6. kidney toxicants - ethylene glycol, NSAIDs, grapes/raisins, vitamin D
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
bloodwork/urinalysis tests of renal function
bloodwork
creatinine
blood urea nitrogen (BUN)
SDMA
urinalysis
proteinuria
glucosuria
specific gravity
pH
urinary sediments: casts, crystals
what are the 3 types of kidney injury?
vascular events
tubular cell injury
idiosyncratic
vascular kidney injury
renal ischemia resulting from persistent vasoconstriction & ↓ glomerular capillary permeability
initially causes pre-renal azotemia with no evidence of intrinsic renal injury
↓ renal blood flow and GFR can lead to tubular dysfunction secondary to anoxia
tubular cell injury
tubular damage and/or tubular obstruction
casts form from:
myoglobin or hemoglobin
necrotic tubule cells
crystals like calcium oxalate
casts may cause arteriolar vasoconstriction, tubular obstruction, and ↓ GFR
idiosyncratic kidney injury
not dose-dependent
unique to individual
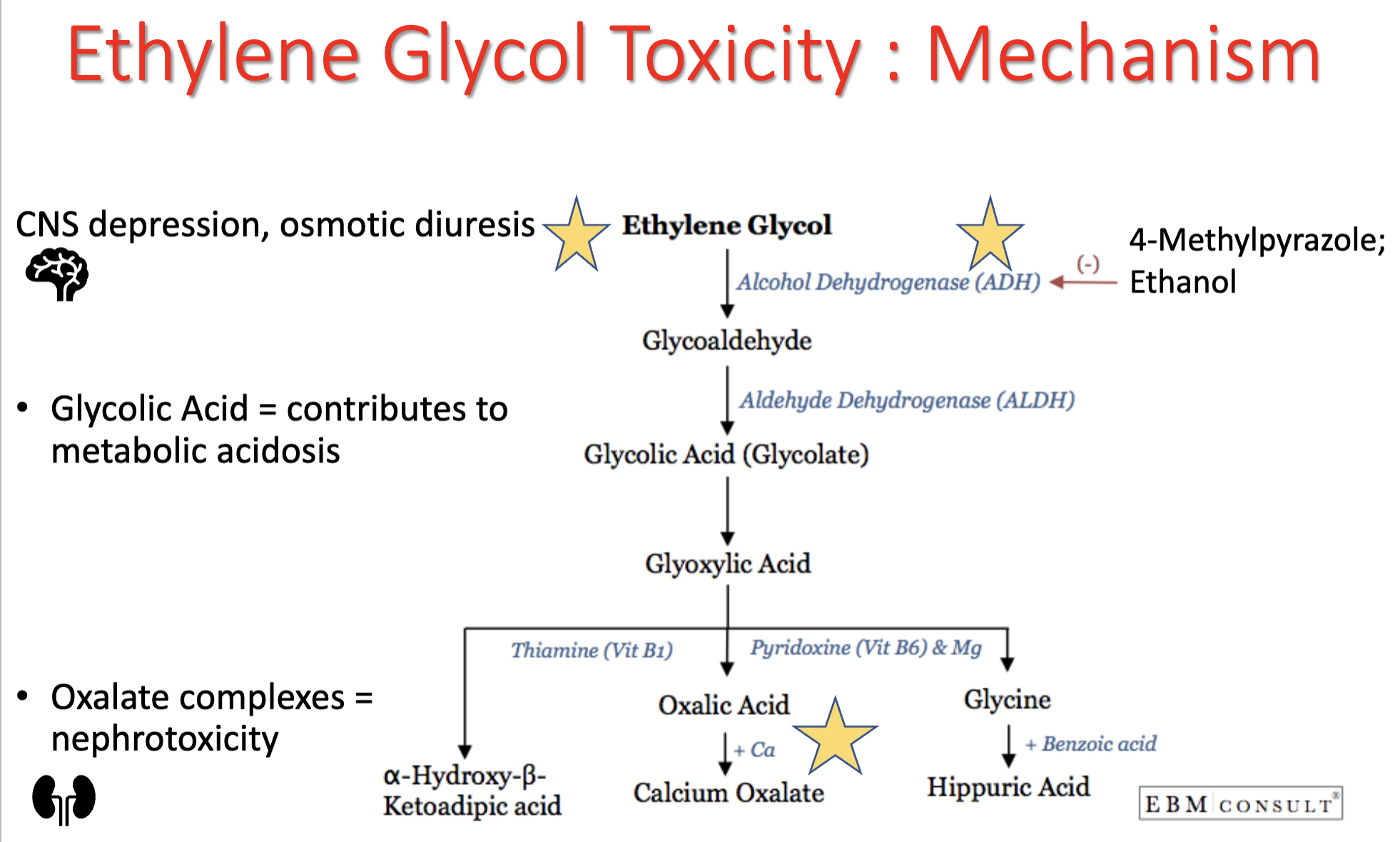
mechanism of ethylene glycol toxicity
ethylene glycol → can cause CNS depression, osmotic diuresis
metabolized by alcohol dehydrogenase in liver → → glycolic acid (glycolate)
glycolic acid = contributes to metabolic acidosis
further metabolism into oxalic acid
oxalate complexes = nephrotoxicity
calcium oxalate crystals → renal tubular epithelium necrosis
stages/timeline of ethylene glycol toxicity
stage 1: 30 min to 12 hrs post-ingestion
stage 2: 12-24 hrs post-ingestion
animal can appear to be recovering
stage 3: 24-72 hrs post-ingestion
which major organs/systems are affected by ethylene glycol toxicity?
CNS
urinary
detoxification treatment for ethylene glycol toxicity
prevent absorption with emetics (before clinical signs appear)
increase elimination with fluid therapy
activated charcoal NOT likely to be beneficial
treatment for preventing metabolism of ethylene glycol
4-methylpyrazole (4-MP, fomepizole) → inhibits alcohol dehydrogenase
ethanol (20%) → competes for alcohol dehydrogenase
do not use 4-MP and ethanol together, or ethanol after treatment with 4-MP
supportive therapy for ethylene glycol toxicity
fluid and electrolyte therapy
peritoneal dialysis or hemodialysis
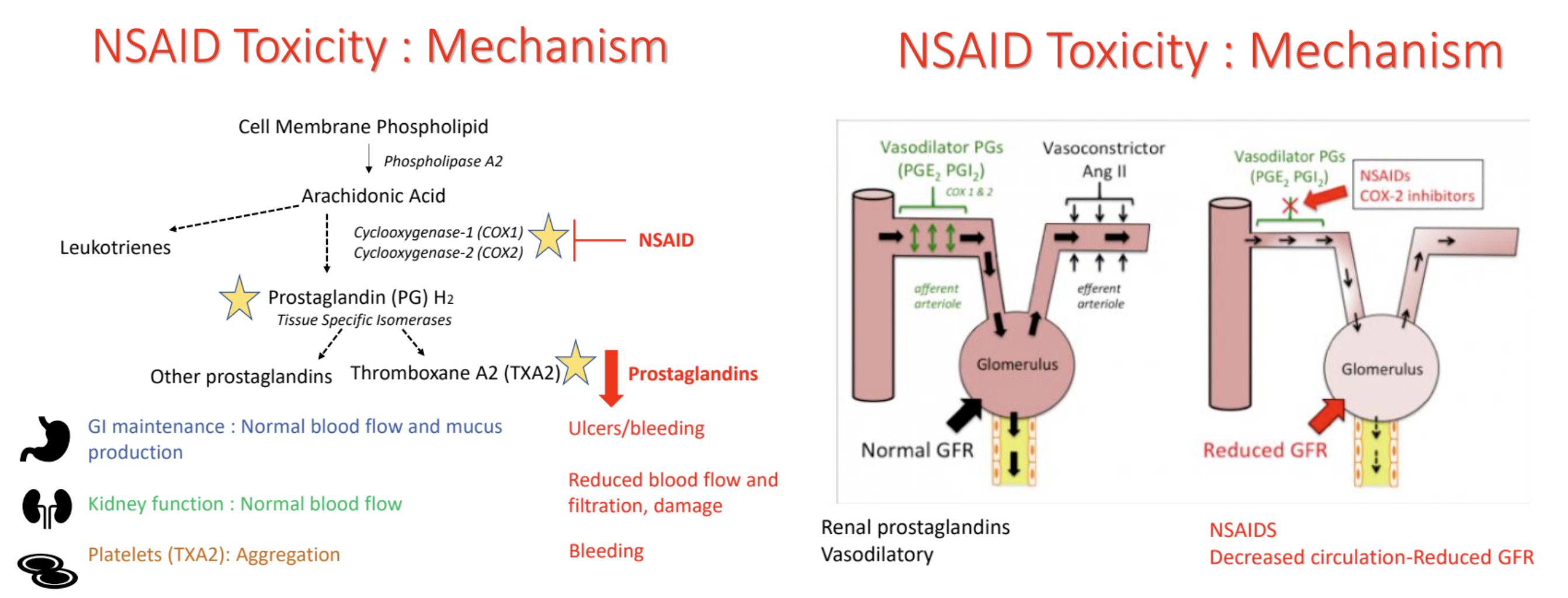
mechanism of NSAID toxicity
inhibits COX enzymes → block production of prostaglandins, including thromboxane A2 (TXA2)
GI → ulcers/bleeding
kidney → reduced blood flow & filtration, damage
platelets (TXA2) → bleeding (decreased aggregation)
which major organs/systems are affected by NSAID toxicity?
GI
kidneys
(CNS — high doses)
important toxicokinetic factors of ibuprofen (NSAIDs)
differ based on type of NSAID
metabolized by liver to inactive metabolites; excreted via urine
enterohepatic recirculation — feces (prolongs half life)
detoxification treatment for NSAID toxicity
prevent absorption with emetics (before clinical signs appear)
increase elimination with activated charcoal, cathartics, and fluid therapy
supportive therapy for NSAID toxicity
GI protectants — antacids, drugs to protect stomach lining, anti-emetic
misoprostol — synthetic prostaglandin E1 analogue
kidney — fluids, monitor blood BUN, creatinine; urinalysis → monitor for casts
CNS — treat neurologic signs symptomatically
severe cases may require blood transfusion
mechanism of grapes/raisin toxicity
renal failure — proximal renal tubular epithelium
only occurs in some dogs — idiosyncratic?
individual sensitivity among dogs
tartaric acid levels in grapes vary by region, ripeness, variety, growing conditions
clear dose-response relationship is not known
timeline of grapes/raisin toxicity
acute signs: 6-12 hrs
renal failure: 24-72 hrs
which major organs/systems are affected by grape/raisin toxicity?
GI
kidneys
treatment for grapes/raisin toxicity
detoxification
prevent absorption with emetics (even several hours after ingestion since grapes do not easily break down)
increase elimination with activated charcoal, cathartics, and fluid therapy
supportive therapy
kidney — fluids, monitor renal function & fluid balance
severe cases may require dialysis
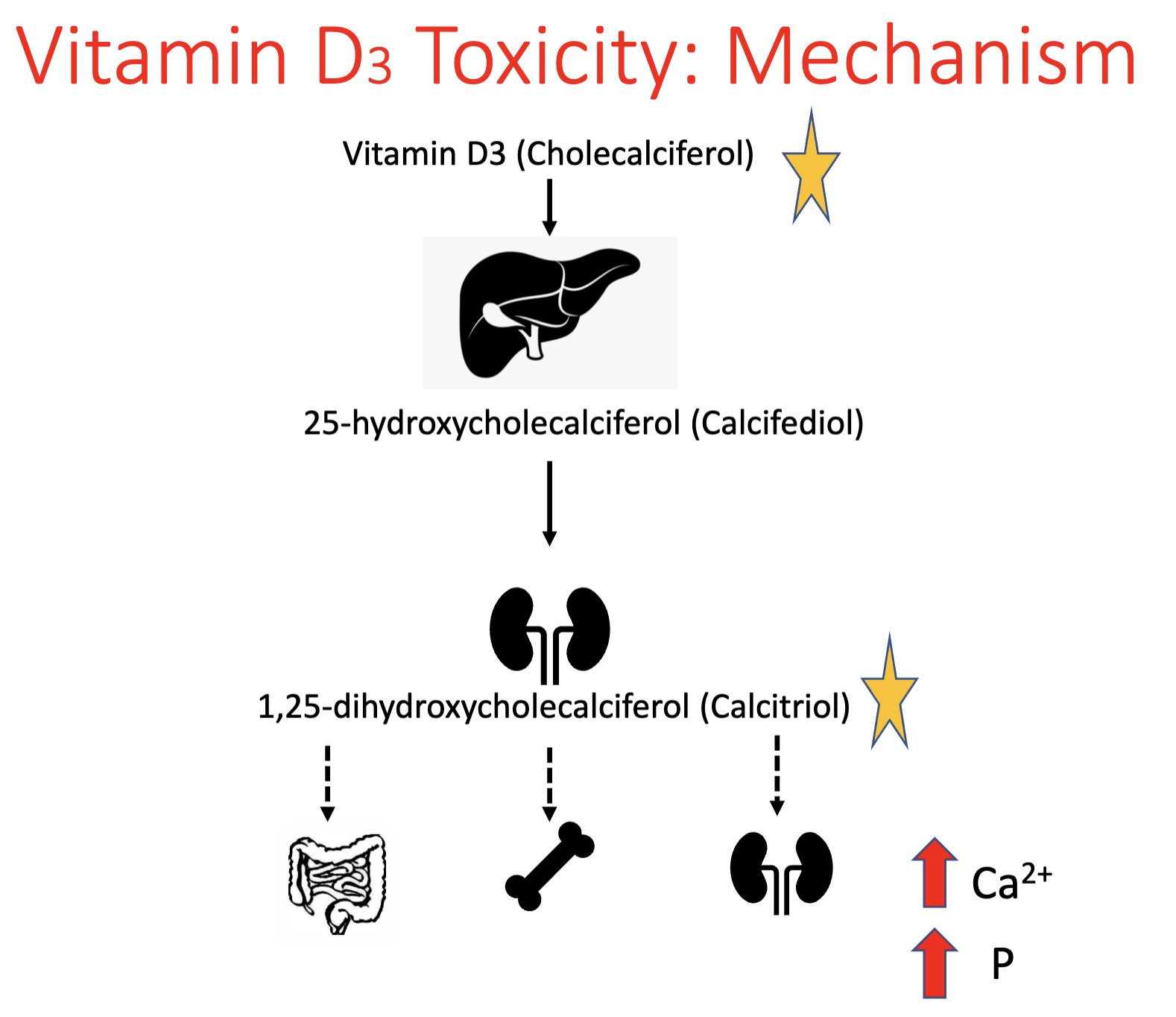
mechanism of vitamin D3 toxicity
vitamin D3 (cholecalciferol) → metabolized to calcitriol → results in ↑ Ca2+ & P
↑ GI absorption
↑ release from bone
↑ kidney reabsorption
**calcitriol binds vitamin D receptors with 1000x greater affinity than vitamin D3
effects of ↑ calcium (vitamin D3 toxicity)
vasoconstriction
soft tissue mineralization (structural damage)
↓ cell membrane permeability
↓ GI motility
↓ cellular energy production
cell death
timeline of vitamin D3 toxicity
initial signs: 18-36hrs
advanced/severe: 2-3 days
which major organs/systems are affected by vitamin D3 toxicity?
GI
kidneys
cardiovascular
important vitamin D3 toxicokinetics
rapidly absorbed, enterohepatic recirculation, excreted mainly via bile & feces
fat soluble (also prolongs half-life)
detoxification treatments for vitamin D3 toxicity
prevent absorption with emetics (early, asymptomatic)
increase elimination with activated charcoal and cathartics, diuretics
supportive therapy for vitamin D3 toxicity
kidney — fluid therapy, monitor renal function & fluid balance
monitor/correct calcium & phosphorus levels
IV lipid therapy
steroids — reduce bone resorption
GI support
low calcium, low phosphorus diet
** long term treatment may be necessary