5. Angle Closure Glaucoma and Gonioscopy
1/117
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
118 Terms
How can mechanical obstruction of the anterior chamber angle lead to glaucoma?
Mechanical blockage of the iridocorneal angle impedes aqueous humor outflow → ↑ IOP → damage to the optic nerve head (glaucomatous optic neuropathy).
What is the purpose of the van Herick technique?
A slit-lamp screening method that estimates anterior chamber angle depth by comparing peripheral anterior chamber depth to corneal thickness. It helps identify eyes at risk for angle closure.
How are van Herick grades interpreted?
Grade 4: Chamber depth > ½ corneal thickness (wide open angle)
Grade 3: ¼–½ corneal thickness
Grade 2: ≈ ¼ corneal thickness (moderately narrow)
Grade 1: < ¼ corneal thickness (very narrow; high angle-closure risk)
What is a key limitation of the van Herick technique?
It estimates chamber depth only; it does not directly evaluate angle structures or the integrity of the aqueous outflow system. Gonioscopy is required for definitive assessment of the angle anatomy.
What is primary angle closure, and what are the two types of angle closure?
Primary angle closure is appositional or synechial closure of the anterior chamber angle, obstructing aqueous outflow.
Appositional closure: Temporary contact between the peripheral iris and angle structures.
Synechial closure: Permanent closure due to peripheral anterior synechiae (PAS).
How does primary angle closure cause elevated IOP?
Closure of the anterior chamber angle blocks access of aqueous humor to the trabecular meshwork → decreased outflow → increased IOP → risk of glaucomatous optic nerve damage.
What is the definitive method for determining whether appositional or synechial angle closure is present?
Gonioscopy. It is the gold standard for directly visualizing the anterior chamber angle and identifying angle closure, PAS, and angle anatomy.
Why is gonioscopy necessary even when screening tests (e.g., van Herick) suggest a narrow angle?
Screening tests estimate angle width but cannot directly evaluate angle structures or confirm appositional vs. synechial closure. Only gonioscopy can definitively assess these disease processes.
What are the main purposes of gonioscopy in glaucoma evaluation?
Gonioscopy is used to:
Determine how much of the drainage angle is open
Assess angle configuration and iris approach
Evaluate trabecular meshwork pigmentation
Differentiate open-angle, angle-closure, and plateau iris mechanisms
Identify signs of secondary glaucomas (e.g., pigmentary, pseudoexfoliative, uveitic, neovascular, traumatic)
Why is gonioscopy considered the gold standard for angle assessment?
Gonioscopy directly visualizes the anterior chamber angle structures, allowing accurate assessment of angle anatomy, closure mechanisms, pigmentation, and secondary glaucomatous changes that cannot be reliably determined by screening techniques alone.
How does gonioscopy allow visualization of the anterior chamber angle?
Gonioscopy uses a specialized contact lens to eliminate total internal reflection at the cornea, permitting direct visualization of otherwise hidden angle structures.
Which secondary glaucomas can be identified or characterized with gonioscopy?
Gonioscopy can reveal findings suggestive of:
Pigmentary glaucoma (PDS)
Pseudoexfoliation glaucoma (PXE)
Uveitic glaucoma
Neovascular glaucoma
Traumatic glaucoma
What are the advantages and disadvantages of a 4-mirror gonio lens without a flange?
Advantages:
Faster to use
No coupling solution required
Can perform indentation gonioscopy
Commonly used clinically
Disadvantages:
Requires more skill/finesse to obtain optimal views
What are the advantages and disadvantages of a 4-mirror gonio lens with a flange?
Advantages:
More stable on the eye
Provides high-quality views
Commonly used for examinations and some surgical applications
Disadvantages:
Requires coupling solution and more preparation
Cannot perform indentation gonioscopy
Which type of gonioscopy lens allows indentation, and why is this clinically useful?
The flangeless 4-mirror lens allows indentation gonioscopy, which helps distinguish:
Appositional angle closure (angle opens with indentation)
Synechial angle closure (angle remains closed despite indentation)
Why should gonioscopy be performed under dim illumination?
Excess room light or slit-lamp illumination causes pupillary constriction, which pulls the peripheral iris away from the angle and can make the angle appear artificially more open. Dim lighting provides a more accurate assessment of angle-closure risk.
How can lighting conditions affect the appearance of a narrow angle during gonioscopy?
Bright light: Miosis → peripheral iris pulled away from angle → angle appears wider.
Dark conditions: Physiologic dilation → peripheral iris crowds the angle → angle may appear narrower, revealing true angle-closure risk.
What techniques can help identify angle structures when gonioscopic findings are difficult to interpret?
Corneal wedge technique: Helps identify Schwalbe's line (SL) and orient angle anatomy.
Indentation gonioscopy: Helps distinguish various angle structures and mechanisms of angle closure.
What is the principle behind indentation gonioscopy?
Pressure from the gonioscopy lens displaces aqueous posteriorly and mechanically opens appositionally closed angles. It is useful for distinguishing:
Appositional closure → opens with indentation
Synechial closure (PAS) → remains closed despite indentation
What gonioscopic finding may occur during indentation when episcleral venous pressure exceeds IOP?
Blood may reflux into Schlemm's canal, producing a characteristic red hue that can help identify the canal.
What components should be documented when recording gonioscopy findings?
Record:
Most posterior visible structure in each quadrant (CB, SS, TM, SL, or NS)
Pigmentation grade (1+ to 4+)
Iris approach (flat, convex, or concave)
Additional findings (PAS, nodules, cysts, iris processes, recession, etc.)
What is the order of angle structures from anterior to posterior? (High yield)
NS → SL → TM → SS → CB
Mnemonic: "No Student Takes Summer Classes"
NS = No structure
SL = Schwalbe's line
TM = Trabecular meshwork
SS = Scleral spur
CB = Ciliary body
How are gonioscopy findings recorded anatomically?
Findings are documented according to the true anatomical quadrant (superior, inferior, nasal, temporal), not the mirror image seen through the gonioscopy lens.
In gonioscopy notation, what does a more posterior visible structure indicate?
A more posterior visible structure (e.g., CB > SS > TM > SL) indicates a wider, more open angle, whereas seeing only anterior structures suggests a narrower angle.
What is a Sampaolesi line, and what conditions is it associated with?
A heavily pigmented line anterior to Schwalbe's line seen on gonioscopy. It is classically associated with:
Pigment dispersion syndrome (PDS)/pigmentary glaucoma
Pseudoexfoliation syndrome (PXE)/pseudoexfoliative glaucoma
What are peripheral anterior synechiae (PAS), and how do they affect aqueous outflow?
PAS are adhesions of the peripheral iris to angle structures. They create a tent-like anterior displacement of the iris, can cover the trabecular meshwork (TM), and obstruct aqueous humor outflow, leading to elevated IOP.
What are common causes of peripheral anterior synechiae (PAS)?
PAS may result from:
Chronic angle closure
Inflammation (uveitis)
Neovascular membranes
ICE (iridocorneal endothelial) syndrome
Ocular trauma
How can PAS be distinguished from appositional angle closure during gonioscopy?
PAS are permanent adhesions and do not open with indentation gonioscopy, whereas appositional closure typically opens when the angle is indented.
What are iris processes, and why are they important to recognize?
Iris processes are normal, thin, vertical projections of iris tissue extending toward angle structures. They:
Do not obstruct aqueous outflow
Do not alter iris position
Should not be mistaken for PAS
What gonioscopic findings suggest neovascularization of the angle (NVA)?
Abnormal blood vessels growing within the angle, particularly vessels crossing the scleral spur onto the trabecular meshwork, are suspicious for neovascularization and are usually abnormal.
How can normal iris vessels be distinguished from angle neovascularization?
Normal iris vessels: Run circumferentially around the angle.
Neovascular vessels: Tend to run vertically within the angle and may cross the scleral spur onto the trabecular meshwork.
Why is neovascularization of the angle clinically important?
Neovascular membranes can contract, leading to secondary angle closure, impaired aqueous outflow, and development of neovascular glaucoma, a potentially severe form of secondary glaucoma.
What traumatic injuries of the anterior chamber angle can be identified with gonioscopy?
Major traumatic angle injuries include:
Angle recession = tear between longitudinal and circular ciliary body muscles
Cyclodialysis = separation of ciliary body from the scleral spur
Iridodialysis = tear/disinsertion of the iris root
Trabecular meshwork damage
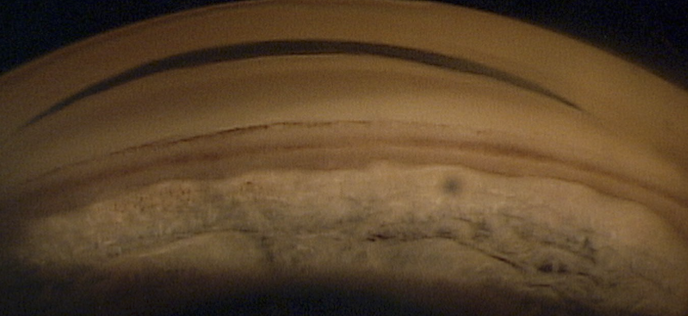
What is angle recession, and how does it affect aqueous outflow?
Angle recession is a tear between the longitudinal and circular fibers of the ciliary body following blunt trauma. Microtears alter normal aqueous drainage pathways and can result in decreased aqueous outflow and subsequent glaucoma.
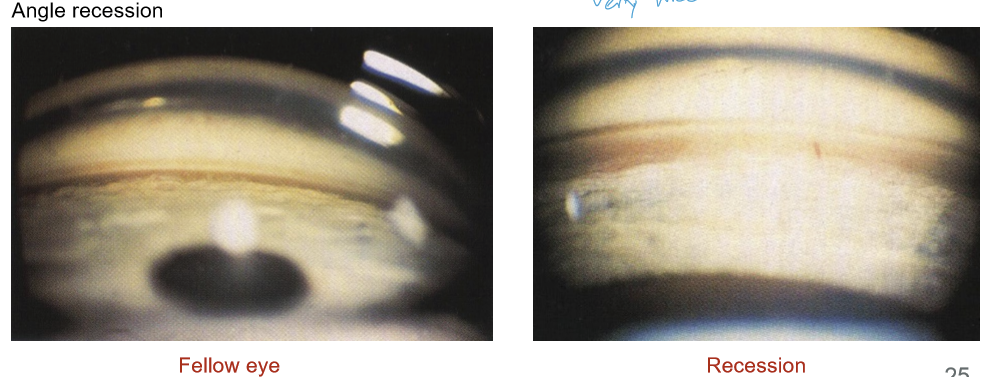
What is the most common gonioscopic sign of post-contusional (blunt trauma) eye injury?
Angle recession.
What is the hallmark gonioscopic appearance of angle recession?
Widening of the ciliary body (CB) band. The recession may be:
Sectoral (localized), or
360° (circumferential)
What is the glaucoma risk associated with angle recession?
Approximately 9% of patients with angle recession develop glaucoma. Importantly, IOP elevation may occur many years after the initial injury, so long-term monitoring is required.
How do cyclodialysis and iridodialysis differ?
Cyclodialysis: Separation of the ciliary body from the scleral spur.
Iridodialysis: Separation/tear of the iris root from its attachment.
Does all angle obstruction result in glaucomatous optic nerve damage?
No. Angle obstruction alone does not equal glaucoma. Optic nerve damage and/or visual field loss must be present for the diagnosis of primary angle-closure glaucoma (PACG).
How do most cases of primary angle-closure disease present?
Most are chronic and incomplete, with angle obstruction that is sectoral and/or intermittent. Symptoms are usually absent unless an acute attack occurs.
What are the stages of primary angle-closure disease?
Primary angle-closure suspect (PACS)
Primary angle closure (PAC)
Primary angle-closure glaucoma (PACG)
Acute angle closure
Plateau iris configuration
What are the diagnostic criteria for Primary Angle-Closure Suspect (PACS)?
All of the following:
>180° iridotrabecular contact (ITC)
Normal IOP
No PAS
No optic nerve damage
No visual field loss
What is iridotrabecular contact (ITC)?
Contact between the peripheral iris and trabecular meshwork (TM). Clinically, if you cannot see the TM, assume the iris is apposed against it (ITC).
What symptoms do PACS patients have, and what is their natural history?
Patients are typically asymptomatic. About 25% progress to elevated IOP or PAS over time.
What distinguishes Primary Angle Closure (PAC) from PACS?
PAC has:
>180° ITC
PAS and/or elevated IOP present
No optic nerve damage
No visual field loss
Why is PAC not yet considered glaucoma?
Although angle closure has caused PAS and/or elevated IOP, there is no glaucomatous optic neuropathy or visual field loss.
How can PAC present clinically?
It may present as:
Chronic intermittent angle closure (most common)
An acute angle-closure attack
When might a patient with PAC become symptomatic?
During episodes of IOP elevation, especially when the pupil dilates (e.g., pharmacologic mydriasis), causing increased angle crowding.
What distinguishes Primary Angle-Closure Glaucoma (PACG) from Primary Angle Closure (PAC)?
PACG has:
>180° iridotrabecular contact (ITC)
PAS and/or elevated IOP
Glaucomatous optic nerve damage
Visual field loss
What symptoms do patients with PACG typically have?
Chronic PACG is usually asymptomatic, while acute angle closure produces symptomatic attacks.
What are the major risk factors for primary angle-closure glaucoma?
Think "Old Hyperopic Asian Female":
Asian ancestry
Age >50 years
Female sex
Hyperopia
Short axial length
Anteriorly positioned crystalline lens
Why is PACG an important cause of visual impairment worldwide?
Although PACG accounts for only about 25% of glaucoma cases worldwide, it causes at least 50% of glaucoma-related blindness, making it disproportionately vision-threatening.
What is the most common mechanism of primary angle closure?
Pupillary block, which accounts for the vast majority of primary angle-closure disease (≈90% in Caucasian patients).
Describe the pathophysiology of pupillary-block angle closure.
Iridolenticular apposition impedes aqueous movement from the posterior to anterior chamber.
Pressure builds behind the iris.
The iris bows forward (iris bombe).
The peripheral iris obstructs the trabecular meshwork.
Aqueous outflow decreases → IOP rises.
What is iris bombe?
Forward bowing (convex configuration) of the iris caused by pressure buildup in the posterior chamber during pupillary block.
Differentiate relative versus absolute pupillary block.
Relative pupillary block: Partial/intermittent obstruction; often chronic and episodic.
Absolute pupillary block: Complete 360° obstruction leading to acute angle closure.
What gonioscopic appearance is characteristic of pupillary-block angle closure?
A convex iris configuration (iris bombe) with iridotrabecular contact (ITC), where the peripheral iris obstructs the trabecular meshwork and reduces aqueous outflow.
When evaluating a narrow angle with pigmentation, why might indentation gonioscopy or the corneal wedge technique be necessary?
They help determine whether the visible pigmented band is:
Trabecular meshwork (TM) that is partially obscured by the iris, or
Ciliary body (CB) with little TM pigmentation visible.
What is the effect of indentation gonioscopy in pupillary-block angle closure?
Indentation pushes aqueous posteriorly, flattening the bowed iris and opening an angle that is closed due to appositional pupillary block.
How does indentation gonioscopy help distinguish pupillary block from synechial closure?
Pupillary block/appositional closure: Angle opens and iris flattens with indentation.
PAS (synechial closure): Angle remains closed because adhesions are permanent.
What is the definitive treatment for pupillary-block angle closure?
Laser Peripheral Iridotomy (LPI).
How does a Laser Peripheral Iridotomy (LPI) work?
LPI creates a small opening in the peripheral iris that:
Provides an alternative route for aqueous flow from the posterior to anterior chamber.
Equalizes pressure between the posterior and anterior chambers.
Eliminates relative pupillary block.
Flattens the iris.
Allows the peripheral iris to fall backward and the angle to open.
What is the mechanism by which LPI reverses iris bombe?
By bypassing the pupillary block, LPI relieves the pressure gradient behind the iris, causing the iris to flatten and reducing iridotrabecular contact.
What anatomic change is seen after successful laser peripheral iridotomy (LPI)?
The iris bombe resolves, the iris flattens, and the anterior chamber angle widens/opening occurs as the pressure gradient across the iris is eliminated.
Which lasers are commonly used to perform an LPI?
Nd:YAG laser (most commonly tested)
Argon laser
Diode laser
Where should an LPI ideally be placed, and why?
A lateral/superior peripheral iris location is preferred because it may reduce stray light symptoms caused by light reflecting through the iridotomy, which acts like an artificial pupil.
What is dysphotopsia after LPI?
Visual symptoms such as glare, lines, streaks, ghost images, or light reflections caused by light passing through or around the iridotomy.
What are the potential complications or side effects of laser peripheral iridotomy (LPI)?
Dysphotopsia
Transient IOP spike
Uveitis
Cataract formation
Retinal detachment (rare)
Recurrent herpetic keratitis
What are the indications for Laser Peripheral Iridotomy (LPI) in pupillary-block angle closure?
LPI may be indicated for:
Primary angle-closure glaucoma (PACG)
Acute attacks (treat fellow eye as well)
Chronic disease
Primary angle closure (PAC)
Primary angle-closure suspect (PACS) to reduce risk of progression
Why is the fellow eye treated after an acute angle-closure attack?
The fellow eye often has similar anatomic risk factors and is at high risk for developing angle closure, so prophylactic LPI is typically performed.
What are the contraindications or situations where LPI may not be appropriate?
Significant corneal edema (need a clear view of the peripheral iris)
Very flat anterior chamber
Angle closure caused by a mechanism other than pupillary block
What did the Zhongshan Angle Closure Prevention (ZAP) Study show?
LPI:
Widens the angle
Reduces the risk of PACS progressing to PAC
However:
The overall risk of progression from PACS → PAC is relatively low
Therefore, not all PACS patients necessarily require prophylactic LPI
How does cataract surgery affect angle closure?
Removal of the crystalline lens and implantation of an IOL:
Deepens the anterior chamber
Moves the iris-lens diaphragm posteriorly
Widens the angle
Can reduce or eliminate pupillary-block anatomy
When should cataract surgery be considered in PACS or PAC patients?
In non-acute PACS or PAC patients, assess whether cataract extraction (CE/PCIOL) may be beneficial because it can open the angle and potentially avoid the need for LPI.
What did the EAGLE trial demonstrate regarding treatment of primary angle closure and PACG?
In selected patients with PAC or PACG and elevated IOP, clear lens extraction (CLE):
Lowered IOP more than LPI
Produced better quality-of-life outcomes
May be more cost-effective long term
How do clear lens extraction (CLE) and LPI differ in treating angle closure?
LPI: Eliminates pupillary block by creating an alternate aqueous pathway.
CLE: Removes the lens, deepens the anterior chamber, widens the angle, and may reduce IOP more effectively in some PAC/PACG patients.
What is the mechanism of plateau iris angle closure?
An anteriorly positioned or enlarged ciliary body pushes the peripheral iris forward, keeping the iris root close to the trabecular meshwork despite a relatively normal central anterior chamber depth.
What are the characteristic findings of plateau iris?
Normal/deep central anterior chamber
Flat iris plane centrally
Narrow or occludable angle
Peripheral iris turns sharply posterior before inserting into the ciliary body
How can plateau iris be distinguished from pupillary block?
After a successful LPI, the angle remains appositionally closed or occludable because the underlying problem is the ciliary body configuration, not pupillary block.
What is the classic indentation gonioscopy finding in plateau iris?
"Rolling" or "double-hump" movement of the peripheral iris during indentation.
When should plateau iris be suspected?
When a patient has:
A patent LPI
Persistent narrow angles
Continued angle closure despite elimination of pupillary block
What is the treatment of choice for plateau iris configuration?
Argon Laser Peripheral Iridoplasty (ALPI), also called gonioplasty.
How does ALPI work?
Low-energy argon laser burns are placed in the extreme peripheral iris, causing stromal contraction that pulls the peripheral iris away from the trabecular meshwork and opens the angle.
What are the indications for ALPI?
Plateau iris configuration
Persistent/chronic angle closure despite LPI
Acute angle-closure attack (can often be performed through a hazy cornea)
What is a contraindication to ALPI?
Peripheral anterior synechiae (PAS), because synechial closure is permanent and cannot be opened by pulling the iris away.
What is the effect of Argon Laser Peripheral Iridoplasty (ALPI) on plateau iris?
ALPI contracts the peripheral iris stroma, pulling the peripheral iris away from the trabecular meshwork and opening the angle despite persistence of the underlying ciliary body anatomy.
What is aqueous misdirection (malignant glaucoma)?
A rare cause of secondary angle closure in which aqueous humor is misdirected posteriorly into or behind the vitreous, increasing vitreous volume and pushing the entire lens–iris diaphragm forward.

What is a classic setting in which aqueous misdirection occurs?
A rare complication following penetrating glaucoma surgery, especially trabeculectomy.
What are the hallmark clinical findings of aqueous misdirection?
High IOP
Uniformly shallow or flat anterior chamber
Forward displacement of the entire lens–iris diaphragm
How can aqueous misdirection be differentiated from postoperative hypotony?
Both may produce a flat anterior chamber, but:
Hypotony: IOP < 6 mmHg
Aqueous misdirection: IOP elevated (>21 mmHg)
What is choroidal effusion as a mechanism of angle closure?
A rare secondary angle-closure mechanism in which swelling of the choroid and ciliary body causes anterior displacement of the lens–iris diaphragm, resulting in shallowing of the anterior chamber and angle closure.
What are common causes of choroidal effusion-induced angle closure?
Ocular surgery
Medications, especially topiramate (Topamax)
Other drug-induced ciliochoroidal effusions
How does choroidal effusion cause angle closure?
Choroidal/ciliary body swelling → anterior displacement of ciliary body and lens–iris diaphragm → narrowed angle + shallow anterior chamber → elevated IOP.
What refractive change is classically associated with choroidal effusion?
A dramatic acute myopic shift due to forward displacement/thickening of the crystalline lens.
How does topiramate-induced angle closure differ from pupillary-block angle closure?
Topiramate/choroidal effusion: Ciliary body swelling pushes the lens–iris diaphragm forward.
Pupillary block: Pressure differential causes iris bombe.
What medication is most classically associated with drug-induced choroidal effusion and angle closure?
Topiramate (Topamax).
How is choroidal effusion or aqueous misdirection medically treated?
Cycloplegics (e.g., atropine)
Aqueous suppressants
Address the underlying cause (especially medications)
Why are cycloplegics used for choroidal effusion and aqueous misdirection?
Cycloplegics relax the ciliary body and help move the lens–iris diaphragm posteriorly, reducing angle crowding and deepening the anterior chamber.
Which miotic should be avoided in aqueous misdirection and choroidal effusion?
Pilocarpine.
What surgical treatment may be required for aqueous misdirection?
Vitrectomy with disruption/puncture of the anterior hyaloid face to restore normal aqueous flow.