Stable Angina
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
Define angina. What is the difference between stable and unstable angina?
Angina - chest pain, pressure or discomfort usually caused by ischemia of the heart muscle
Stable angina - predictable chest pain, brought on by exertion or emotional stress, relieved within minutes by rest or short-acting nitroglycerin
Unstable angina (UA) - chest pain increases (in frequency, intensity or duration) and is NOT relieved with nitroglycerin or rest
Describe the pathophysiology of stable angina.
Angina = Oxygen demand > Oxygen supply
Demand increases with:
↑ Heart rate
↑ Contractility
↑ Preload
↑ Afterload
Supply decreases with:
Coronary artery disease (atherosclerosis)
Coronary artery vasospasm
Can occur at rest or caused by illicit drug use (cocaine)
What type of tests are used to diagnose stable angina and assess likelihood of CAD?
1) Cardiac stress test
Increases myocardial oxygen demand with exercise or IV meds and monitors pt for sx of chest pain, SOB, lightheadedness, changes in HR/BP, ECG abnormalities
2) Coronary angiography
Performed to assess the extent of atherosclerosis and need for revascularization
Describe the treatment approach for stable angina.
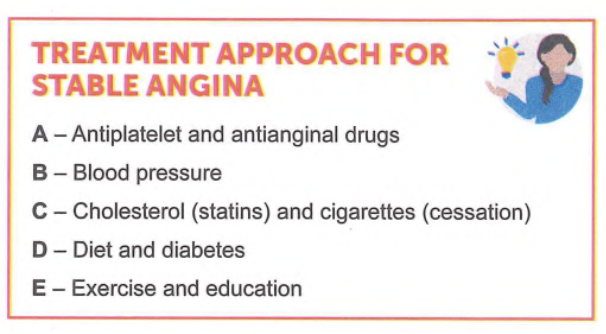
1) Antiplatelet (for secondary prevention)
Aspirin - recommended antiplatelet
Clopidogrel used when there is allergy or CI to aspirin
DAPT NOT useful for secondary prevention in pts with stable angina
Recommended only after recent ACS or percutaneous coronary intervention (PCI)
2) Antianginal (reduce chest pain)
3) BB, DHP / non-DHP CCB, long-acting nitrates
Prevent symptoms
4) Ranolazine can be added if needed after above therapies
5) Short-acting nitroglycerin (SL) or TL spray
Recommended for immediate relief of angina in ALL pts
Aspirin MOA
Irreversibly inhibits COX-1 and COX-2 enzymes —> ↓ prostaglandin (PG) and thromboxane A2 (TXA2) production
TXA2 is a potent vasoconstrictor and inducer of platelet aggregation
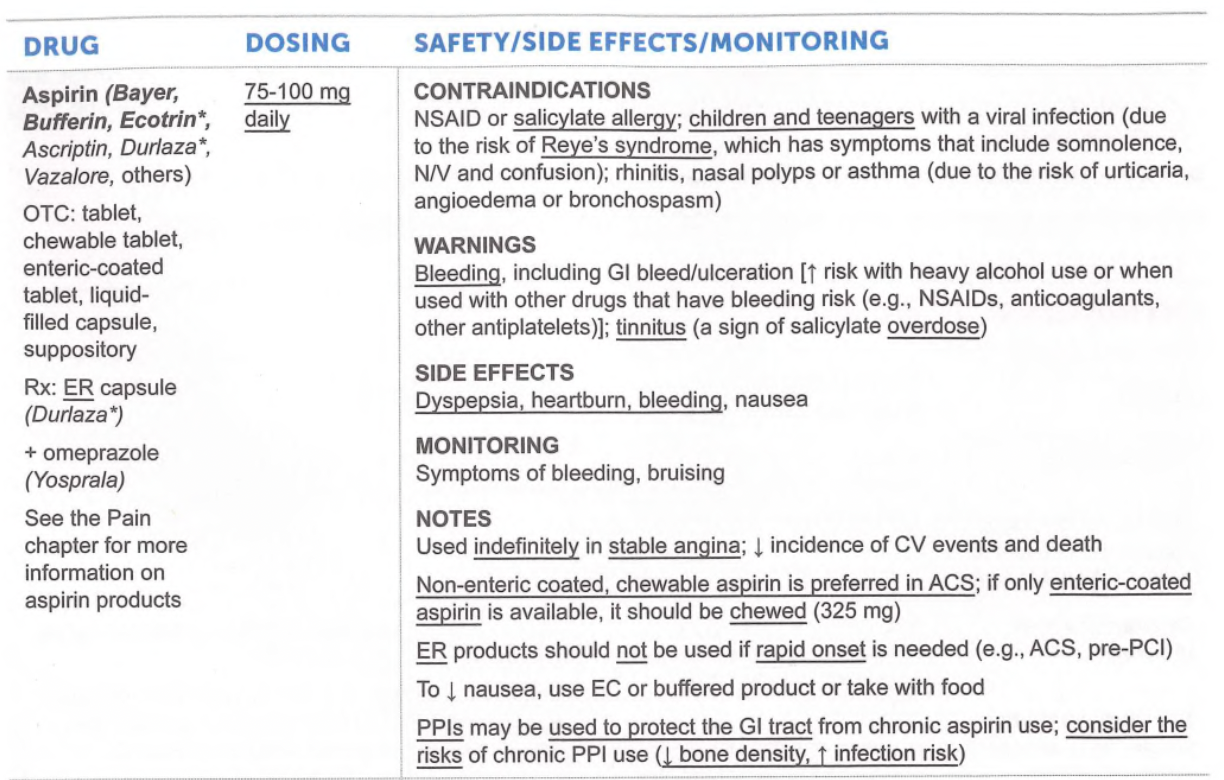
Aspirin CI
NSAID or salicylate allergy
Children and teenagers with viral infection (due to risk of Reye’s syndrome) - sx of somnolence, N/V, and confusion
Aspirin warnings / SEs/ monitoring
Warnings
Bleeding
Tinnitus (a sign of salicylate overdose)
SEs
Dyspepsia, heartburn, bleeding, nausea
Monitoring
Sx of bleeding, bruising
How long does a pt have to be on aspirin when used for stable angina? Why?
Used indefinitely in stable angina: ↓ CV events and death
What form of aspirin is preferred in ACS?
Non-enteric coated, chewable aspirin
If only enteric-coated aspirin availble, should be chewed (325mg)
What drug can be used to protect the GI tract from chronic aspirin use?
PPIs
Consider risk vs benefits
Risks: ↓bone density, ↑infection risk
Clopidogrel MOA
Prodrug that irreversibly inhiits P2Y12 ADP-mediated platelet activation and aggregation
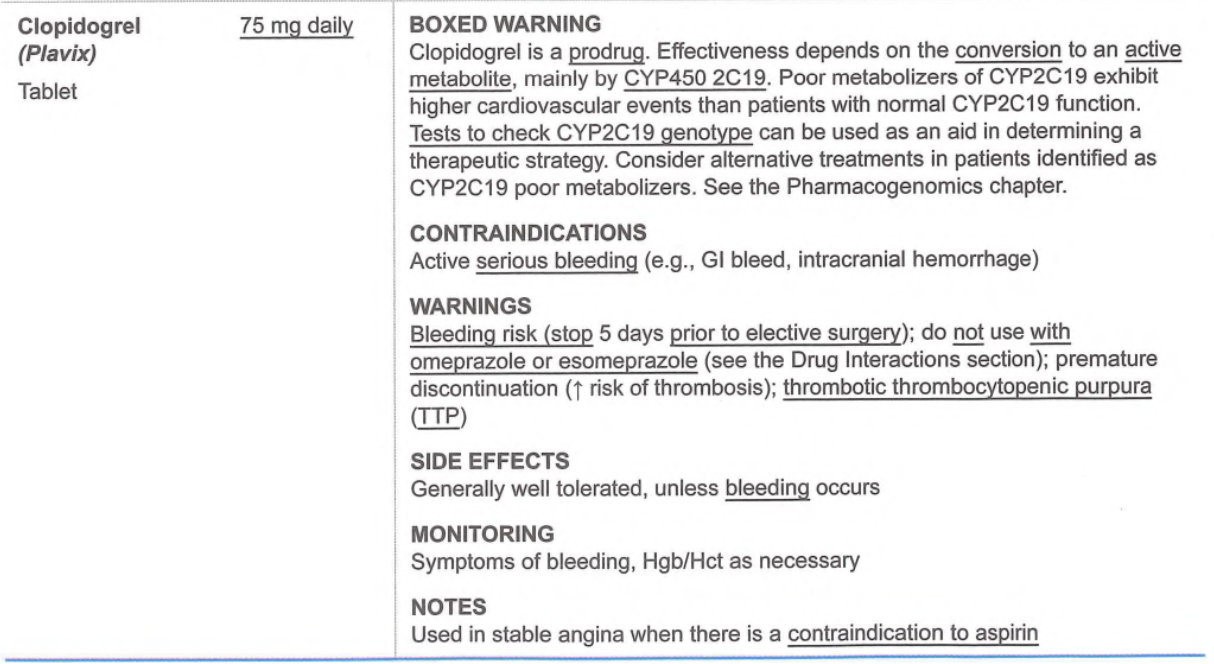
Clopidogrel boxed warning
Prodrug
Effectiveness depends on conversion to active metabolite via CYP450 2C19
If poor metabolizer, consider other treatments
Clopidogrel CI / warnings/ SEs/ monitoring
CI
Serious bleeding (GI bleed, intracranial hemorrhage)
Warnings
Bleeding risk
DO NOT use with omeprazole or esomeprazole
Omeprazole/esomeprazole: CYP2C19 inhibitors
Premature discontinuation (↑ risk of thrombosis)
Thrombotic thrombocytopenia purpura (TTP)
Small blood clots forming in many small blood vessels throughout the body
SEs
Bleeding
Monitoring
Symptoms of bleeding, Hgb/Hct as necessary
Clinical benefit of beta blockers as antianginal treatment.
Reduce oxygen demand from heart: ↓ HR, ↓ contractility, ↓left ventricular wall tension

In what type of angina should BB be avoided?
Avoid in vasospastic angina
Use CCB instead
Clinical benefit of CCB as antianginal treatment
Reduce myocardial oxygen demand: non-DHPs ↓ HR and contractility; DHPs ↓ SVR (afterload)
Slow release/long acting preferred
AVOID nifedipine IR
DHPs preferred when used with BB compared to non-DHPs
Risk of bradycardia

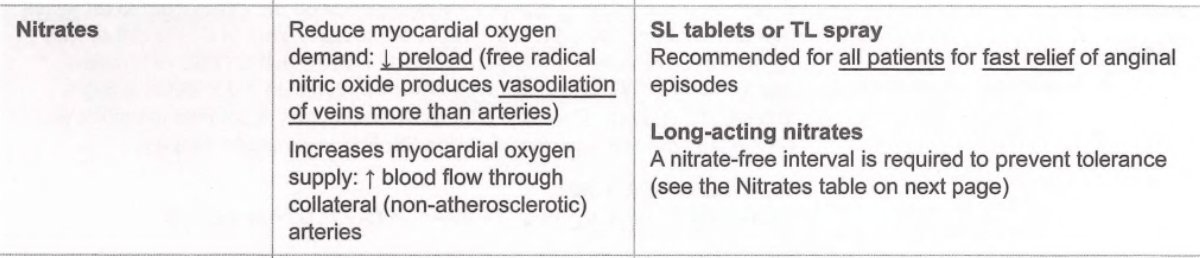
Clinical benefit of nitrates as antianginal treatment
↓ preload (free radical nitric oxide produces vasodilation of veins more than arteries)
Fast relief for chest pain
Nitrate CI
Do not use with PDE-5 inhibitors
Nitrate warnings / SE/ monitoring
Warnings
Hypotension
Tachyphylaxis (tolerance/↓effectiveness)
SE
HA, flushing, syncope, dizziness
Monitoring
BP, HR, chest pain
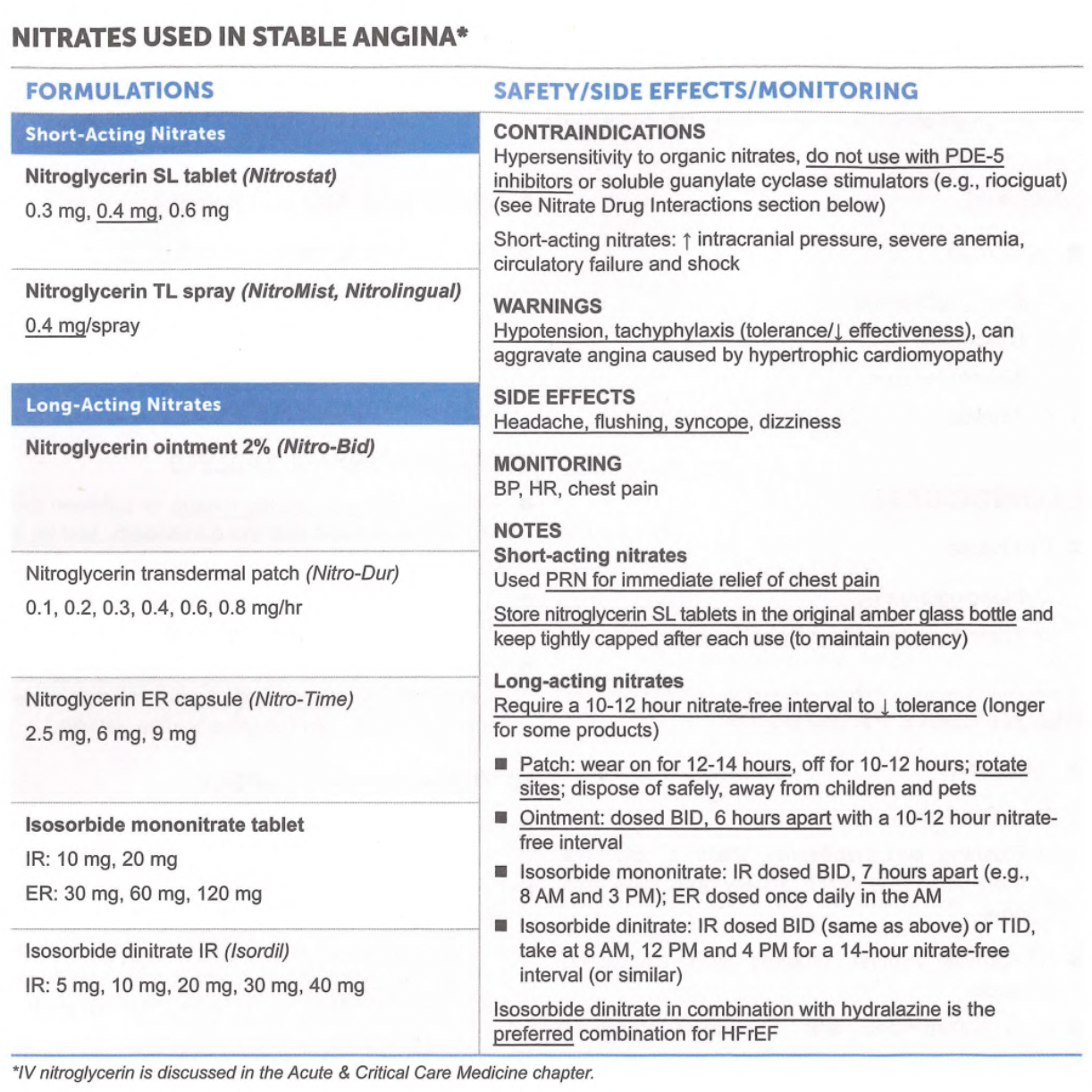
Long acting nitrates require a nitrate free interval. Why? How long is patch, ointment, and isosorbide mononitrate dosed?
Ranolazine MOA
Selectively inhibits late phase Na current and ↓ intracellular Ca
↓ ventricular tension
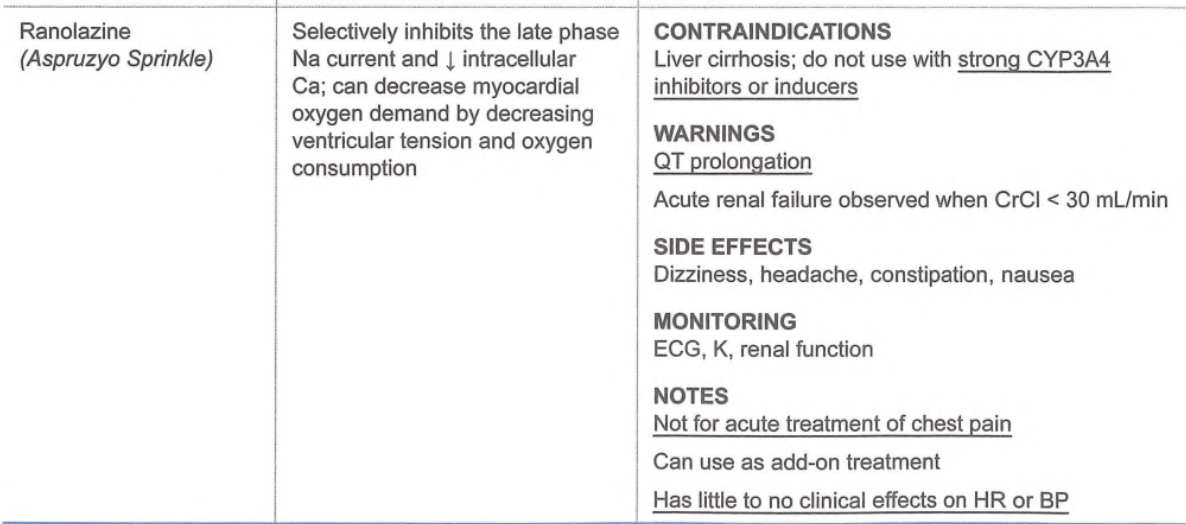
Ranolazine CI / warnings / SEs/ monitoring
CI
Liver cirrhosis; don’t use with strong CYP3A4 inhibitors or inducers
Warnings
QT prolongation
Acute renal failure observed when CLcr < 30 mL/min
SEs
Dizziness, HA, constipation, nausea
Monitoring
ECG, K, renal function
What is the major drug interaction with ranolazine?
Ranolazine is a major CYP3A4 substrate and minor CYP2D6 and pgp substrate
DO NOT use with strong CYP3A4 inhibitors or inducers