psychosis and developmental trauma
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
people with psychosis die earlier than those who do not have psychosis
true
death 20 years earlier
life-limiting diagnosis
huge progress in other disorders and illnesses
why may someone with psychosis have a lower life expectancy?q
suicide
cardiovascular disease and other comorbid physical health problems
shared risk factors with psychosis: e.g. SE deprivation
increased rates of health-damaging behaviour
state of psychosis itself is very stressful and traumatic, and places strain on the body
what characterises schizophrenia spectrum disorders?
fundamental and characteristic distortions of thinking, perceptions and affect
what are the key symptoms of psychosis in schizophrenia?
thought interference and sonorisation (thoughts being heard out loud)
3rd person hallucinatory voices
passivity (somebody is controlling thoughts or actions)
thought disorder
negative symptoms
what are the characteristics of paranoid schizophrenia?
clinical triad of paranoia (feeling very threatened, others are actively trying to harm me)
delusions: beliefs held despite contrary evidence
hallucinations
can be very negative content, distracting
how may hallucinations and delusions arise after trauma?
experience of childhood trauma alters the ability to tell what is coming from inside and outside the mind
what was hysteria characterised as in the past?
mix of medically unexplained physical symptoms and high levels of anxiety
the association between early life experiences and MHDs have been identified historically
true
Dr. Pierre Janet proposed that early life experiences were contributing to this (around the time of Freud)
Freud: advanced the idea that sexual trauma can contribute to mental disorders in adulthood
Ferenczi: first to suggest psychosis and sexual abuse are related
what do psychoanalytic theories suggest about the intrapsychic processes occuring between trauma and psychosis?
there may be a deficit in telling between reality and unconscious fantasy that occurs in psychosis
what do French psychoanalytic theories suggest about the intrapsychic processes occuring between trauma and psychosis?
psychosis results from a deficit in ability to learn how to symbolise
what do British psychoanalytic theories suggest about the interpsychic processes occuring between trauma and psychosis?
there is a disruption in the connection between infant and mother in terms of the info flowing between them
when the parent is abusive or neglectful, they respond to the infant with punishment or ignorance
what is the impact of developmental trauma on psychosis?
more severe psychosis
lowered response to standard treatments
more hospital readmissions
less engagement with services
30% of psychosis cases are attributable to developmental trauma
what percentage of psychosis cases can be attributed to developmental trauma?
30%
developmental trauma
trauma during childhood and adolescence
includes all forms of childhood abuse
can be perpetrated by primary caregiver or family members
does developmental trauma fit the Bradford-Hill criteria for medical causation?
meets criteria for
strength of association: strong association
consistency: consistently found
temporality: recent psychotic experiences can be predicted by preceding trauma exposure, stopping trauma reduces symptoms
dose-response effects: more severe psychotic syptoms in prospective studies and poorer treatment response
plausibility: biologically plausible
coherence: association between childhood trauma and psychosis remains while controlling confounds and reverse causality
developmental trauma does not impact neurocognitive processes
false
developmental trauma impacts a range of neurocognitive processes in a way that produces underlying latent vulnerability to psychopathology
there is evidence that experiencing childhood trauma alters brain connectivity, and this may relate to vulnerability to psychosis
there is high vulnerability during adolescence in hippocampal volume
false
there is high vulnerability during early life and adolescence
there is high vulnerability during adolescence in right amygdala grey matter volume
true
from 11-13 years old
there is high vulnerability during early childhood in PFC grey matter volume
false
high vulnerability during adolescence
what specific alterations are found in neurocognitive processing in individuals with psychosis?
altered amygdala response during threat processing
ACC hyperactivation during emotion regulation and executive functioning
blunted striatal response during reward processing
the pathway from developmental trauma to psychosis is mediated by dopamine
true
dopamine is involved in psychosis and affected by developmental trauma
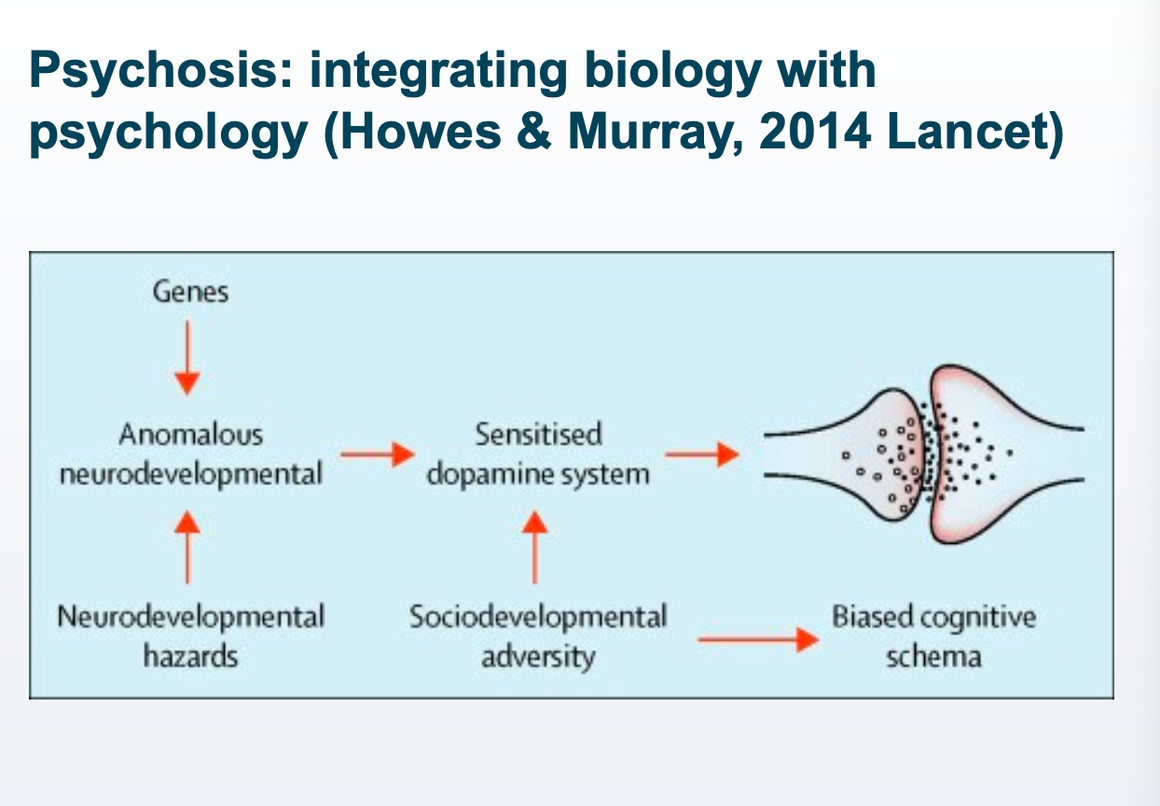
how does psychosis arise from developmental trauma?
combined genetic vulnerability and developmental trauma leads to sensitisation to dopamine system → dopamine responds to both reward AND threat
sociodevelopmental adversity on its own leads to biased cognitive schema, but is accelerated via dopamine sensitisation
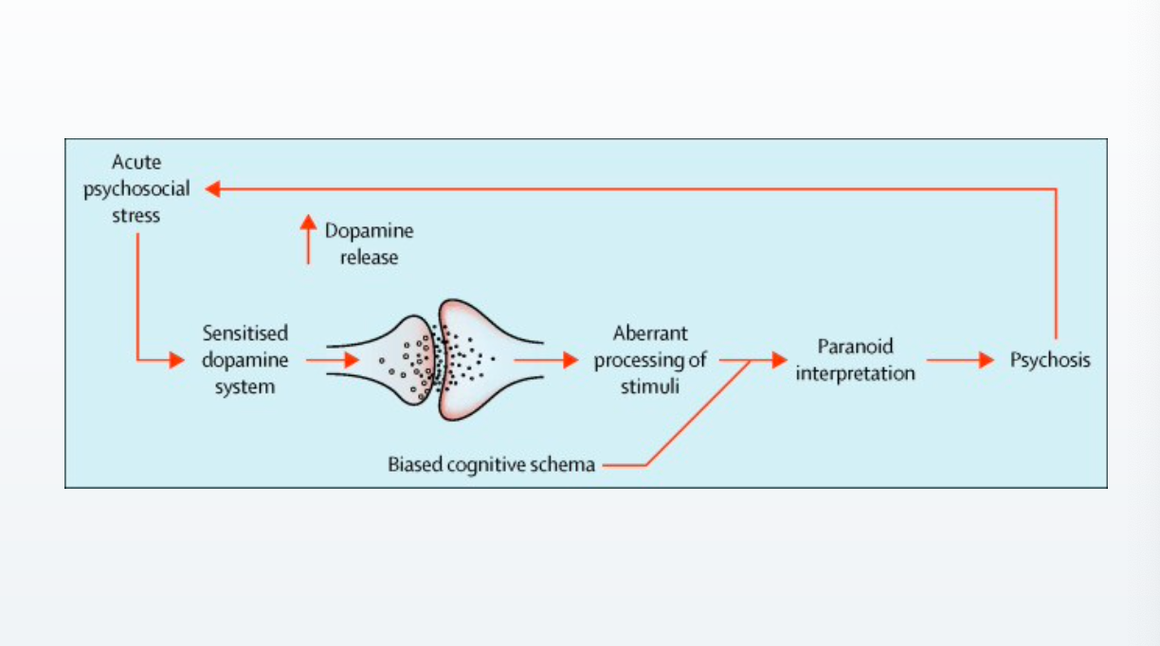
summarise how acute psychosocial stress leads to psychosis
psychosocial stress, more dopamine than normal
information processing is biased
paranoid interpretation is more readily accessible, leading to psychosis
psychosis then leads to more psychosocial stress
how does stress relate to psychosis?
corticotropin releasing factor (HPA axis: stress response system) binds to dopaminergic neurons, modulating release of dopamine during threat in the ventral tegmental area
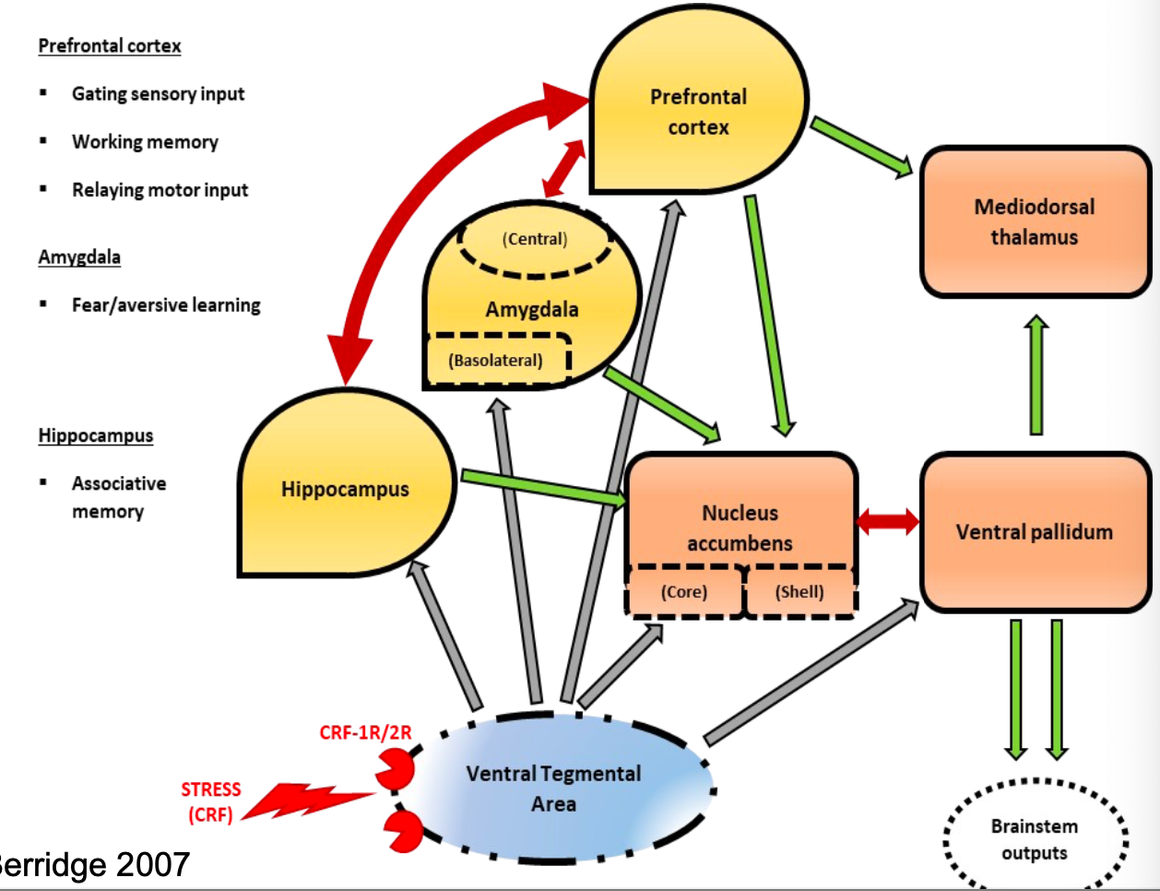
how does dopamine relate to trauma processing?
the VTA is in the brainstem, where dopamine projections come from
dopamine projections reach areas involved in trauma processing
amydala
PFC
hippocampus
when restrained, the animal experiences stress, dopamine is released and comes down again
true
dopamine has been found to become elevated in response to aversive stimuli such as restraint and pain (at least in animals)
how does dopamine alter long term potentiation?
dopamine interacts with glutamate and GABA systems (neuromodulation: longer term effect of dopamine)
dopamine has both immediate and long term neuromodulatory effect
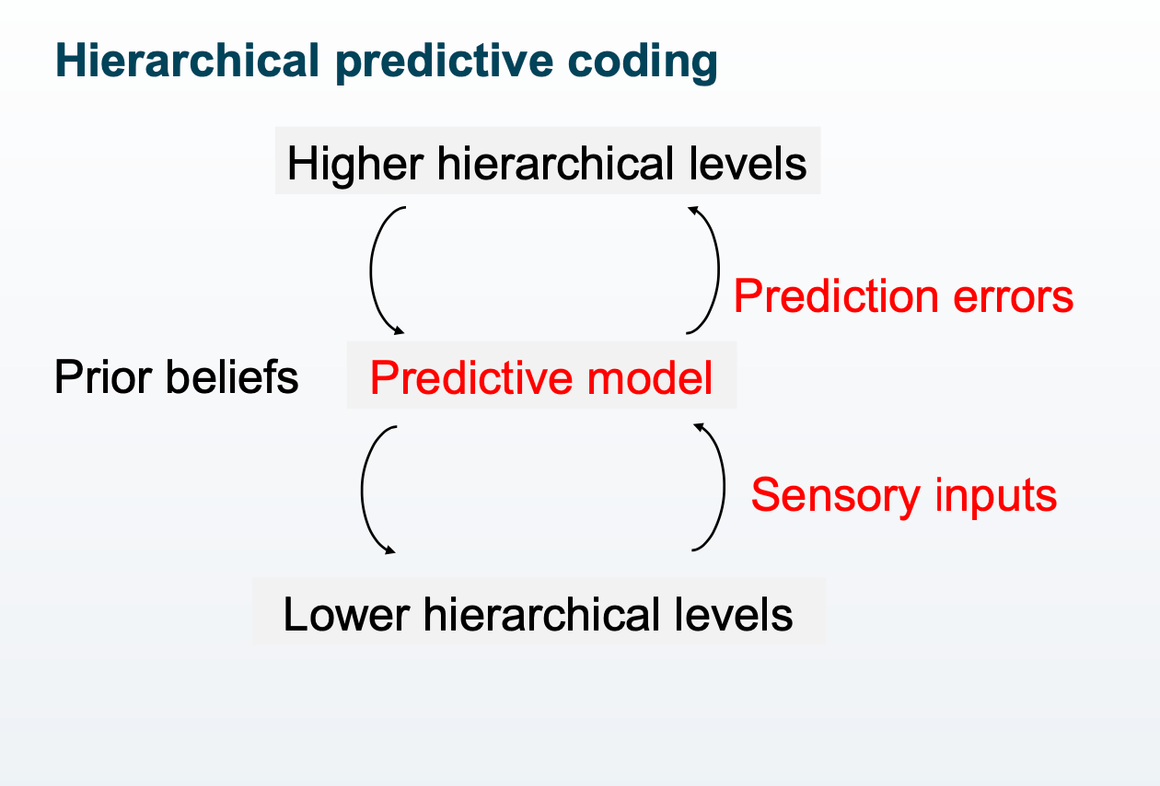
prediction errors are also dopamine activity dependent
when is there an update in prediction?
when there is a mismatch prediction and experience
this is the neurochemical basis of learning
if this process is perturbed, there may be aberrant predictions of the outside world that do not match with reality
if there is a perterbation of learning processes, your learning would cease to match reality
true
if this process is perturbed, there may be aberrant predictions of the outside world that do not match with reality
there are different levels of hierarchy in information processing
true
different levels of hierarchy in information processing
highest hierarchy can be considered to be schema
according to animal models, adolescent stress exposure leads to changes in dopaminergic function in adulthood
true
developmental stress can result in long term increases in dopaminergic function persisting into adulthood
combination of footshock and restraint stress yielded long term changes
MAM developmental model of schizophrenia
animal model of schizophrenia: developmental disruption model
displays a number of histological, neurophysiological and behavioral deficits observed in schizophrenia patients
increased sensitivity to stress during early development
there is lowered dopamine synthesis after childhood adversity in humans
true
there is a dampening of biological stress response
there is lowered dopamine synthesis after high levels of adversity experience although there are high levels of threat experience/distress
these individuals do not have psychosis, however
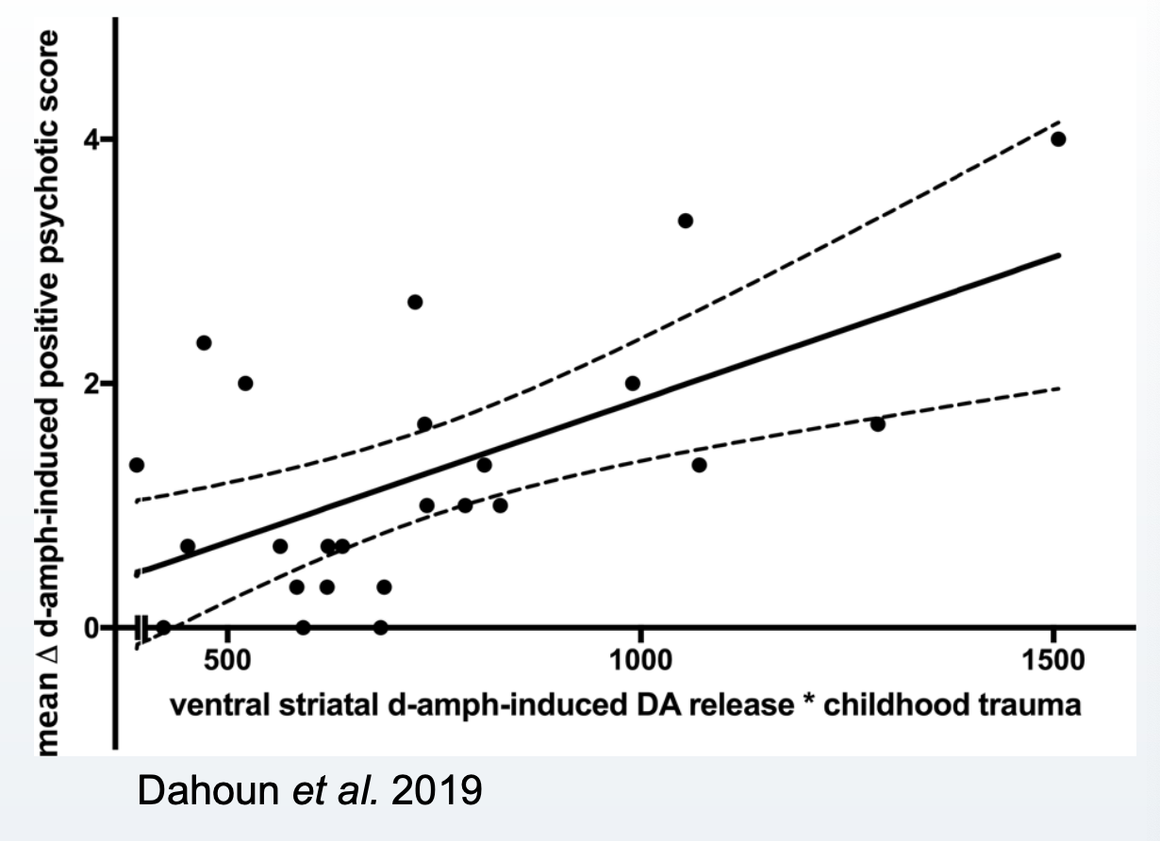
people with childhood trauma more readily release dopamine
true
greater dopamine release in response to amphetamine in those with childhood trauma
also relates to positive symptom scores
a recent systematic review has found that there are many pathways from developmental trauma to psychotic experiences
true
pathways include:
dissociation
OCD-like phenomena
PTSD symptoms
emotional dysregulation
schemata and belief systems
attachment and social cognition
what factors mediate the relationship between developmental trauma and hallucinations?
dissociative processes
OCD-like phenomena
PTSD symptoms
what factors mediate the relationship between developmental trauma and delusions?
PTSD symptoms
emotional regulation
schemata and belief systems
what factors mediate the relationship between developmental trauma and paranoia?
schemata and belief systems
attachment and social cognition
what has meta-analytic findings shown about how much dissociation, emotional dysregulation, and PTSD symptoms contribute to hallucinations?
dissociation: ES 0.35
emotional dysregulation: ES 0.06
PTSD symptoms: ES 0.12
what mediator of developmental trauma contributes highest to hallucinations?
dissociation
people with psychological trauma + psychosis have higher cortical thickness and hippocampal volume
false
people with psychological trauma + psychosis have lower cortical thickness and hippocampal volume
there are differences in clinical presentation between people with and without childhood trauma
true
more severe symptoms and links between hallucination content and trauma memory in pw psychosis + childhood trauma
how may trauma memories manifest in hallucinations in pw psychosis + trauma?
auditory memories of trauma experiences
voices relating to the perpetrator
schematised negative content
increased fear in response to voice
what do intervention studies of adult survivors of developmental trauma with psychotic and dissociative symptoms suggest are the mechanisms between developmental trauma and psychosis?
emotional regulation
attachment and social cognition
memory processing
dissociation e.g. ego disintegration
there are high rates of undetected PTSD in people with psychosis
true
around a third of pw psychosis have undetected PTSD
high rates of undetected PTSD across conditions
schizotypy
traits that predispose to psychosis
schizotypy is not a vulnerability factor for trauma memory intrusions
false
schizotypy (proneness to psychosis) is a vulnerability factor for intrusive trauma memories
what does the cognitive behavioural model of psychosis suggest about the role of developmental trauma in psychosis?
there is an interaction between:
underlying vulnerability
the ways memories are processed
how they are appraised and coped with
what are the rates of CPTSD in pw schizophrenia + developmental trauma?
70%
meeting CPTSD predicted psychosis in individuals experienced childhood trauma
there are high rates of CPTSD in pw schizophrenia and no developmental trauma
false
rates of CPTSD are very low in pw schizophrenia without DT
what are the potential mechanisms of how developmental trauma contributes to psychosis?
brain structure changes
dopamine system changes
hierarchical predictive coding changes
memory processing changes
social cognition and attachment changes
mentalisation changes and dissociation
what are important social factors in psychosis?
social isolation
high stigma and marginalisation
re-traumatisation from psychotic symptoms
re-traumatisation by compulsory treatments