Local Function of the Spinal Cord: Segmental Spinal Reflexes (Week 1, Mod 8)
1/20
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
21 Terms
TERMINOLOGY TIME
What is an alpha efferent neuron?
An efferent neuron with its cell body in the VENTRAL gray horn of the spinal cord
Innervates the extrafusal muscle fibers
What is a gamma efferent neuron?
Is an efferent neuron with its cell body in the ventral gray horn of the spinal cord
innervates the polar region of the intrafusal muscle fibers
What is a lower motor neuron (LMN)?
Neuron associated with motor function; cell body is WITHIN the CNS, while the axon LEAVES the CNS
Considered to be peripheral motor neurons
What is an upper motor neuron (UMN)?
Neurons confined WITHIN the CNS that are associated with motor function
Are what communicate between the brain and LMN to get muscles to move
Involved in the INITIATION and CONTROL of the LMNs… INHIBITS THEM from overreacting to stimuli
What is a reflex arc?
Involves both the PNS and the CNS:
Sensory / afferent nerve brings info into the CNS where the input is linked DIRECTLY to a motor / efferent nerve
“Hard wired” into the nervous system; is what controls many of our involuntary functions
(Ex: pupil contracting in response to bright light)
What is a response / reaction, and how is it different from a reflex arc?
Is CORTICALLY MEDIATED
Sensory / afferent info is integrated and interpreted into the cerebral cortex
A motor / efferent response is initiated as a consequence
Again, what are the segments of the spine?
Cervical spine: C1-C5
Thoracic spine: C6-T2
Lumbar spine: T3-L3
Sacral spine: L4-S3
Can be differentiated into L4-S1 and S1-S3 for clinical reasons
What is an example of a spinal reflex?
Patellar reflex (aka muscle spindle and stretch reflex)
How exactly does the patellar reflex come about upon stimulation? List what happens in the AFFERENT pathway…
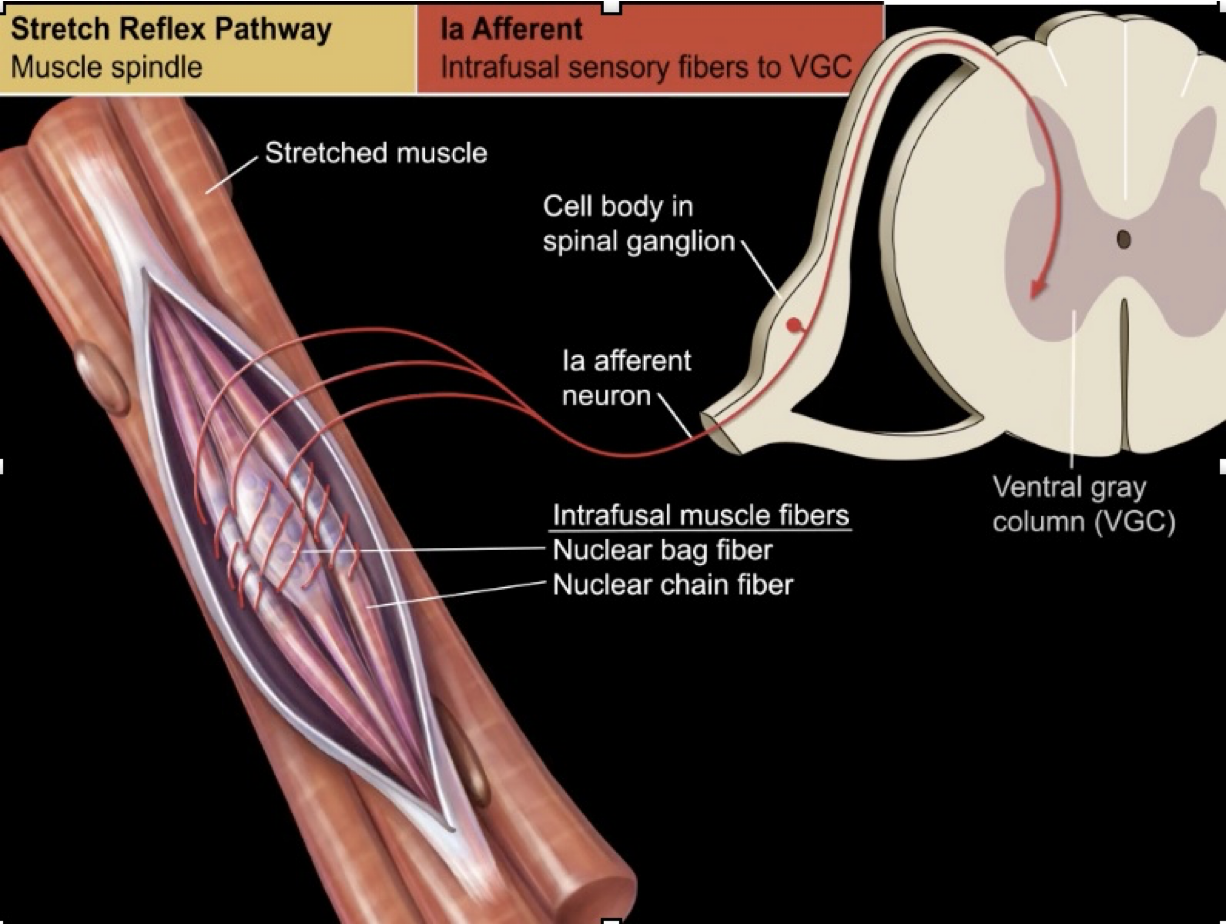
Afferent Pathway:
Muscle is stretched by contact with the hammer
Stretch receptors in the muscle fiber are stimulated
These are intrafusal sensory fibers… wrap around the nuclear bag fiber of the intrafusal muscle of the patellar tendon (see image)
These afferent nerves then send the signal up to the DORSAL horn of the gray matter of the spinal cord
Remember: neuronal cell body OUTSIDE of CNS, found in the spinal ganglion
How exactly does the patellar reflex come about upon stimulation? List what happens in the EFFERENT pathway…
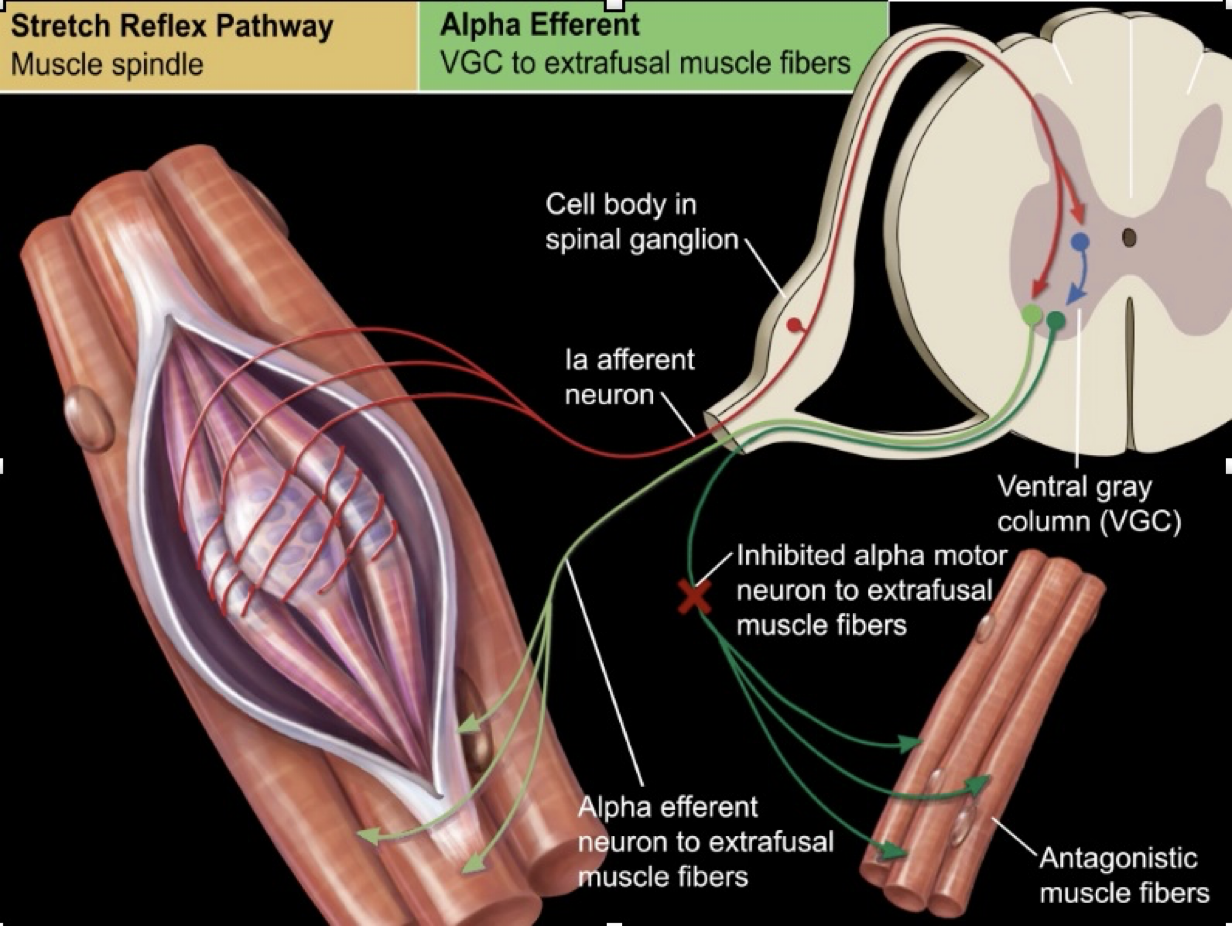
Efferent Pathway:
Efferent nerve cell body lies WITHIN the gray matter of the VENTRAL horn, communicates directly with the afferent nerve in here
NO INTERNEURON
Signal of alpha efferent neuron is sent to the EXTRAFUSAL muscle fibers of the tendon, triggering a contraction
At the same time, has to INHIBIT ANTAGONISTIC MUSCLE FIBERS, so a different alpha motor neuron that has received the same signal from the afferent neuron is stimulated
Sends a signal to inhibit the contraction of antagonistic flexor muscles, allowing for the involuntary extension of the patella
What are the 3 functional tests you can perform to assess for damage in the lumbosacral plexus?
1) Flexor (withdrawal) reflex
Evaluates the sciatic + femoral nerve and L4-S1 spinal cord segments
Pinch paws for this
Looking for flexion of ALL the joints
Sciatic nerve = flexion of stifle and tarsus
Femoral nerve = flexion of the hip
DOES HAVE AN INTERNEURON = MULTISYNAPTIC REFLEX
2) Patellar reflex
Evaluates the femoral nerves + L4 - L6 spinal cord segments
Monosynaptic reflex (1 synapse, no interneuron)
3) Perineal reflex
Evaluates the pudendal nerve, caudal nerves, and S1-Cd5 spinal cord segments
Pinch the anus; sphincter should contract, tail should even tuck
What are the 2 tests you can perform to assess for damage in the brachial plexus?
1) Flexor (withdrawal) reflex
Again, looking for flexion of ALL the joints in the forelimb
Evaluates brachial plexus (RADIAL NERVE specifically) + C6-T2 spinal cord segments
2) Cutaneous trunci reflex
Is pinching of the skin over the dorsum (where you give booty scratches)
Evaluates the SENSORY nerves of the dorsal trunk (T2-L5) + CTL spinal cord segments + lateral thoracic nerve
Essentially looking for flinching of the muscle
Stimulus enters spinal cord segment associated with each block of muscle, called a dermatome (see image)
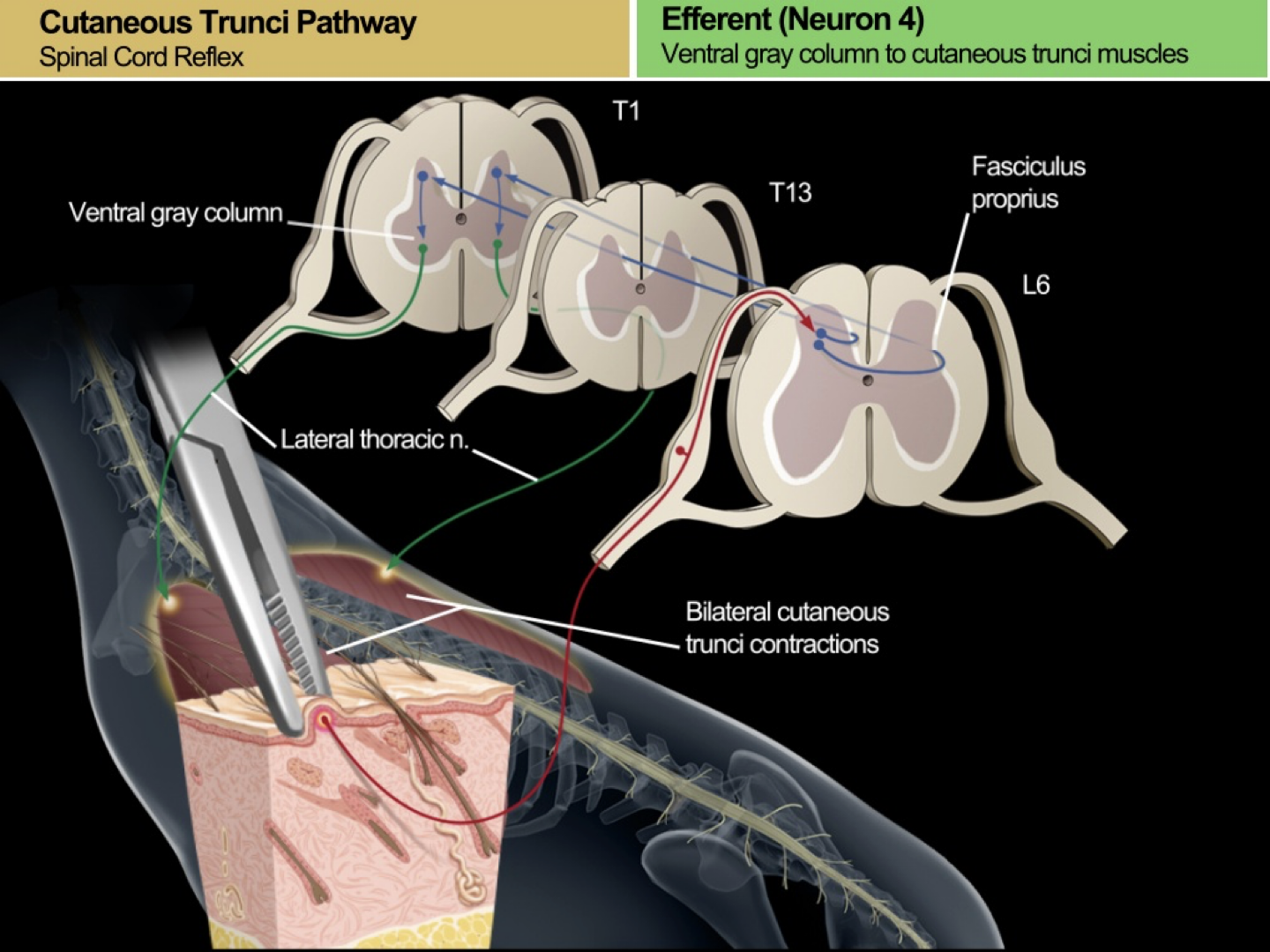
Describe how the nerve pathway of the cutaneous trunci reflex is different from the other reflexes?
Nociceptor is triggered by pain, and interacts with a pair of interneurons once signal travels to the dorsal horn of gray matter
These interneurons actually WRAP AROUND an area of the dorsal horn of gray matter called the fasciculus proprius, and travel UP the spine
These interneurons then communicate with interneurons in the vertebrae farther up the spine, which send the signal to EFFERENT neurons in the ventral horn
These then send a signal to contract the dermatome that they are associated with within the thorax
What are the 4 clinical signs of damage in the LMNs?
1) Affection of voluntary movement = weakness or complete paralysis
2) Affection of INvoluntary movements = reflexes reduced or absent
3) Reduced / absent basal muscle tone = flaccidity
4) Denervation of the muscles = quick atrophy
What are the 3 clinical signs of damage in the UMNs?
Affection of voluntary movement = weakness or paralysis
DOES NOT EFFECT INVOLUNTARY!!!!
Reflexes will still be present
Stiffness / spasticity
Since there is a LACK of inhibition from the UMN to the LMNs, this could result in increased (vigorous) reflex / involuntary movement
Some atrophy; will be SLOW and not very noticeable; will be due to disuse
What would happen if there was damage to the C1-C5 segment of the spine?
Loss of UMN in ALL 4 LIMBS
Voluntary movements affected in the 4 limbs
Present / increased INvoluntary movement
What would happen if there was damage to the C6-T2 segment of the spine?
Loss of LMN in the THORACIC limbs + loss of UMN in the PELVIC limbs
Voluntary movements affected in all 4 limbs
Involuntary movements affected ONLY in the forelimbs
What would happen if there was damage to the T3-L3 segment of the spine?
Loss of UMN in the PELVIC limbs
Voluntary movements affected
INvoluntary movements STILL PRESENT (or increased)
What would happen if there was damage to the L4-S3 segment of the spine?
Loss of LMN in the PELVIC limbs
Voluntary AND involuntary movements in the pelvic limb affected
Where is the damage in the spine if there is lack of nociception (deep pain)?
Could be damage to the UMN or LMN at ANY level
BAD PROGNOSIS
What is the ONLY diagnosis for whether or not an animal is experiencing deep pain?
BEHAVIORAL RESPONSE
If dog or cat REACTS to painful stimuli, then they can feel
Can’t base it off of whether or not the limb RETRACTS… remember, if there’s UMN damage, they can still perform involuntary actions without actually “feeling” it