CXR Image Appraisal Quiz 2024
1/9
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
10 Terms
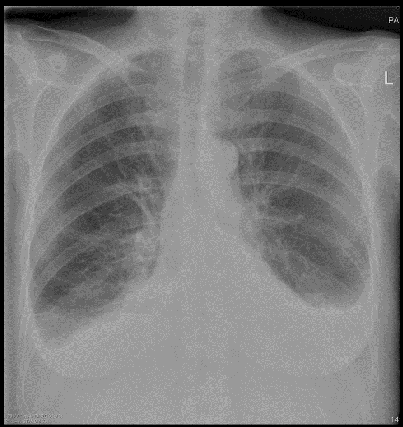
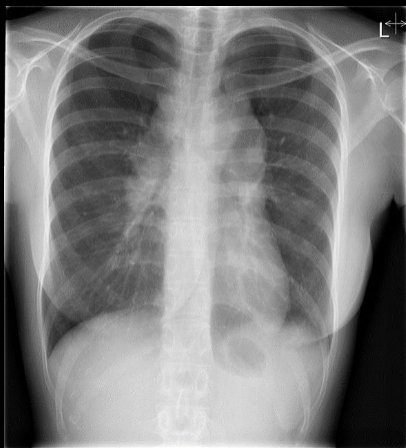
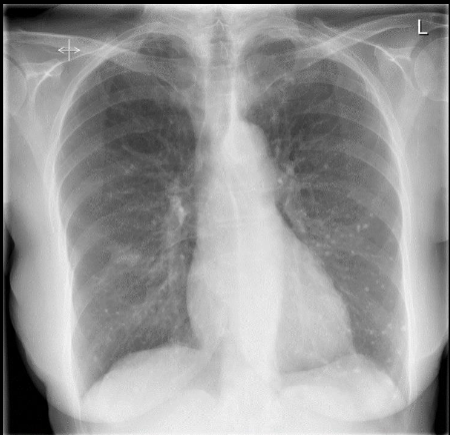
Female. 85 years. Previously well. Now attends her General Practitioner c/o increasing shortness of breath.
Temperature normal
Postero-anterior Chest X-ray
Abnormal
Bilateral costophrenic blunting, synonymous with bilateral
pleural effusions.
The patient has taken a good inspiration but there is volume loss in both lungs, although lung markings
appear normal.
Difficult to assess cardiothoracic ratio due to
effusions.
There appears to be splaying of the carina and this may relate to some cardiac (left ventricular failure) enlargement.
Note to students there are many causes of bilateral effusions, not all are evident on CXR. However, given the history (previously well, but now breathless) the likely cause is probably left ventricular failure (LVF). NB most patients who have CXR evidence of LVF invariably have evidence of cardiac enlargement on a standard PA CXR. One exception to this "rule" is the patient with a normal size heart who develops an acute myocardial infarction and then goes into LVF.
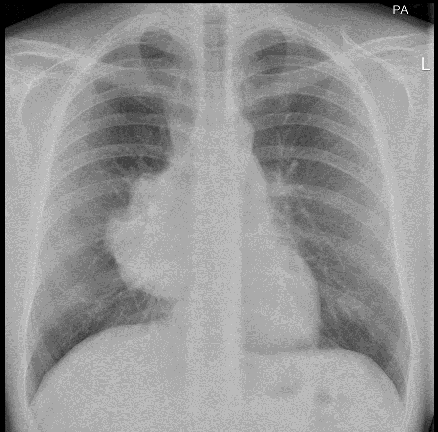
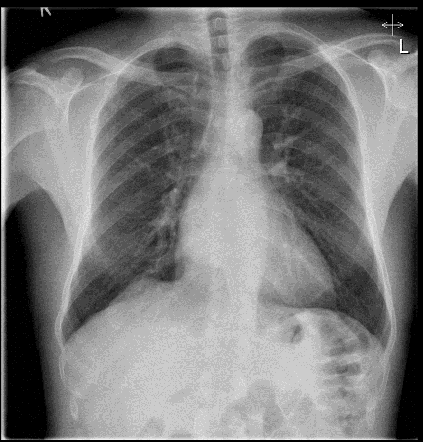
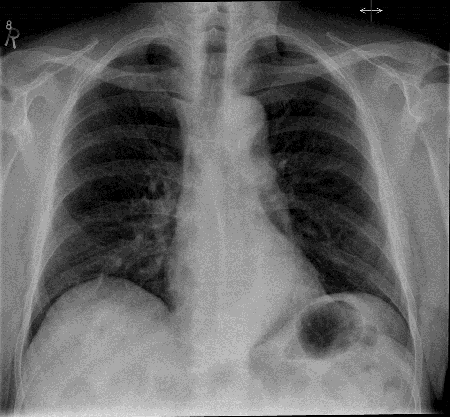
Male. 22 years. Loss of weight and generalised weakness
Postero-anterior Chest X-ray
Abnormal
There is a large, irregular, mass obscuring the right cardiac
border – leading to a widened mediastinum.
The left cardiac border and both diaphragmatic contours can be seen.
There has been a good inspiratory effort, and visible lung
markings are normal, as are the remaining bone and soft
tissue appearances and there is no volume loss in the left
lung.
Obliteration of the rt cardiac border suggests an anterior
mediastinal mass.
Notes for students: If this is an anterior mediastinal mass then the most likely causes are the Terrible T’s Thymoma, Teratoma, Thyroid Carcinoma OR Terrible lymphoma.
Subsequent histology: lymphoma
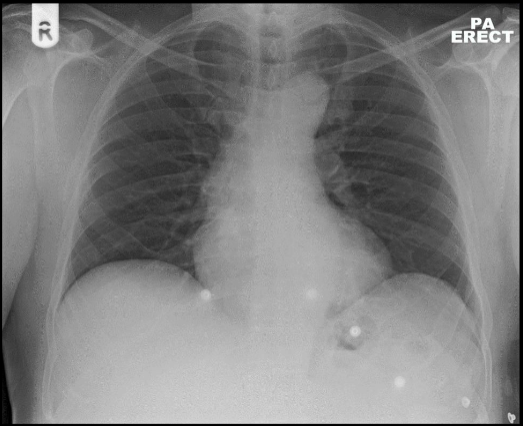
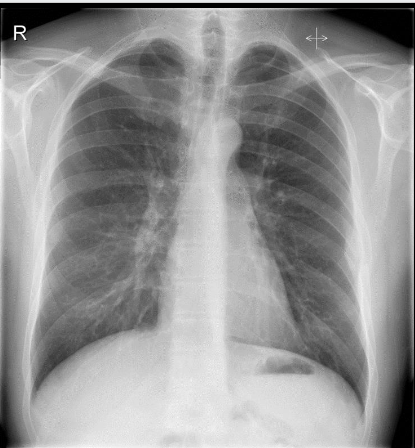
Female. 65 years. Acute left sided chest pain. ?MI
Posteroanterior chest X-ray
Abnormal
There is a widened mediastinum, both diaphragms appear raised although the lung markings are unremarkable.
The mediastinal widening appears to be due to an unfolded aorta (age related) which has resulted in a prominent aortic arch.
Heart size is within normal limits.
The costophrenic angles are normal, as is the mediastinum, hila, lungs, bones - all normal.
Notes for students: The cause of the chest pain is not shown, it could be the aorta, or something else. The CXR appearances are within normal limits for age; age-related aortic unfurling is a phenomenon of old age – strictly this would be classed as a “Normal or Age Related Variant”
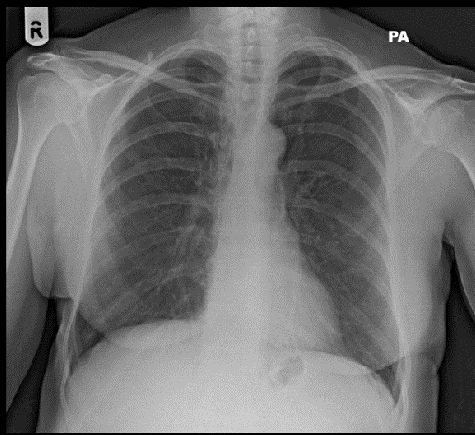
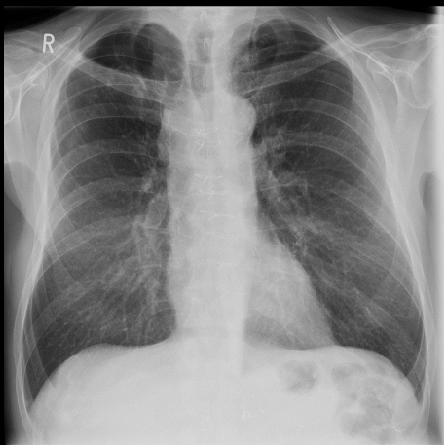
Female. 64 Years. Non-smoker. Persistent cough
for one month. Otherwise well
Postero-anterior chest X-ray.
Normal
Both lungs are of normal volume with unremarkable lung markings.
No evidence of shadowing in either lung.
And the trachea is central.
The Cardiothoracic ratio is within normal limits.
Both hila are symmetrical in appearances, and the diaphragmatic contours are normal, no soft tissue or bony abnormality seen.
Note for students: You may have observed a lucent / black area around the left side of the aortic arch and left cardiac border - These appearances are normal - but might have caused you to consider mediastinal emphysema. In that respect, there is no evidence of air elsewhere in the mediastinum nor in the soft tissues.
Sometimes, a normal CXR may show an increase in "blackening" along the left side of the heart, yet the explanation is not obvious. Occasionally the explanation is a prominent vessel paralleling the left border of the heart or due to an optical illusion based on a Mach band or the Mach effect.
Female, 30 years. Erythema nodosum and arthralgia. No other symptoms
Postero-anterior chest X-ray
Abnormal
Both lungs are on the upper limits of normal lung volume, and the lung markings are normal.
There is, however, asymmetry of the hilar regions, with bilateral hilar enlargement, and increased hilar density seen.
There also appears to be right paratracheal lymph node enlargement contributing to mediastinal widening.
The heart is not enlarged and there is no costophrenic blunting.
No other soft tissue or bony abnormality seen.
Notes for students: The appearance may be due to several causes including malignancy, Tuberculosis or sarcoid – but the clinical history, age and nodal enlargement suggests Sarcoid as a probable cause.
Male. 42 years. Persistent cough. Otherwise well
Posteroanterior CXR
Abnormal
Normal lung volume and lung markings. No cardiac enlargement.
However, there is a focal increase in density, behind the right cardiac outline.
This is probably a retro-cardiac mass.
There is also juxtaphrenic peaking of the right hemidiaphragm,
otherwise the rest of the CXR is normal with no other soft tissue or bony abnormalities.
Notes for students: Remember the rule . . . " the density of the shadowing on the right side of the heart should be: (a) even/uniform, and (b) the same as the density of the shadow of the left side of the heart. On this patient's CXR this rule [ie both (a) and (b)] is clearly broken. Follow up ascertained: this mass was a bronchogenic cyst.
Bronchogenic cysts are congenital, mediastinal abnormalities arising from the bronchial tree. They can cause mediastinal widening, compression and airway obstruction.
Male. 32 years. Complains of severe left sided chest pain.
Postero-anterior chest X-ray
Abnormal.
Good inspiratory effort, both lungs are of normal volume, and the lung markings are unremarkable.
There is a soft tissue shadow seen in the left middle zone, arising from the chest wall, and is visible in relation to the lateral aspect of the left 7th rib.
There may also be some associated rib destruction.
Otherwise, heart size is normal, and no other soft tissue or bony abnormality seen
Notes for students: The soft tissue shadow is visible on CXR, and the appearances are concerning and require further investigation. This patient underwent CT, and rib destruction was confirmed. (Eventual diagnosis: was Histiocytosis, a rare condition affecting the histiocytes found in the blood. There is still some debate whether Langerhan’s Histiocytosis is a type of cancer or not)!
Male 60 years. Recent onset of shortness of breath and wheezing
Posteroanterior chest X-ray
Abnormal
There are sternotomy wires present from a previous median-sternotomy / Coronary Artery Bypass Graft.
There are also some old TB scars at the apex of the right lung.
Otherwise, a good inspiratory effort with normal lung markings evident.
Heart size is within normal limits, but there is moderate superior mediastinal widening present with co-existing tracheal narrowing.
This may be suggestive of a mass exerting extrinsic pressure on the trachea.
Female. 70 years. Persistent and troublesome cough
Posteroanterior chest X-ray
Abnormal
Good inspiratory effort with no volume loss.
However, there is a conspicuous, well-defined shadow in the right middle zone.
There are also diffuse small calcifications apparent within both lungs – but mainly in the left lung, and normal cardiac contours and size.
Both hila are symmetrical in size, shape and density and no effusions can be seen.
Also, note that an azygo-oesophageal line is seen over the anterior surfaces of the thoracic vertebrae.
No other soft tissue or bony abnormality seen.
Notes for students: The radiologist also noted some shadowing to the left side of the trachea and manubrium. . . BUT this was not considered to be of any significance on this slightly rotated CXR. The RMZ lesion warranted further investigation with CT section. Lung calcifications also seen on CT and a confirmed history of chickenpox in her 30’s, is the cause of the abnormal calcification appearances.
Male. 75 years. Cough and a slight fever – over the last
week.
Posteroanterior Chest X-ray
Abnormal
There is a subtle area of increased density / shadowing evident in the right lung base located below the dome of the right hemidiaphragm.
The mediastinum appears widened, with increasing density seen behind the left cardiac shadow, this is probably due to aortic unfurling and is therefore unimportant.
There is also a prominent azygo-oesophageal line, but this is of no consequence.
The lungs are well inflated, and normal markings are depicted; heart size is within normal limits.
Notes for students: the posterior portions of the lungs extend well below the anterior aspect of the hemidiaphragms, so it is important that you always check BELOW BOTH diaphragms – “if you do not look, you will not see!”