heart rate and is demonstrating a Kussmaul breathing pattern. upon entry to the patient’s room, an ICU nurse smells a strong nail polish acidic odor. the ICU nurse performs blood tests because she suspects what differential diagnosis?
diabetic ketoacidosis
what is hyperosmolar hyperglycemia state (HHS)?
life-threatening diabetes complication occurring when blood glucose levels are extremely high for a prolonged period, causing severe dehydration and highly concentrated blood
a patient presents to the ER with complaints of severe abdominal cramping, muscle cramping, and vomiting. his wife reports to the ER nurse that her husband has been complaining of headaches and was diagnosed with type 2 diabetes within the past year. during the examination, the ER nurse finds a high heart rate, low blood pressure, and A&O x1 (d/t confusion). the ER nurse performs a blood sugar test because he suspects what differential diagnosis?
hyperosmolar hyperglycemia
what is Addison’s disease?
a rare disorder where the immune system attacks the adrenal glands causing a decrease in the production of cortisol and aldosterone
a patient presents to the ER with a new onset of diarrhea/nausea/vomitting and muscle weakness. during the examination, the ER nurse finds hyperpigmentation and hypotension and testing revelas adrenal atrophy. what primary diagnosis should be considered?
Addison’s disease
what hormones must be replaced in treatments for Addison’s disease?
cortiocosteroids via Hydrocortison (Cortef) and mineralocorticoids via Fludrocortisone (Florinef)
what should therapists monitor in patients taking medications for Addison’s disease?
blood pressure, fatigue, proximal muscle weakness, blood glucose levels, signs of infection, edema, and muscle cramps
what is Cushing’s Syndrome?
a hormonal disorder caused by prolonged exposure to excess levels of cortisol in the body
a patient presents to the ER with complaints of hair thinning, muscle weakness, and big hump on her back (buffalo hump). the patient reports history of diabetes, osteoporosis, and HTN. during the examination, the ER nurse finds a lot of bruising and acne and striae of her abdomen along with a truncal obesity pattern. what primary diagnosis should be considered?
Cushing’s Syndrome
what is the ideal treatment for Cushing’s Syndrome?
removal of pituitary/adrenal adenoma
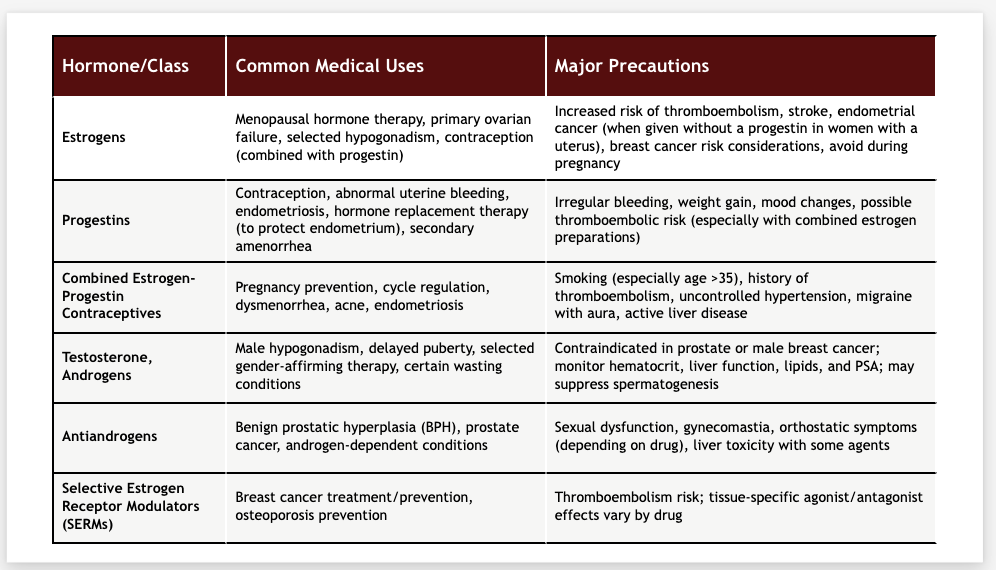
hormone replacement graph
a T-score of ___ indicates osteoporsis.
> -2.5
____ ____ is the gold standard of diagnosing osteoporosis because it measures bone density.
DEXA scan
describe the mechanism of action of calcium and vitamin D in osteoporosis treatment.
vitamin D increase Ca+ absorption and supports bone mineralization
- calcium carbonate is best absorbed when taken with acidic substances like coffee or OJ
describe the mechanism of action of Teriparatide (Forteo) in osteoporosis treatment.
recombinant parathyroid hormone with intermittent dosing stimulates osteoblast activity to promote new bone formation
describe the mechanism of action of RANKL inhibitor → Denosumab (Prolia) in osteoporosis treatment.
it is a monoclonal antibody against RANK ligand that prevents osteoclast formation → reduces bone resorption
high risk of rebound fractures and osteonecrosis of the jaw