Looks like no one added any tags here yet for you.
What is mental health defined by the WHO?
State of wellbeing that includes the ability to cope with normal stressors, contribute to the community, realise own abilities and work productively.
What is the key criticism of the WHO definition?
It doesn’t account for the factors outside of an individuals control e.g. social and physical environment. It assumes the individual has complete control.
What are the objective factors that influence wellbeing?
Material resources (income, food, housing), social attributes (education, health, politics, social networks) and demographics (marital status, age, gender)
What are the subjective factors that influence wellbeing?
Life satisfaction, temperament, personality, affect, and attitudes. It’s how someone feels and thinks about their life.
What two variables make up emotional wellbeing?
cognitive (life satisfaction) + affect (positive and negative) reported through self report measures.
What are the two theories of what determines subjective wellbeing?
Top down theory = there is a genetic predisposition that determines subjective wellbeing baseline.
Bottom up = subjective wellbeing is determined by the accumulation of happy experiences, social support and domain satisfaction.
What are the aspects of psychological wellbeing?
Self-acceptance, purpose in life, autonomy, positive relations, environmental mastery and personal growth.
What health benefits is psychological wellbeing linked to?
Reduced disease risk, protective factor against mental illness, longer life, biological regulation, health behaviours, and biological markers of physical health
What are the dimensions of social wellbeing?
Social coherence, acceptance, actualisation, contribution and integration.
What are the problems with research methods of wellbeing?
Focus on survey based designs, evaluative studies (poor recall/biases), definitions of wellbeing differ across cultures, and most samples are WEIRD.
Mental disorders
Clinically significant disturbance in cognition, emotion. regulation or behaviour caused by genetics and environment. They are not always chronic.
What aren’t mental disorders?
Culturally approved responses, e.g. hearing voices after someone has died in Aboriginal culture OR conflict between individual and society, e.g. deviance
What do the statistics of mental health conditions show in Australia?
45% of Australians will experience a mental health condition in their lifetime w/ 20% experiencing one in a given year. 38% of GP visits relate to mental health and mental & substance disorders account for 15% of burden of disease.
Stigma
Negative perceptions of individuals or groups because of a certain characteristics/condition.
Discrimination
Acting on negative beliefs and treating individuals/groups badly.
Stereotypes
An oversimplified idea or view of an individual or group that can be negative or positive.
How is stigma and discrimination perpetuated?
Through misrepresentations in the media and news that are then adopted by communities.
Recovery based frameworks
A centred approach focusing on empowerment, autonomy and hope. The main principles are uniqueness of individual, real choices, attitudes/rights, dignity/respect, partnership/communication and evaluating recovery.
What are some of the changes to the original WHO definition?
Cope with normal stressors in accordance with severity/importance. Contribute to community when it’s welcomed and appreciated. Realise own abilities when given the opportunity by social environment. Work productively in ways that suit the individual.
Mental state exam
Structured assessment of clients behavioural and cognitive functioning. Assesses appearance, speech, behaviour, attitude, mood (self-report/subjective), affect (what interviewer observed), thought form (how thoughts are expressed) and content (e.g. delusions), perceptions (illusions and hallucinations), risk, cognition, and insight (awareness of condition)
History of asylums
Asylums were used to isolate ppl with severe mental illness or learning disabilities which contributed to stigma, public viewings, and fear. Bethlam (bedlam) is a popular example.
Biomedical approaches to mental illness
Caused by the classification of mental illness as a medical disorder which led to the development of psychiatry. Encouraged development of new medical interventions and drug discoveries.
What medical interventions and drug discoveries were made during early biomedical approaches
Lobotomies, electroconvulsive therapy (still used but more refined), insulin shock therapy (induces a coma), lithium (to treat mania), and chlorpromazine (to treat hallucinations and sedate ppl)
Four main psychological approaches to mental illness
Psychodynamic (freud) e.g. talk therapy, behaviourism (Watson) e.g. learned helplessness, humanisitc (Rogers & Maslow) e.g. self actualisation, and cognitive (Beck) e.g. maladaptive cognition/emotion.
How has the classification of mental illness in the DSM changed and why?
Removed: Homosexuality and gender identity disorder
Added: internet gaming addiction, hoarding disorder, and pre-menstrual dysphoric disorder. These changes stem from research and social changes that develop our understanding.
How has the language around mental illness changed?
No longer label person by mental health diagnosis, less use of behavioural descriptions as labels e.g. crazy or lunatic, and less use of derogatory terms e.g. schizo.
1981 Richmond report
Inquiry into mental health services that found serious abuse. This led to deinstitutionalisation and establishment of multidisciplinary community mental health teams (poorly funded and executed).
1993 Burdekin report
Inquiry into human rights of people with mental illness that recommended mental health care should occur in less restrictive settings and people with mental illness should be able to live in the community.
2014 National Mental Health Commission report
Identified that regional and rural communities experience higher mental health problems but receive less funding.
2005 Not for Service report
Human rights commission that recommended better funding and resources for mental health services.
Summary of the results from mental health care reports
Deinstitutionalisation, decrease in psychiatric hospitals, seperation of developmental disability services and mental health services, support for people with mental health disorders living in the community, and development of integrated community services.
What are the fundamental principles of mental health legislation
Protecting human rights, guarding safety of people with mental health conditions and the community, ensuring treatment in least restrictive environment and promoting individual autonomy/choice of lifestyle.
Mental health Act (2007)
Provides a legal definition to assist in providing care for people with mental illnesses or disorders through community care facilities either voluntarily or involuntarily (rare) while protecting their civil rights, health and the health of others (i.e. risk assessment), and facilitating involvement of carers/guardians. Legal definition is different to DSM diagnosis and mainly used for involuntary care.
Mentally ill (legal definition)
(A) Serious impairment (temporarily or permanently) to mental function demonstrated by one or more symptoms: delusions, hallucinations, serious disorder of thought or mood, and repeated irrational behaviours + reasonable grounds that care of person is nesscary to protect them or others from serious harm.
(B) OR person has continuing condition that is likely to deteriorate and cause A.
Mentally disordered (legal definition)
Individuals behaviour is irrational that it justifies care for individual to protect themselves or others from serious physical harm e.g. suicide.
What does the assessment of being mentally ill/disordered involve (mental health act)
First assessment by medical officer: if found mentally ill → admitted into care
Second assessment by medical officer: if first officer isn’t a psychiatrist second must be → if found not mentally ill then lead to third assessment
Third assessment by medical officer: final decision = released or detained as an assessable person.
What happens after assessment of being mentally ill (mental health act)
a) Detainment i.e. given treatment without consent b) must be reviewed by a tribunal and can have medication administered unconsentually
Mental health review tribunal: final decision with consideration for least restrictive environments + patient can’t be kept in facility for more than 3 months.
APS code of ethics
Respect for rights and dignity, propriety, and integrity. Ensures safety of clients and maintains integrity and standards of the profession.
What are two examples of ethical issues?
An individual right to autonomy can be overrided by the responsibility of psychologists to do no harm e.g. mandatory reporting. Informed consent can be affect if individual doesn’t have capacity to make informed decisions.
Informed consent
Individual fully understands nature, purpose, risks and benefits of doing or not doing an intervention.
What are the characteristics of capacity and competence.
Individuals capacity and competence may be affected when: impaired/disturbed mental functioning e.g. alcohol or level of competence doesn’t match the severity of the medical decision e.g. children. Competence is only applied to one decision and incapacity may be permanent, temporary or partial.
Substitute decision-making
Another person/organisation has legal power to make decisions on someones behalf.
Person responsible = someone you know aids you with decision making
Guardian = legally appointed to make decision on your behalf (only applies to ppl over 16)
Ethical decision making: Practice-based model (Corey)
Identify problem or dilemma
Identify potential issues involved
Review relevant ethics codes and own values
Know applicable laws and regulations
Obtain consultation
Consider possible and probably courses of action
Consider consequences of various decisions
Choose best course of action
Six questions in ethical decision making
Fairness (would you do same to others), universality (would you recommend decision to a peer), publicity (what is decision was made public), moral traces (uncertainty), reversibility (would you want decision applied to you), and mentor test (would someone you respect do the same)
Approaches to assessment and structured tools to inform diagnosis.
4 R’s, psychological formulation (5 P’s), BioPsychoSocial formulation/model, Mental State Examination and clinical risk assessment. Tools = psychometric tools, diagnostic manuals, and appropriate training of professionals.
4 R’s of assessment
Reflection = psychologists need to be self-aware, reflect on performance and develop practice
Relationship = should be collaborative, person-centred care, therapeutic relationship/rapport and unconditional positive regard
Recording = record information with a focus on the key aspects and best outcome for client
Reporting = ensure they report findings of assessment ot support best outcome for client
Psychosocial formulation
Co-constructing hypothesis of the origins of a person’s difficult/condition to increase understanding of clients situation and trust.
5 P’s of psychological formulation
Presenting problem = specific condition or broad symptoms that client wants to be addressed
Predisposing factors (long term) = areas of that increase risk of presenting problem e.g. genetics
Precipitating factors (short term) = stressors/events that trigger symptoms e.g. developmental transitions
Perpetuating factors = factors that exacerbate problem e.g. finacial stress
Protective factors = factors that counteract the problem and factors e.g. clients competency, skill or support.
BioPsychoSocial formulation
Generates hypotheses about causes of patients symptoms by considering biological, psychological, and social factors.
Pros = provides comprehensive approach to healthcare
Cons = lacks clear guidelines and limited empirical evidence
Examples of predisposing factors in Biopsychosocial model
Biological = Family psychiatric history, toxic exposure in utero, neurodevelopmental history, & temperament at birth.
Psychological = Attachment styles, family structure, low self-esteem, childhood trauma & negative cognitive styles.
Social = Poverty, low SES, poor access to healthcare, childhood exposure to domestic violence, immigration history, discrimination, and racism.
Examples of precipitating factors in Biopsychosocial model
Biological = Medical illness/injury, increased use of substances, medication non-adherence, pregnancy or hormonal changes and sleep deprivation.
Psychological = Cognitive distortions, grief, loss, emotional dysregulation, and transitions.
Social = Interpersonal trauma, work/academic/financial stressors, loss of supportive services or loved ones.
Examples of perpetuating factors in Biopsychosocial model
Biological = Chronic illness, lack of treatment, substance use, & suboptimal medication
Psychological = chronic negative thoughts, emotional dysregulation, & poor distress tolerance.
Social = Unsupportive relationships, dangerous neighbourhoods, poor finance or occupation conditions, isolation, & trans-generational problems e.g. immigration
Examples of protective factors in Biopsychosocial model
Biological = good overall health, absence of family psychiatric history, medication adherence, or above average intelligence.
Psychological = Good self-esteem and coping skills and ability to be reflective, & empathetic
Social = Positive relationships, supportive community, financial/disability support, & positive religious beliefs.
Clinical risk assessment
Identify risk factors to inform persons immediate risk and care plan. E.g. suicidal thoughts are risk factor for suicide which might require hospitalisation.
Psychometric tools
Standardised measurements with high reliability and validity that can measure cognitive ability, personality, and behaviours. E.g. Wechsler Adult Intelligence Scale and the Depression Anxiety and Stress Scale.
Diagnostic manuals + two examples
Provide clear diagnostic criteria (threshold or spectrum) to guide clinical practice, research, education and, improve communication among professionals. They help with prevention, management, and assessment of improvement.
ICD = includes mental health section that considers symptoms and social circumstance
DSM-5-TR = evidence based consensus document that defines mental disorders
Clinical interviews
Helps to identify stressors, experiences, and emotional processes to understand someones condition, symptoms, and help develop a care plan. Interviews can be loosely structured or more structured (e.g. involving tests) depending on severity or difficulty of condition.
Necessary skills for clinical interviews
Attending behaviour, directive and non-directive listening (active listening), directive action responses, developing rapport, using understanding/supportive language, let patient descirbe own experiences and lightly challenge beliefs.
Culture
Accepted pattern of knowledge, beliefs, norms, attitudes and behaviour combined with shared history and tradition. It shapes peoples lives and informs how they understand the world e.g. health
Cultural views of health
Western = health is an absence of disease with a focus on biology
Indian = health is harmony between body, organs, mind, & world
Chinese = health is balance between yin (hot) and yang (cold)
Challenges in cross-cultural communication
More distant cultures can make communication hard, interpreters aren’t always available/effective, misunderstandings of each others social systems which increase risk of breaking cultural rules and risk of misinterpretation
Cultural proficiency continuum
Cultural aversion = hating other cultures
Cultural incompetence = doing the wrong thing
Cultural blindness = “i don’t see culture”
Cultural pre-competence = surface level/performative activism
Cultural competence = have necessary skills but not mastered
Cultural proficiency = involvement, reflection, and mastery
Culturally informed approach
Person and family centred, self-disclosure, initial connection, shared understanding, respectful, non-judgemental, informed curiosity, seek knowledge on cultural differences, deal with complexity and ambiguity, and understand clients cultural and individual beliefs.
What aspects of healthcare can cultural competence improve?
Research = operationalise variables cross-culturally and allow for higher external validity
Clinical care = integration of cultural factors into assessment and treatment
Education = open-mindedness and new perspectives
Six factors of culturally competent mental health care
Ask about individuals understanding of illness
Don’t push labels or use jargon
When appropriate describe mental illness as a biological disorder
Ask about customs/practices and whether they should be involved in treatment
Request referral for mental health provider that speaks clients language/is from same background
Don’t use family members as interpretors
Culturally appropriate assessments
Should consider the SEWB framework, cultural factors within biopsychosocial model, cultural explanations for the illness and the cultural elements of relationship between client and practitioner.
Culture bound syndrome
Recurrent, locality-specific patterns of abnormal behaviour that may or may not be linked to a particular diagnostic category and that could be explained culturally. E.g. being sung/ having “bone” pointed, longing for country, wrong-way relationships, Sorry time and cuts and spiritual visits.
Six principles for practitioners supporting indigenous communities
Respect the strong connection to land, Country, ancestor and spirits
Respect for Elders in decision making and knowledge sharing
Role of Aboriginal Health Workers in linking professional to the individual, family and community
Importance of family
Importance of community and community roles
Importance of humour
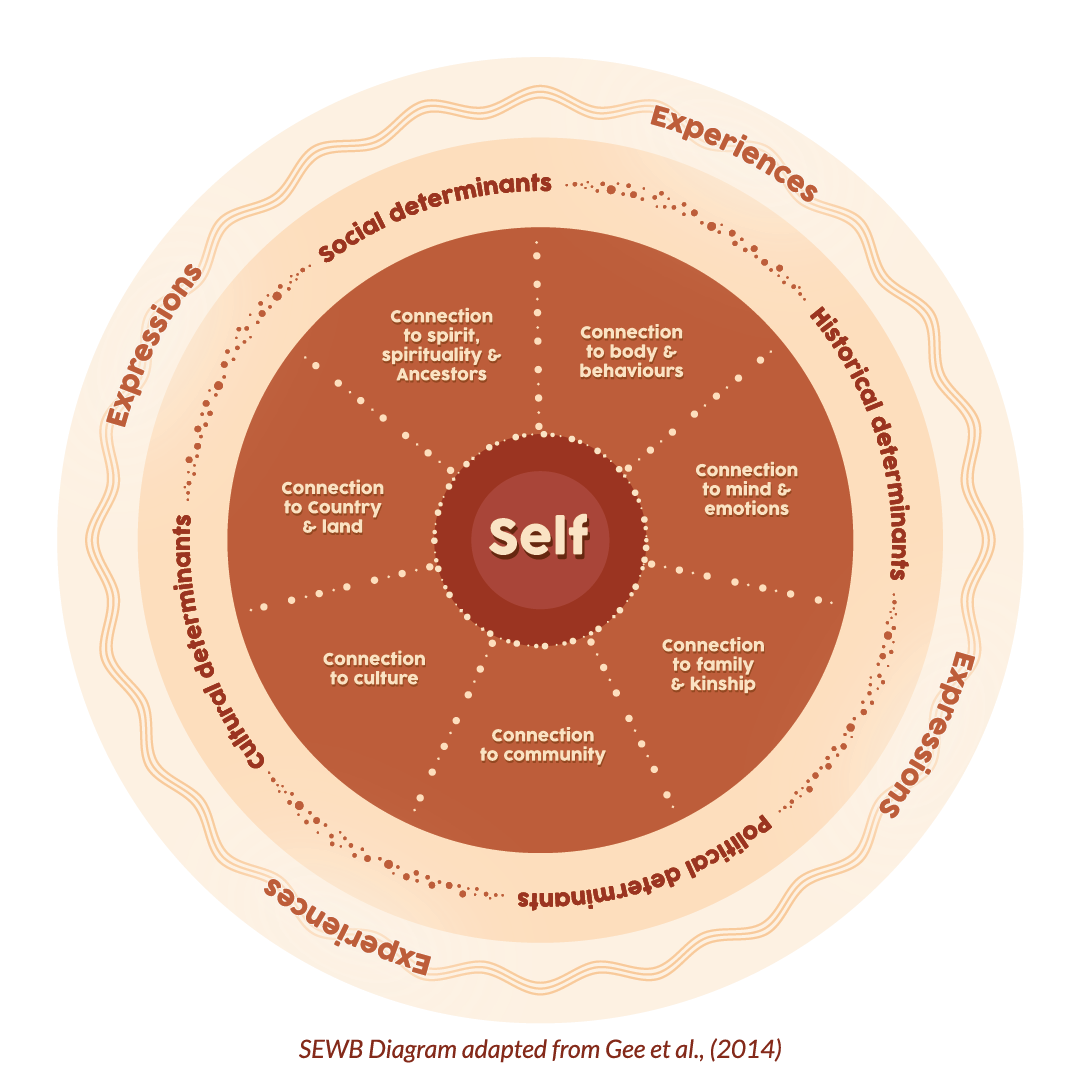
Social, emotional, wellbeing framework
Guidelines for working with Indigenous Australians (National Strategic Framework)
Health is holistic, land is central to wellbeing, self-determination, culturally valid understanding, trauma and loss is caused by disruptions of cultural wellbeing, human rights must be respected, racism, stigma, environmental adversity and social disadvantage are ongoing stressors, importance of family, sharing, and reciprocal affection, multiple cultural groups and languages, and recognition of strength.
Collective trauma
Trauma experienced by groups who may share distress and symptoms.
Intergenerational trauma
Trauma is passed down from one generation to the next e.g. through parenting
Transgenerational trauma
Trauma is transmitted across no. of generations e.g. skipped one generation
Single incident vs complex trauma
Single incident = one-off event
Complex = repeated threats often involved attachment figures e.g. abuse, neglect, and domestic violence.
The ways of working model of engagement (Ranzijn, McConnochie and Nolan)
Engage with community
Establish context
Establish rapport
Define problem
Develop communication strategies
Decide tools (assessment/diagnosis)
Implement response (intervention/treatment)
Evaluate outcomes
Percentage of Indigenous Australian psychologists
1%
Vouching
When a member of an Indigenous Australian community vouches for a psychologist to help them engage with the community.
Longing for country
A set of symtpoms Indigenous Australians might experience when they are not on their home country. E.g. pervasive sadness, lack of motivation, nausea, general sickness, somatic complaints, dissociation and distress. It is often mistaken as a major depressive episode.
High-context communication
Telling stories to explain what’s happening to the client and using the contexft of the story to help people connect to what is happening.
Sorry time
Important time of mourning involving responsibilities to attend funerals and participate in cultural events with the community.