4. Schizophrenia
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
What are the key symptoms of Schizophrenia?
Delusions (false beliefs about external reality)
Hallucinations (Perception in the absence of an external stimulus)
Disorganised speech
Grossly disorganised or catatonic behaviour (abnormal movement behaviours)
negative symptoms (e.g. diminished emotional expression)
How are cognitive symptoms involved in Sz?
Cognitive symptoms, including problems with attention, memory, executive function) are common, but not considered for a formal diagnosis.
What is required for a formal Sz diagnosis
delusions and/or hallucinations must be present
continuous signs of disturbance for at least 6 months
Diagram showing Schizophrenia vs other psychoses
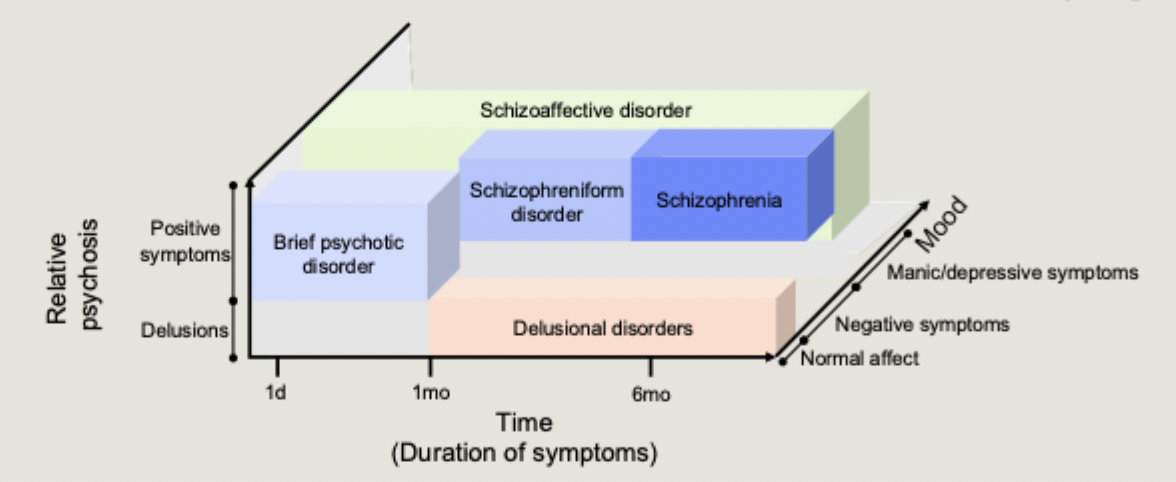
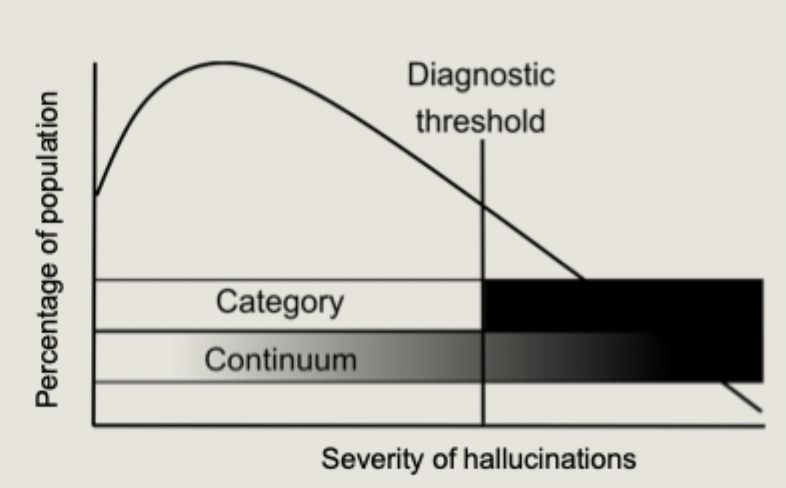
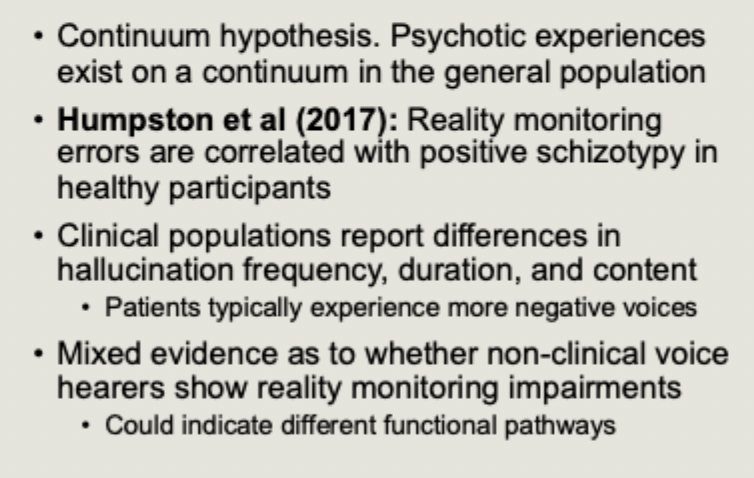
What does the continuum hypothesis argue?
argues that psychotic experiences exist on a spectrum
auditory hallucinations and delusions can occur without a schizophrenia diagnosis
What is the common misconception about Sz to do with personality?
Sz means you have split personality
however, split/multiple personalities is completely unrelated to schizophrenia
What refutes the misconception that schizophrenia patients are violent and dangerous?
higher rates of violence in schizophrenia tend to co-occur with co-morbid issues such as substance abuse disorders
people with schizophrenia are far more likely to be the victim of crimes
What refutes the misconception that bad parenting is the cause of schizophrenia?
There are a multitude og genetic and environmental factors that increase Sz risk
What refutes the misconception that having Sz means you cannot integrate into society?
Schizophrenia outcome is poor, only 25% recover enough to work and live on their own
many more people can improve to a level where they can live relatively independently
new innovations in the understanding and treatment of sz offer hope for future
History of Schizophrenia treatments diagram
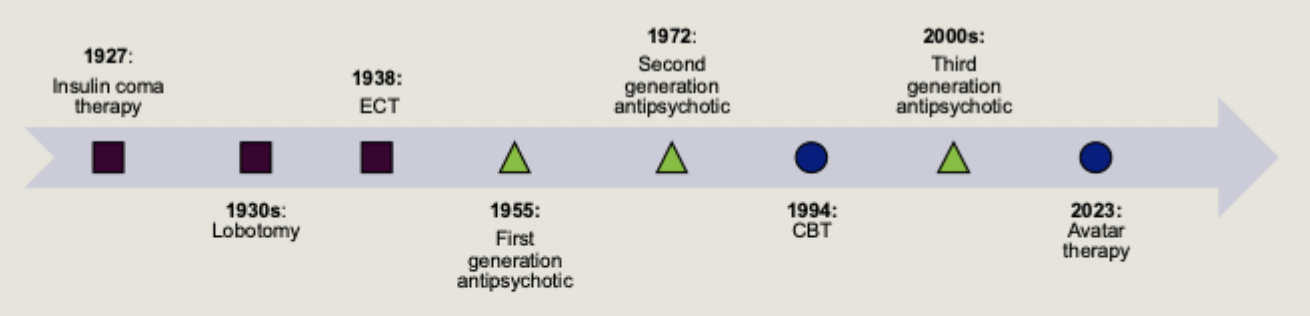
When were typical antipsychotics discovered?
discovered by accident in the 1950s
also referred to as first generation antipsychotic
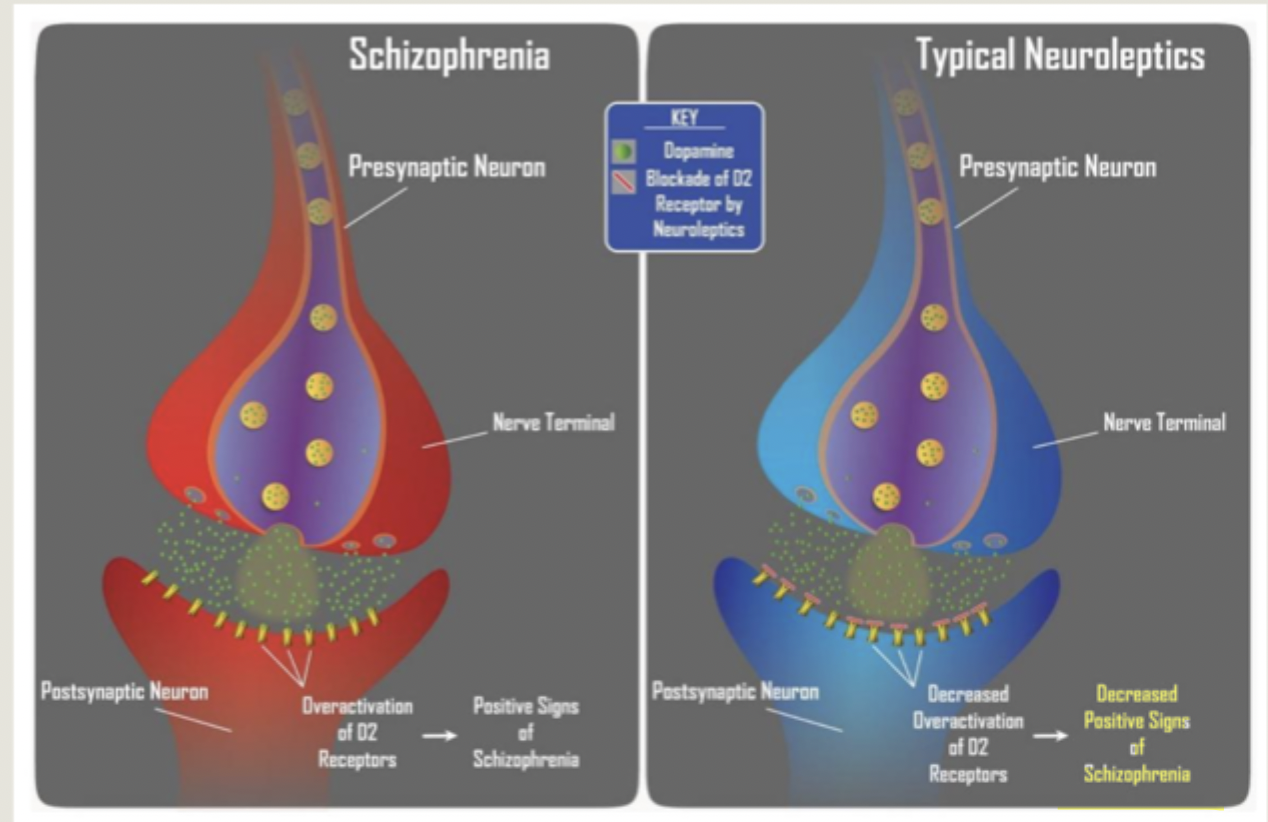
What is the primary mechanism of action and main effect of Typical Antipsychotics?
primary mechanism of action is through the blocking of D2 dopamine receptors
the main effect is a reduction in positive symptoms
When were Atypical antipsychotics developed?
developed in the 1970s-1980s
also referred to as novel or second generation antipsychotic
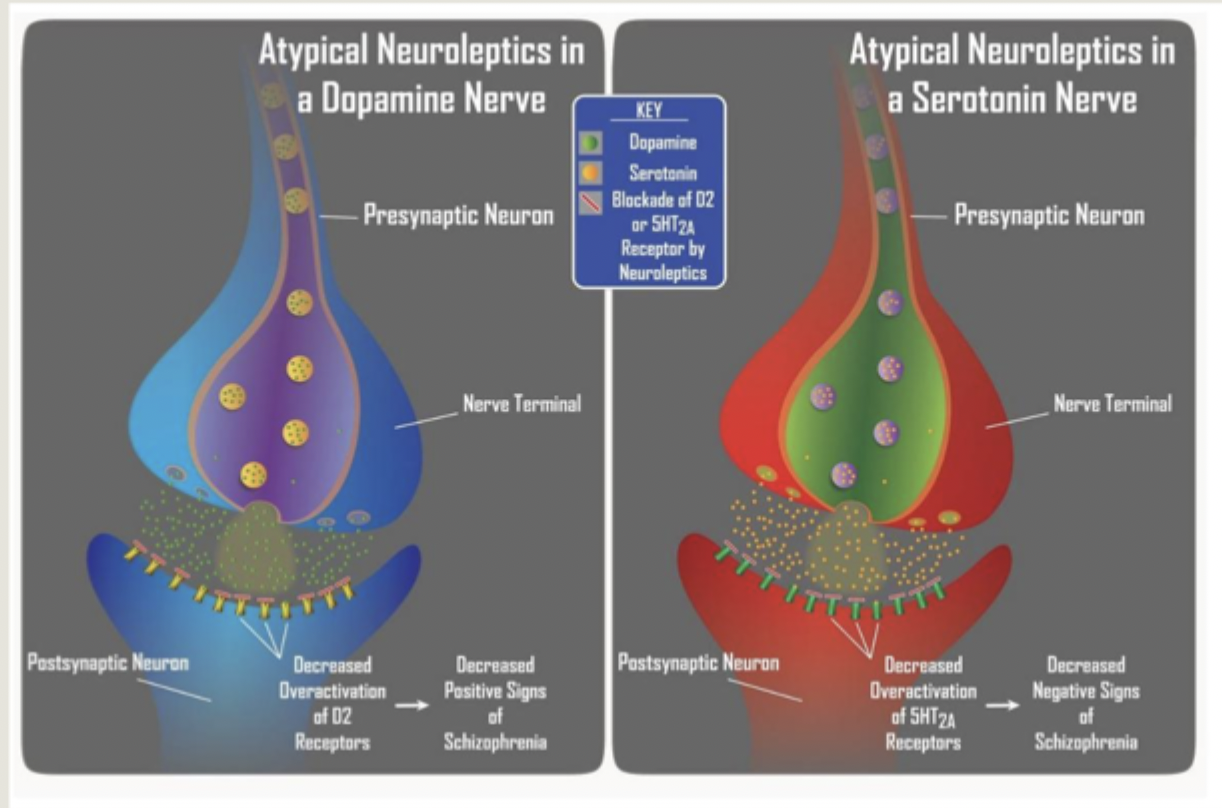
How to atypical antipsychotics work and what are their effects?
work through blocking both dopamine and serotonin receptors
appear to be more effective at reducing negative symptoms
What kind of neurotransmitter is dopamine?
monoamine neurotransmitter involved in reward and motivation
Where is dopamine released from?
released from the ventral tegmental area to forebrain network
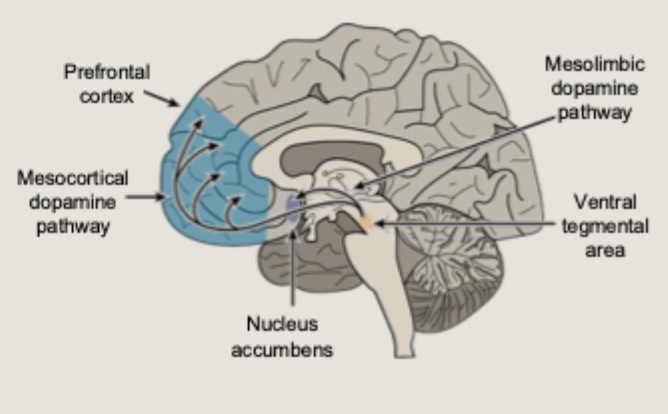
Dopamine is involved in reward processing via which pathways?
mesolimbic pathway
mesocortical pathway
How do typical antipsychotics work on dopamine?
excess of dopamine in synapse
the typical antipsychotics blocks post synaptic receptor cells so dopamine undergoes reuptake
decreased overactivation of D2 receptors leading to decreased positive symptoms of Sz
What does the dopamine hypothesis suggest about the mesolimbic pathway and Sz?
mesolimbic pathway: processing of reward/salience
positive symptoms associated with excess dopamine in this pathway
hyperdopaminergic: delusions, hallucinations, disorganised thought, speech and behaviour
What does the dopamine hypothesis suggest about the mesocortical pathway and Sz?
mesocortical pathway: attentional control and executive function
negative symptoms associated with insufficient dopamine in this pathway
hypodopaminergic: alogia, affective flattening, avolition
How do post-mortem studies evidence the dopamine hypothesis?
Post-mortem studies reveal higher counts of dopamine receptors in schizophrenia patient
How does the use of dopamine agonists evidence the dopamine hypothesis?
Dopamine agonists can trigger psychotic episodes
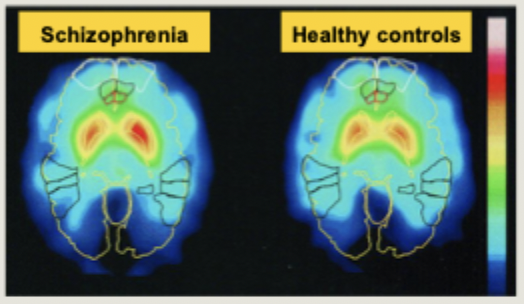
How has PET scanning evidenced the dopamine hypothesis?
Positron Emission Tomography can be used to image neurotransmitter function in living humans
PET revealed evidence of increased dopamine synthesis in the striatum of 10 unmedicated schizophrenia patients
What are the roles of glutamate and GABA?
glutamate is an excitatory neurotransmitter
in tandem with inhibitory GABA, it controls excitation/inhibition in the brain
What could be the results of drugs that block glutamate transmission?
Can induce symptoms of psychosis (e.g. ketamine, PCP)
What is the suggested role of glutamate and GABA in schizophrenia?
people with schizophrenia exhibit low levels of glutamate and GABA
proposed that excessive dopamine is driven by a lack of GABAergic inhibition, primarily cause by reduced levels of glutamate
Have the development of glutamate-based treatments been successful?
No
What is the limitation of the dopamine hypothesis involving where dopamine is increased?
dopamine is not increased everywhere in the brain, as it might suggest
evidence that dopamine levels are reduced in areas of the frontal cortex which might be linked to negative symptoms
this has led to the revised dopamine hypothesis that emphasises an imbalance of dopamine transmission across different brain regions
What is the limitation of the dopamine hypothesis regarding the negative symptoms of sz?
DH does not account for the negative symptoms of schizophrenia
typical antipsychotics are not effective at treating them
What is the limitation of the dopamine hypothesis regarding use of typical antipsychotics?
side effects
extrapyramidal syndrome is a risk with typical antipsychotics (tremors and shaking, difficulty moving and walking)
What kind of neurotransmitter is Serotonin?
a monoamine neurotransmitter
with reduced levels being implicated in depression
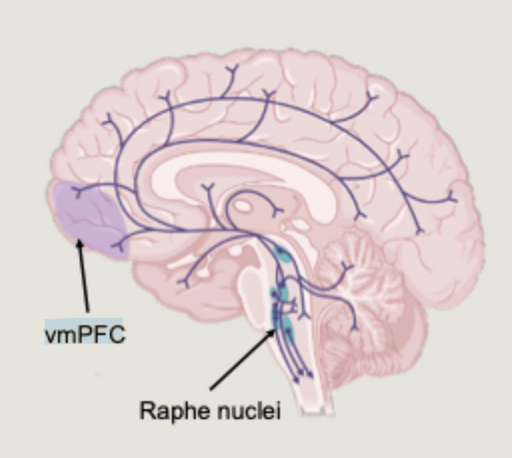
Where is serotonin generated and released to?
generated in the raphe nucleu
released throughout the brain
What might too much serotonin cause?
hallucinations (e.g. psilocybin, LSD)
How has Serotonin been implicated in Sz?
Increased serotonin has been implicated in the negative symptoms of schizophrenia
especially in pre-frontal regions
discovered through the mechanism of atypical antipsychotics
How to atypical antipsychotics work?
Blocks receptor cells to reduce both serotonin and dopamine
Are antipsychotics effective?
reductions in positive and negative symptoms
but non-response rates as high as 30%
cognitive symptoms are minimally effected
Can we compare typical and atypical antipsychotics?
there is no consistent evidence that atypical antipsychotics outperform typical antipsychotics
atypical antipsychotics produce fewer extrapyramidal side effects
other common side effect: weight gain/ diabetes/ sedation, nausea/dizziness, cardiovascular problems
NICE no longer recommends atypical over typical antipsychotics
What is the source monitoring framework and how do we discriminate between real and imagined?
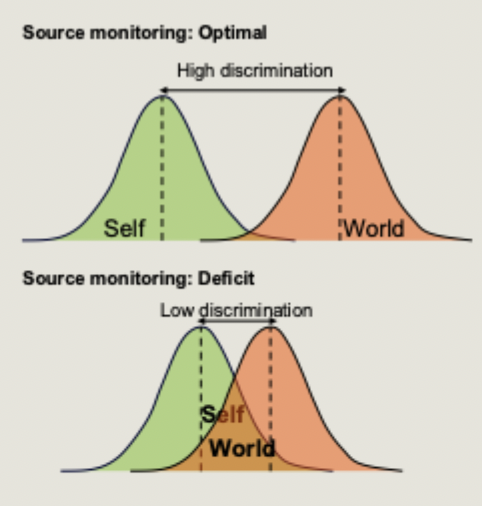
identifying the origin of a memory is a judgement call
we make attributions about the origin of an experience by considering its features
a ‘memory’ rich in visuoperceptual is judged as more likely to be real
a ‘memory’ that comprises traces of internally generated thought is judged as being imagined
What is reality monitoring?
specific types of source monitoring: determining whether information was internally or externally generated
misidentifying internally generated events as being real are reality monitoring errors
reality monitoring errors are most common for auditory information, but can occur in any sensory modality
What is the role of the Anterior pre-frontal cortex
situated at the very front of the prefrontal cortex
recent evidence suggests anterior PFC is involved in reality monitoring judgements
supports successfully distinguishing between internally and externally generated information
What is the neural basis of auditory hallucinations?
activity in superior temporal gyrus
what is the neural basis of visual hallucinations?
Extrastriate cortex
How can hallucinations be explained by perception processing deficits?
Hallucinations are unusually vivid internally generated experiences processed as if they were external sensory events
hallucination-prone individuals may have difficulty discriminating perceived and imagined information
What did Vinogradov find when examining reality monitoring ability in healthy controls and schizophrenia patients?
patients showed specific impairment in recognising the source of self-generated items
during reality monitoring trials, patients showed reduced activation in anterior PFC
Which group of patients did Brunelin et al suggest impairments in reality monitoring were specific to?
Only seen in patients who experience hallucinations
What was the method of Subramaniam et al (2012) who used a non-pharmacological intervention to try and improve reality monitoring in patients?
Intensive 80hr of cognitive training over 10 weeks (50 hour auditory/30 visual)
patients told to make progressively more accurate discriminations regarding auditory/visual stimuli
control group played computer games
What were the findings of Subramaniam et al (2012) who used a non-pharmacological intervention to try and improve reality monitoring in patients?
Cognitive training led to improved reality monitoring that correlated with increased anterior PFC activity
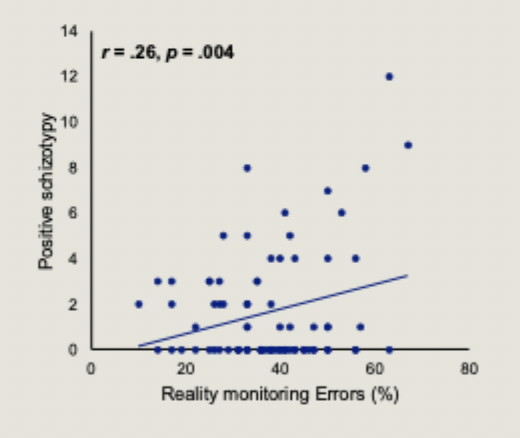
What did Humpston et al find regarding reality monitoring erros and positive schizotypy in healthy participants?
they are correlated
Reality monitoring in non-clinical voice hearers slide
How are cognitive deficits characterised in schizophrenia?
deficits include: working memory, attention, executive function
they predate symptoms onset and persist throughout the course of illness (ever after primary symptoms controlled by APs)
How are cognitive deficits important but how have they failed to be considered?
cognitive deficits are better predictors of functional outcome than the defining symptoms
effective treatments for cognitive deficits are lacking
cognitive testing tends to ignore long-term memory processes
How did Manoach et al demonstrate memory consolidation failures in schizophrenia?
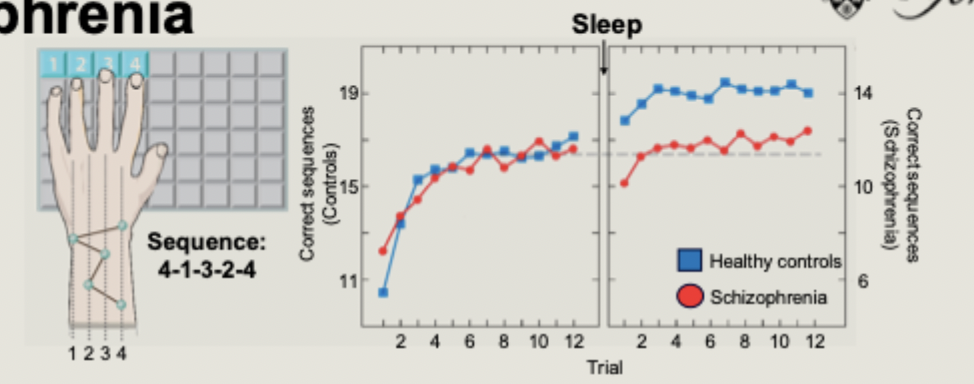
Schizophrenia patients and healthy controls performed a procedural memory test
sleep significantly improved performance in controls, but not in patients
deficits in sleep-dependent consolidation also seen for word pair association, picture recognition
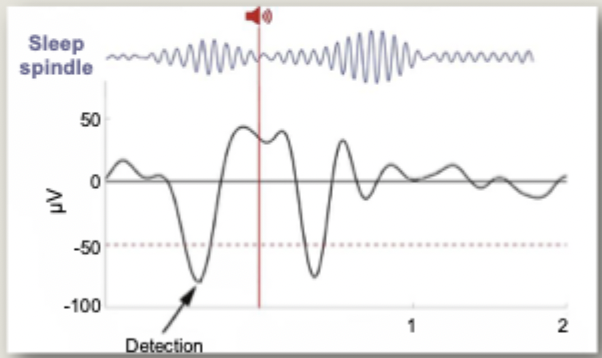
What are sleep spindles?
sleep spindles are a hallmark oscillation of NREM sleep
Where and how are sleep spindles generated?
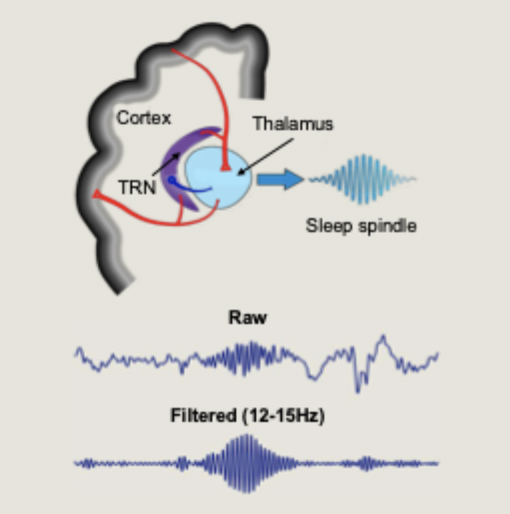
generated in the thalamic reticular nucleus (TRN)
spindles are generated through a powerful inhibition of neurons by the TRN, followed by a rebound burst firing at the spindle frequency
What are the properties of the thalamic reticular nucleus?
comprised of almost entirely GABAergic inhibitory neurons
acts as a sensory gating mechanism to control what sensory information reaches the cortex
What did denis et al find about sleep spindles in early course psychosis patients?
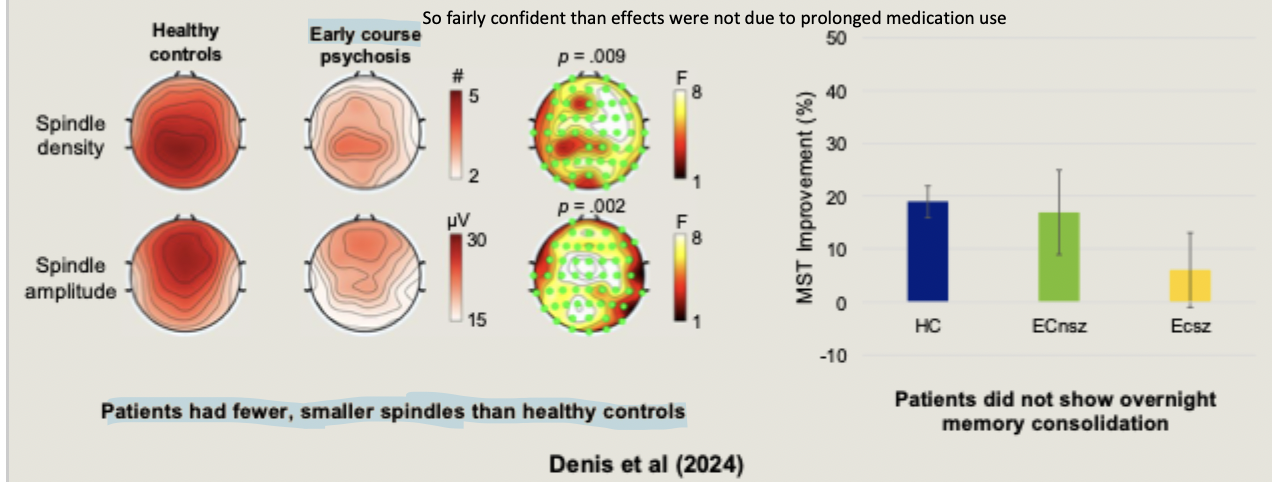
patients had fewer, smaller spindles than healthy controls
did not show overnight memory consolidation
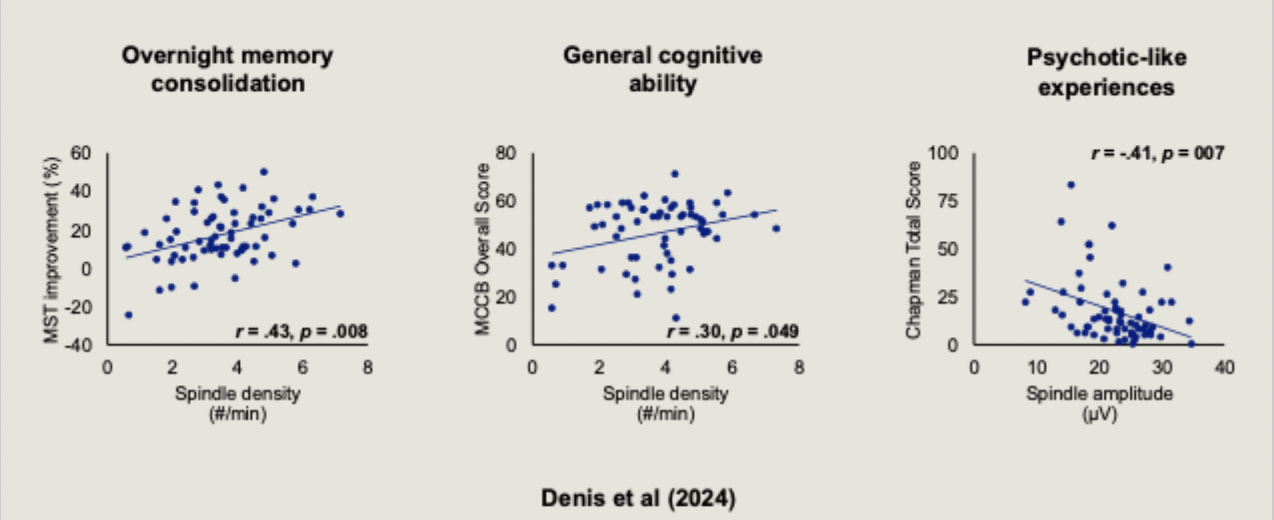
What are three factors that denis et al found sleep spindles correlated with?
overnight memory consolidation
general cognitive ability
psychotic-like experiences
with fewer spindles: suffer more from the cognitive problems of sz
What do post-mortem studies show regarding the Thalamic Reticular Nucleus (TRN) and schizophrenia?
Postmortem studies show smaller TRN in patients
the TRN is comprised of inhibitory GABAergic neurons
GABA levels are lower in schizophrenia
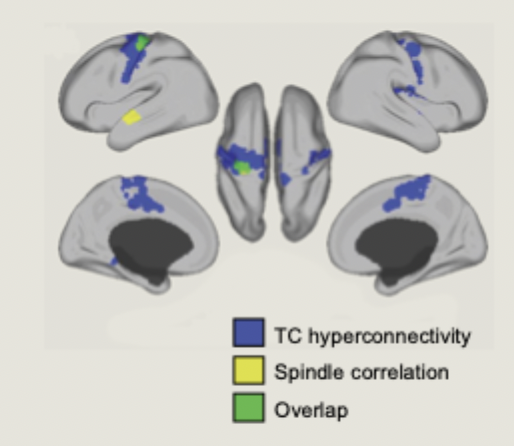
How does Baran et al suggest the thalamus is implicated in sleep spindles and cognitive symptoms of schizophrenia?
hyperconnectivity between the thalamus and the cortex in schizophrenia, correlated with fewer sleep spindles
a lack of inhibition in the thalamus impairs sensory gating and results in fewer sleep spindles, contributing to cognitive deficits
Which approaches are being investigated for treating sleep spindles to improve cognitive symptoms? what evidence proves supportive so far
pharmacological and acoustic stimulation
initial trials in healthy participants confirms that acoustic stimulation of spindles can improve memory consolidation