3. Conduction Emergencies
1/36
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
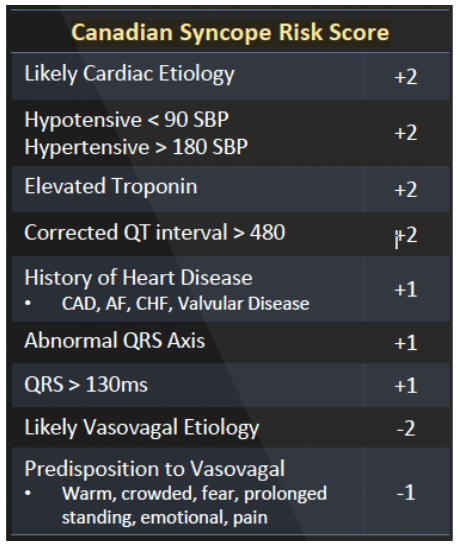
Canadian Syncope Risk Score
<1 → discharge
1-3 → admit if unstable or unresolved sx
>4 → admit
explain axis deviation
I UP & aVR DOWN → Leaving each other → Left
I DOWN & aVR UP → Reach for each other → Right
Both UP → 2 thumbs up → normal
SVT treatment
Pediatrics
1st line = Valsalva Maneuver
2nd line: Adenosine
Adults
Adenosine
Refractory: Beta Blockers or Calcium Channel Blockers
Afib/Aflutter Rate Control
Rate Control
Beta-1 Selective Beta-Blockers → Metoprolol, Esmolol
Non-dihydropyridine calcium channel blockers (NCCB) → Diltiazem (less bronchospams risk)
Digitalis glycosides (Digoxin)
if refractory to BB or NCCB
Amiodarone
if refractory to BB or NCCB
3 bolus q5min, usually done if pt not candidate for immediate electrical cardioversion (more than 48hr)
Afib/Aflutter Rhythm Control
Criteria for ED Cardioversion
new onset AF w/in 48hr
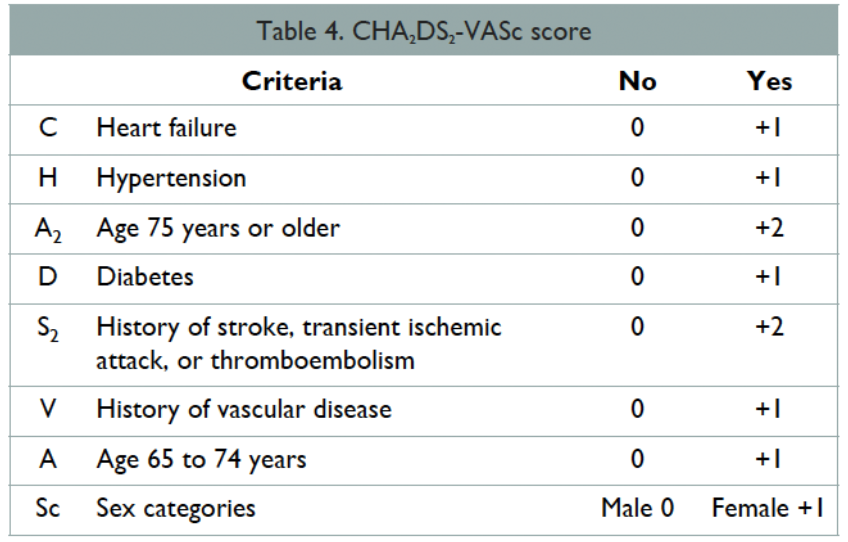
CHA2DS2-VASc score less than 1
= anticoag before cardioversion and after x 4 weeks
Delayed Cardioversion
AF > 48hr but less than 1 year
= anticoag for 3-4 wk first, then cardiovert, then anticoag 4 weeks after
Electrical Cardioversion
Pharmaceutical Cardioversion → Flecainide. Propafenone, Procainamide, Amiodarone
CHA2DS2-VASc score
Consider anticoagulation if:
Males: score > 2
Females: score >3
Anticoagulation Options
Heparin: periprocedural
DOAC: mainstay for outpatient stroke prevention
Warfarin: mechanical heal valves
who gets admitted w/ afib
Unsuccessful rate or rhythm control
Symptomatic
Unstable
tx wide regular ventricular tachycardia (monomorphic)
▸ Stable
1st line: Procainamide
2nd-line: Amiodarone
▸ Unstable
Synchronized Cardioversion
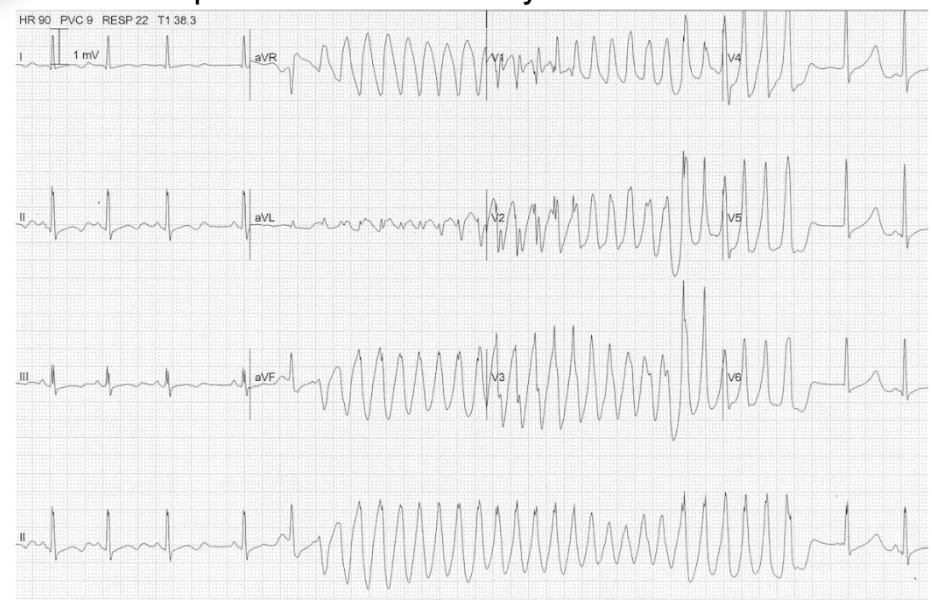
tx wide irregular ventricular tachycardia (polymorphic)
▸ Stable
1st line: Correct Electrolytes (MgSO4 IV)
2nd line: Ventricular overdrive pacing
3rd-line: Unsynchronized cardioversion
▸ Unstable
Unsynchronized cardioversion
who gets admitted w/ Ventricular Tachycardia
all get admitted
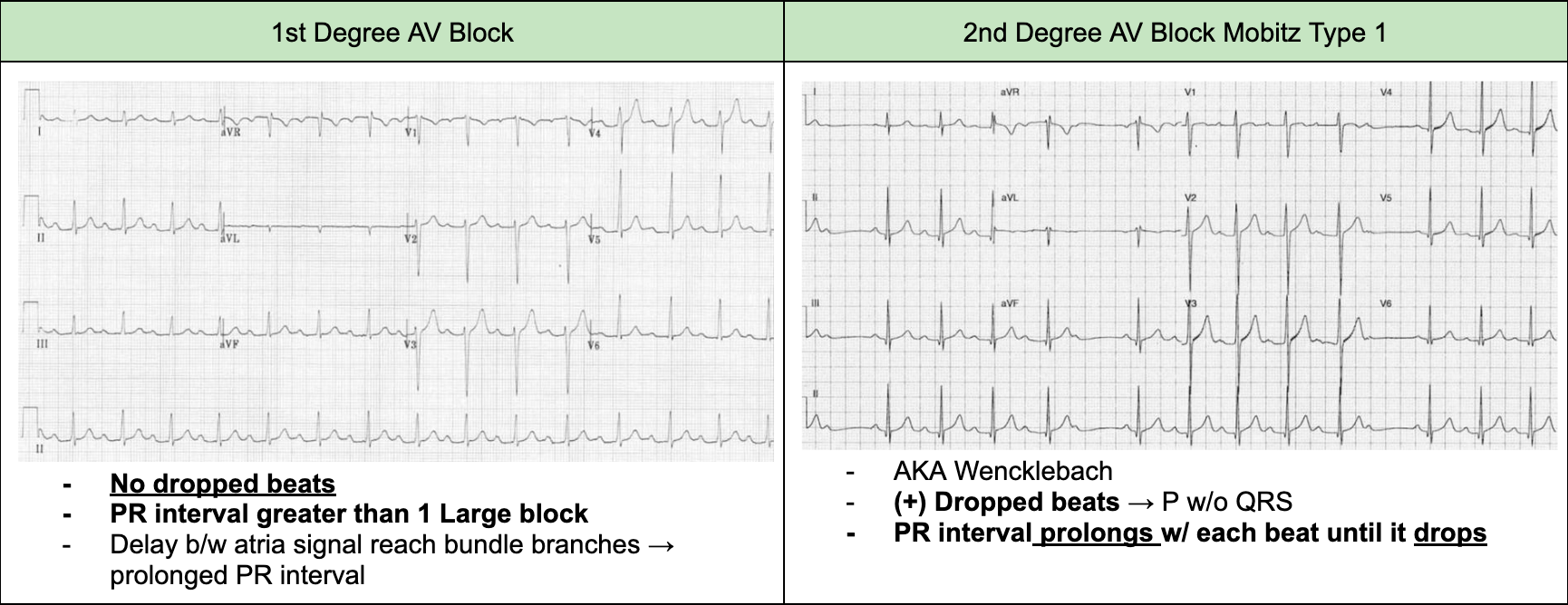
tx AV Block: 1st Degree or 2nd Degree Type I
Identify and correct any acquired pathogenesis
Require cardiology consultation if pathological
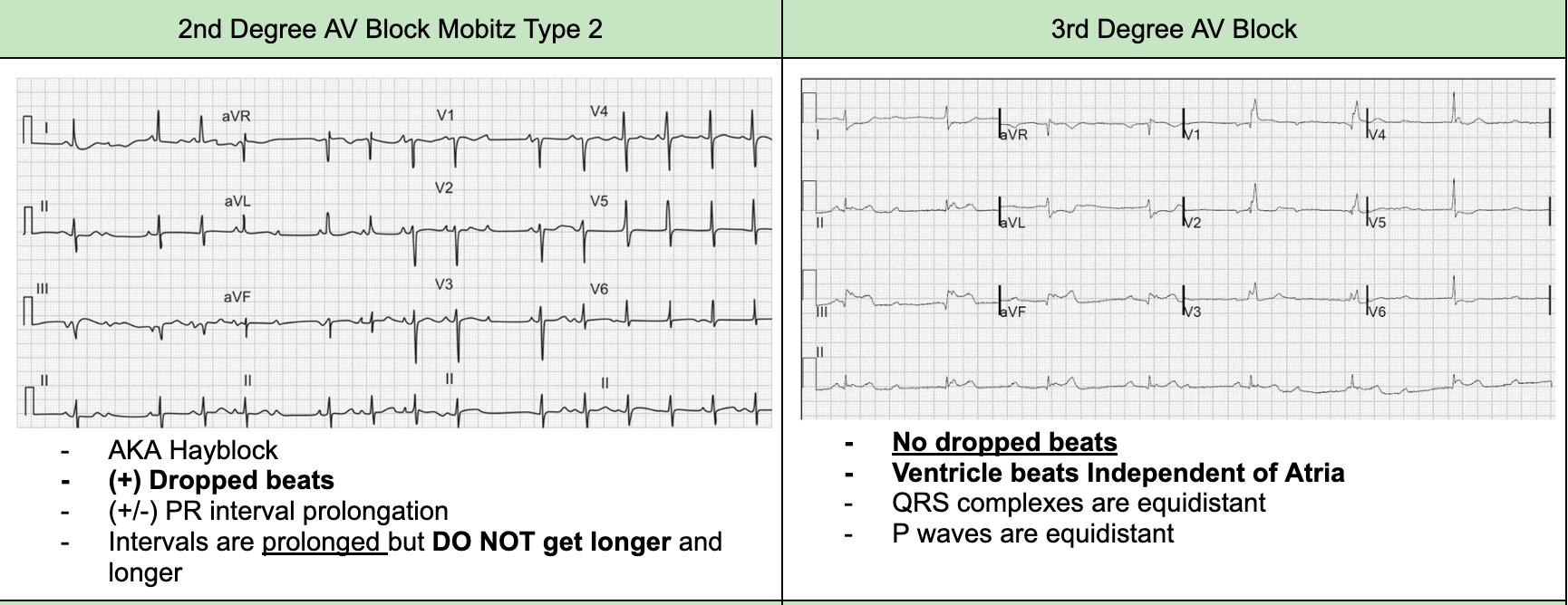
tx AV Block: 2nd Degree Type II or 3rd Degree
cardio consult to correct pathologic causation or place ICD
who gets admitted w/ AV blocks
2nd Degree Type II or 3rd Degree
Symptomatic
Pathological pathogenesis
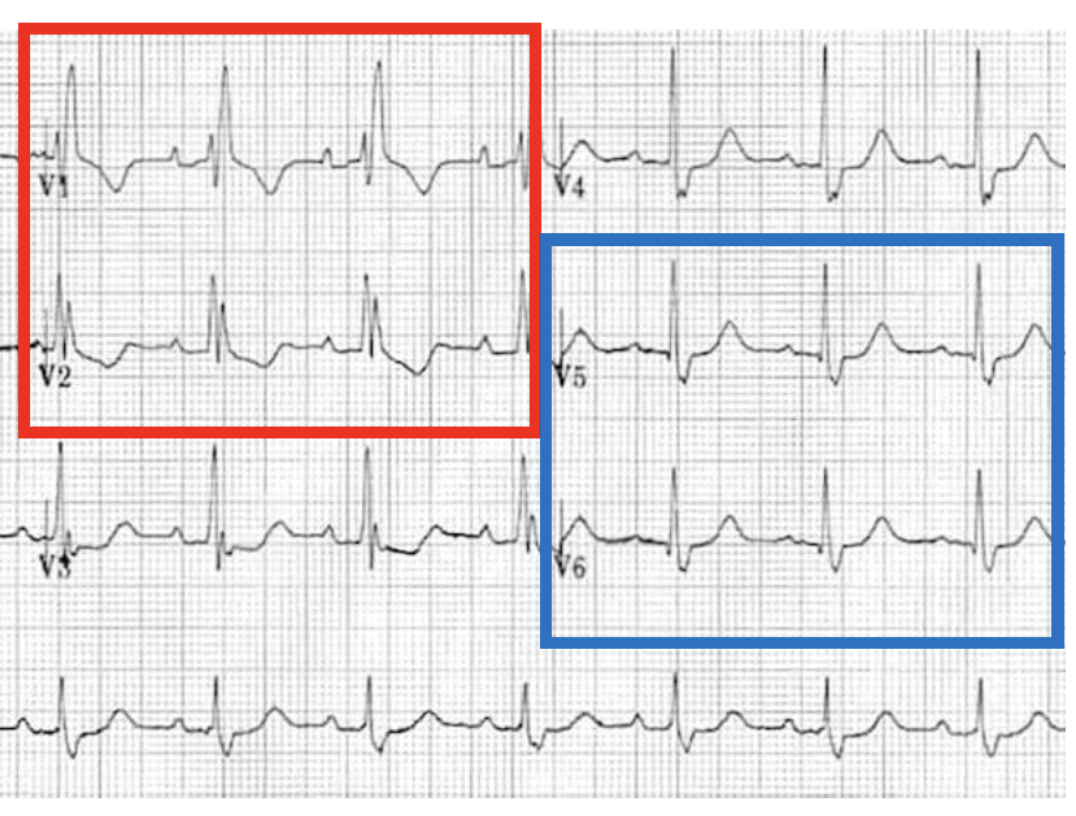
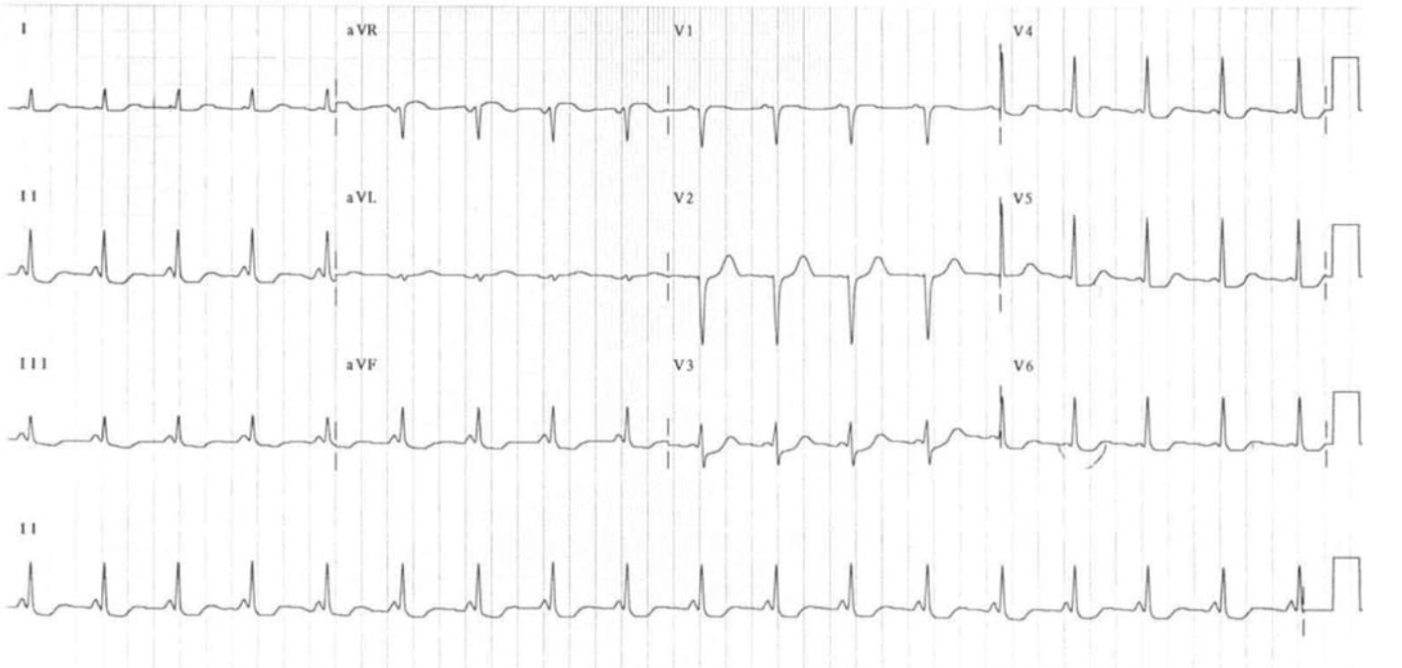
ECG findings in right bundle branch
RSR’ pattern on the right side of the heart → V1 & V2 shows a conduction delay → “bunny ears”
Reciprocal Deep S on left side of the heart → V5 & V6→ “slurred S”
ECG findings in left bundle branch
RSR’ pattern on the left side of the heart → V5 & V6 → broad monomorphic wave, "clumsy" not smooth
Reciprocal Deep S on right side of the heart → V1 & V2

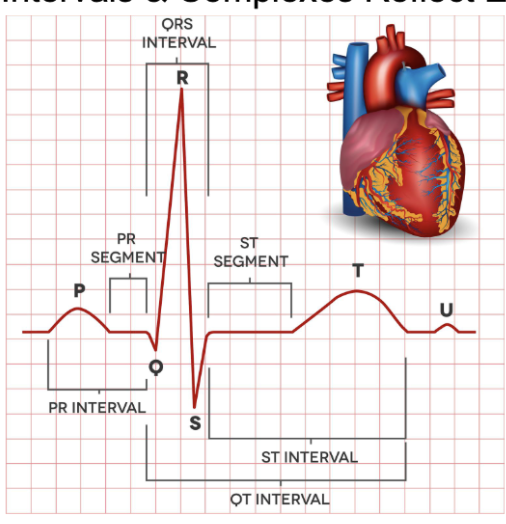
normal QT interval
~ little over 2 large boxes (<440ms)
from start of Q wave to end of T wave
what can cause prolonged QT and short QT
long - hypokalemia, hypocalcemia, hypothermia, MVP, ICP
short - hyperkalemia, hyperthermia, acidosis
what arrhythmias ca prolonged QT or short QT progress to?
long - Torsades
short - ventricular fibrillation
tx and dispo for prolonged or shortened QT syndrome
correct acquired pathologies & cardio consult for ICD if congenital
admission if symptomatic or congenital pathogenesis
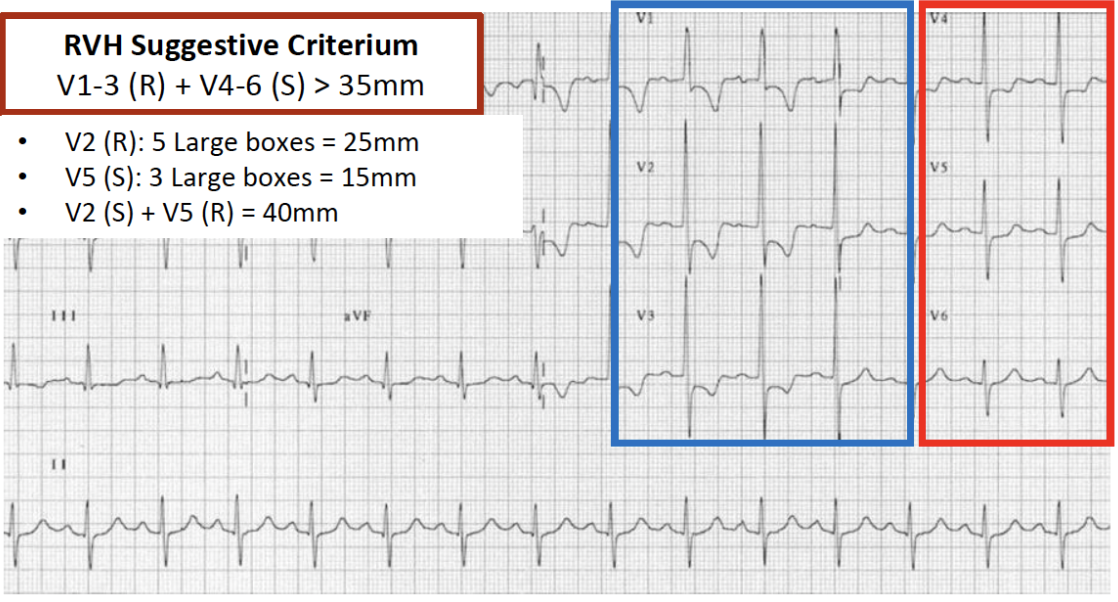
ECG findings in right ventricular hypertrophy
Tall R waves in V1, V2, V3 (right side of heart)
Reciprocal Deep S in V4, V5, V6
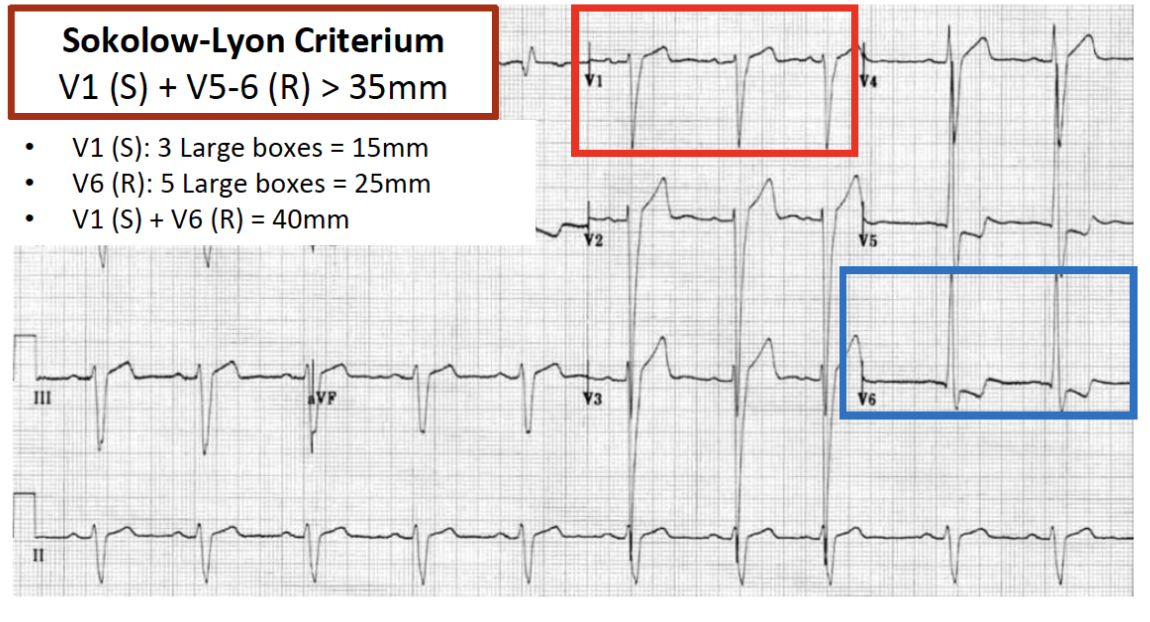
ECG findings in left ventricular hypertrophy
Tall R waves in V4, V5, V6 (left side of heart)
Reciprocal Deep S in V1, V2, V3
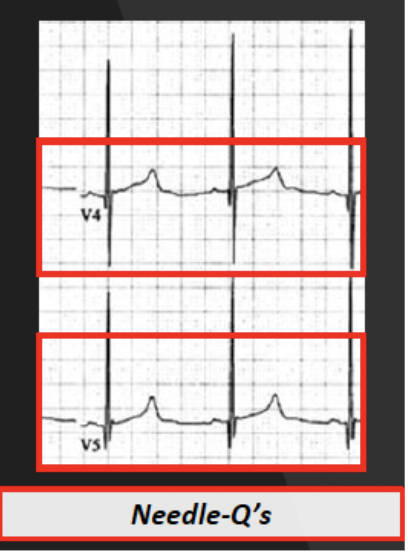
ECG findings in hypertrophic cardiomyopathy (HCM)
Needle-Q’s or Daggers of Death → Deep narrow and sharp Q waves in lateral leads (I, aVL, V5-6)
Tall R waves on left side (V5, V6) and Deep S in right side (V1, V2, V3)
murmur in Hypertrophic Obstructive Cardiomyopathy (HOCM)
Harsh mid-systolic crescendo-decrescendo murmur
Increased with Valsalva or Exertion (preload dependent)
Decreases with Squatting (increases afterload and forces tract open)
Echo finding in HOCM
Myocardial thickness > 15mm
tx for HOCM
Increase preload (to keep track open) → NS or LR IV
Increase ventricular filling (slow down heart) → Labetalol IV bolus
Increase afterload (keep track open) → Phenylephrine IV
Surgical intervention
Cardiology consultation → ICD
Cardiothoracic surgery consultation → Myectomy (if significant)
who gets admitted with HOCM, ARVD, Brugada Syndrome, or AVRT?
symptomatic or new diagnosis
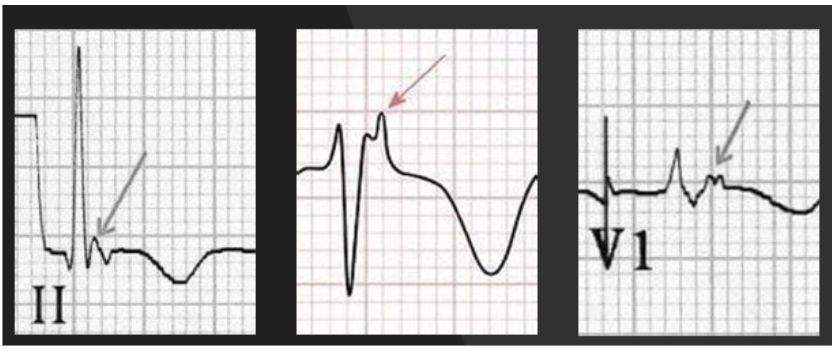
ECG finding in Arrhythmogenic Right Ventricular Dysplasia (ARVD)
Epsilon Wave (fat deposition in myocardium → conduction delay)
small deflection “blip” at the at the end of QRS complex, just before T wave
T wave inversion and prolonged QRS in V1-V3 (right side of heart)
tx for Arrhythmogenic Right Ventricular Dysplasia (ARVD)
Dual Rate and Rhythm Control → Sotalol or Amiodarone IV
Rate Control (BB) → Metoprolol IV or Esmolol IV
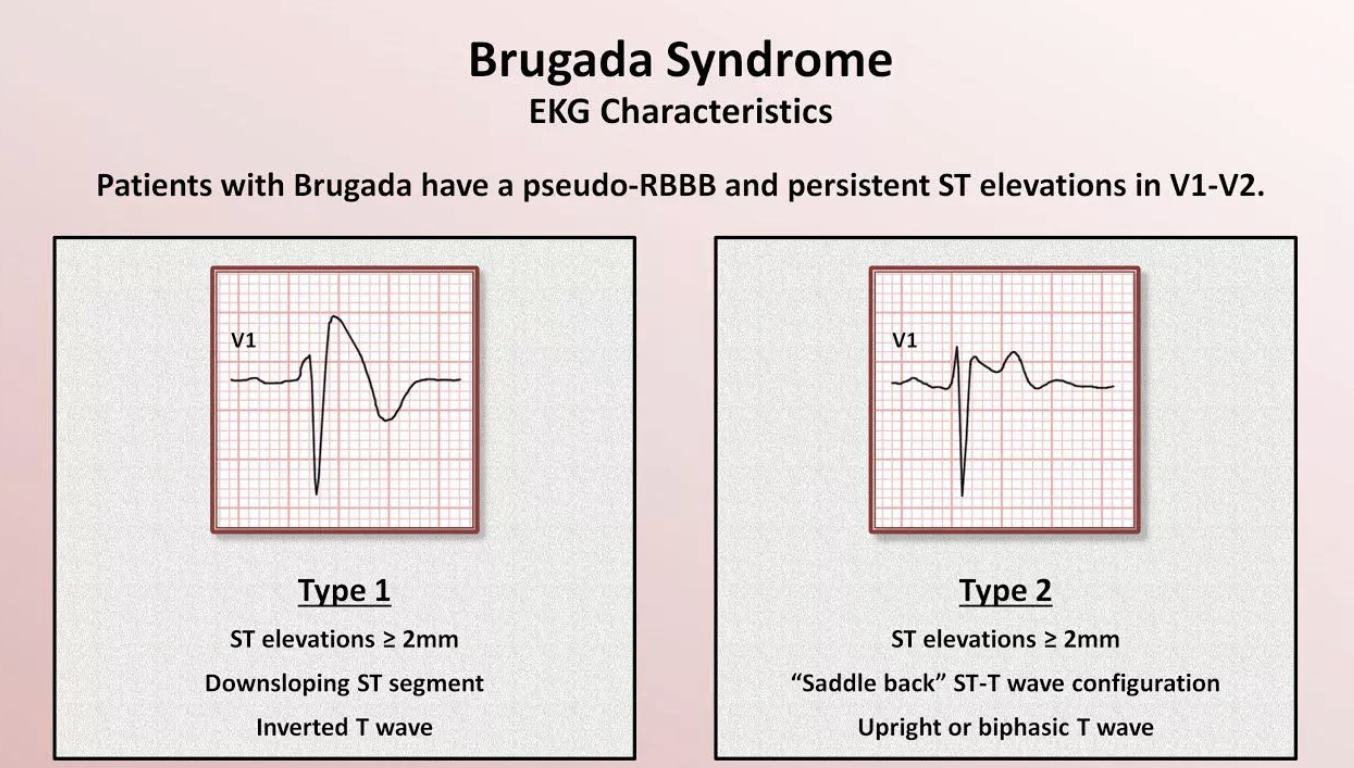
causes of Brugada Syndrome and precipitating agents
autosomal dominant inheritance or sodium channelopathy → loss of function of Na+ channels
sedation (propofol, ketamine)
Na channel blockers (procainamide, flecainide)
Antipsychotics or depressants (SSRI’s, TCA’s, Lithium)
nocturnal agonal respirations and no chest pain
Brugada Syndrome
ECG finding in Brugada Syndrome
Saddleback or Covered ST Segment Elevation in V1-V3
also has J point elevation
tx for Brugada Syndrome
electrical cardioversion to fix tachydysrhythmias
cardio consult for ICD
ECG of Lown-Ganong-Levine Syndrome
Narrow PR interval < 3 small boxes
Narrow QRS < 1.5 small boxes
tachycardia

ECG finding in WPW Syndrome
Delta waves = slurred, slow upstroke in the initial part of the QRS complex
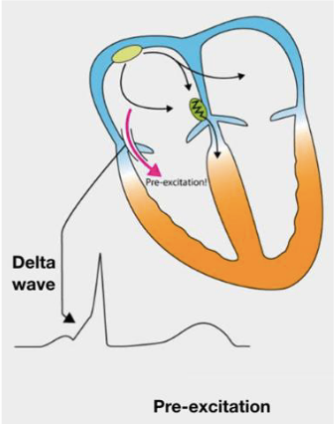
when is WPW presentation most common
children
congenital pre-excitation syndrome
tx AVRT
stable pt → Procainamide IV
CI: prolonged QT
unstable pt → Synchronized Cardioversion
Avoid all AV node blocking agents (Digoxin, BB, CCB)