Hearing Science Final
1/175
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
176 Terms
Basilar Membrane (BM)
A structure in the cochlea that moves in response to sound waves, influencing the bending of stereocilia in hair cells.
Stereocilia
Tiny hair-like structures on hair cells that bend in response to sound vibrations, initiating the process of hearing.
Depolarization
The change in electrical potential across a cell membrane, leading to the generation of a neural signal.
Cochlear Amplifier
A feedback system involving outer hair cells that enhances sound sensitivity and frequency selectivity in the cochlea.
Otoacoustic Emissions (OAE)
Sounds generated within the cochlea, reflecting the active processes of outer hair cells, which can be spontaneous or evoked.
Afferent Fibers
Nerve fibers that carry sensory information from the cochlea to the brain.
Efferent Fibers
Nerve fibers that transmit signals from the brain to the cochlea, modulating auditory processing.
Cochlear Nucleus
The first relay station for auditory information processing in the brainstem.
Superior Olivary Complex (SOC)
A brainstem structure that integrates input from both ears, crucial for sound localization.
Tonotopic Organization
The spatial arrangement of sound frequency processing, where different frequencies are represented in distinct anatomical locations.
Auditory Cortex
The region of the brain responsible for processing auditory information, particularly speech and sound.
Heschel's Gyrus
The primary auditory cortex located in the temporal lobe, crucial for auditory perception.
Wave III of the ABR
An auditory brainstem response wave associated with processing at the level of the cochlear nucleus and SOC.
Wave V of the ABR
An auditory brainstem response wave associated with processing in the lateral lemniscus and inferior colliculus.
threshold
Intensity needed for an individual to just detect the presence of a stimulus. In a clinic the subject has to note hearing the sound 50% of the time it is presented.
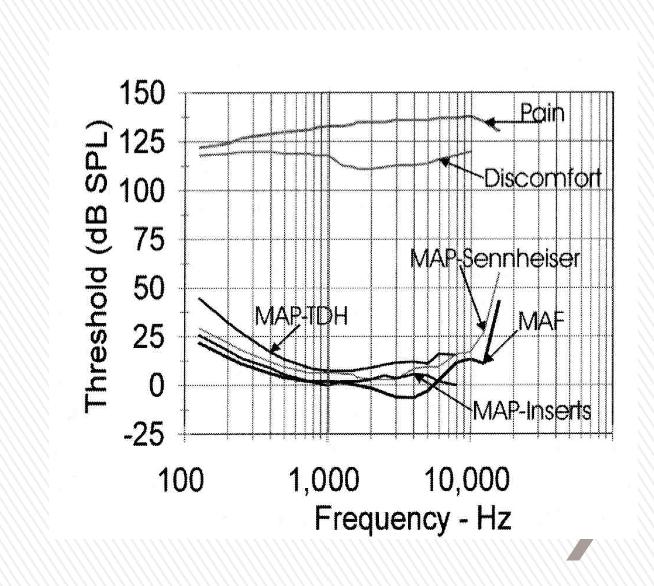
minimum audible field (MAF) curve
Plot of threshold as a function of frequency. Measured in sound field, both ears allowed to participate; yields better sensitivity. Measured in free field using loudspeakers. Group averages. People with reported good hearing health
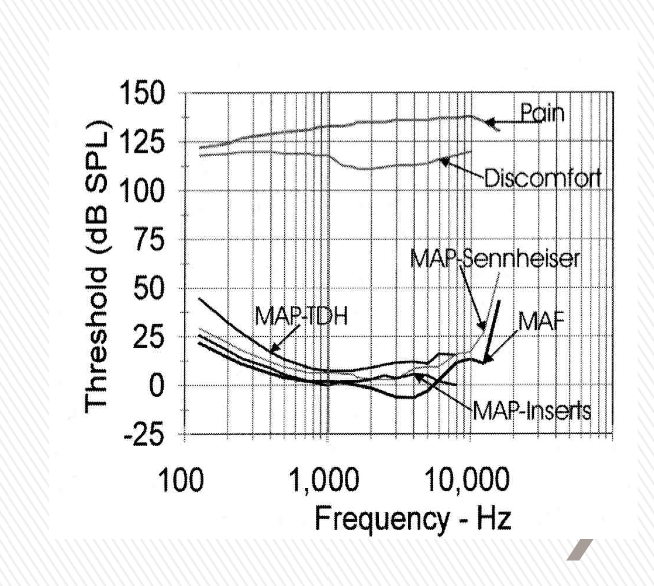
Minimum audible pressure (MAP) curves
Measured under earphones, so one ear at a time. Group averages. People with reported good hearing health.
What matters in measuring threshold for hearing?
The condition of the individual matters
The stimulus matters (steady, pulsed, warbled tone)
How we ask “Can you ____?” matters.
The environment we test in — matters
Calibration of equipment matters
purpose of testing matters ($$)
Obtained from a neural/physiological response or does client need to signal.
Methods of Limits (most commonly used)
Set the frequency - start at 1000 Hz
Present a tone - start around 40 dBHL
Client responds drop down 10 dB to 30 dBHL
Continue dropping by 10 dB steps until the client stops responding
Go up in steps of 5dB until client responds
Decrease by 10 dB
Bracket looking for 2 responses at one level
Methods of Limits is accurate for clinical purposes, easy to do, and efficient. Ages 4 and up can do this 3 yo can drop a block.
Importance of Instructions
You can guess if not sure leads to false positive responses & lower thresholds
Wait until you are sure leads to higher thresholds, but fewer false positives
Hughson-Westlake (1959) “The purpose of this test is to see how well you can hear some faint tones. Each tone will be quite short. Some will be easy to hear. Others will
be quite faint. Whenever you hear one of these tones, no matter how faint it is, raise your finger. As soon as the tone goes off, lower your finger.”
HIT
correctly responding to a tone
Miss
did not respond and tone was there
False positive
subject responds, no tone there
Correct rejection
No response and not tone
Ascending run
Start out below threshold and raise the intensity in steps. Higher thresholds, harder to hear “coming from nothing”. Good if you think someone is malingering as they cannot use your test tone intensity to “set” their response limits. Used by the Veteran’s Administration.
Bekesy audiometry
Client has the controls. Hold the button down as long as you hear it, let up when you do not. Method of adjustment. Not really used clinically. Threshold is the halfway point between peaks on the resulting graph.
Method of Constant Stimuli
Experimental technique, not used clinically. “Constant” number of stimuli are given per intensity per frequency. Randomize order of the intensities presented. Tally how many correct hits happen. Threshold is the intensity at 50% hit rate.
Experimental issues in threshold detection
Noise - breathing, ambient noise, clothing.
Instructions
Age
Guesser
Reward systems
Air Conduction Audiometry
purpose: determine if hearing loss exists and if it does, specify the amount of hearing loss.
The results of air conduction testing give us the degree of hearing loss, but does not tell us the etiology of the hearing loss (i.e., is it conductive, mixed, or sensorineural?)
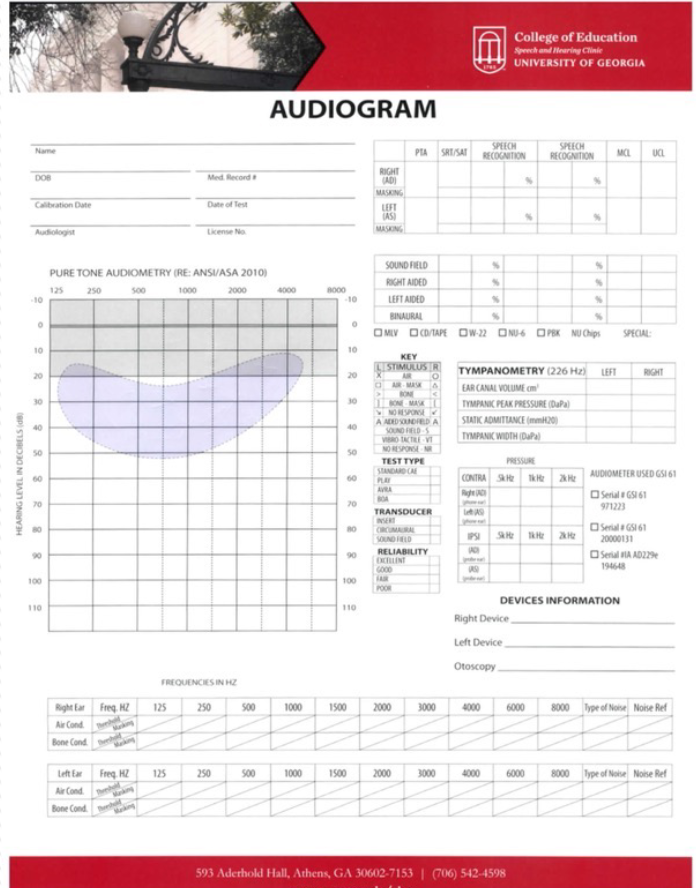
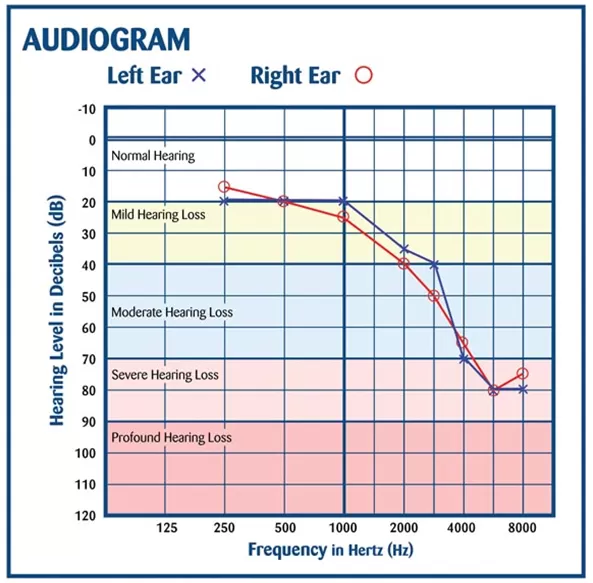
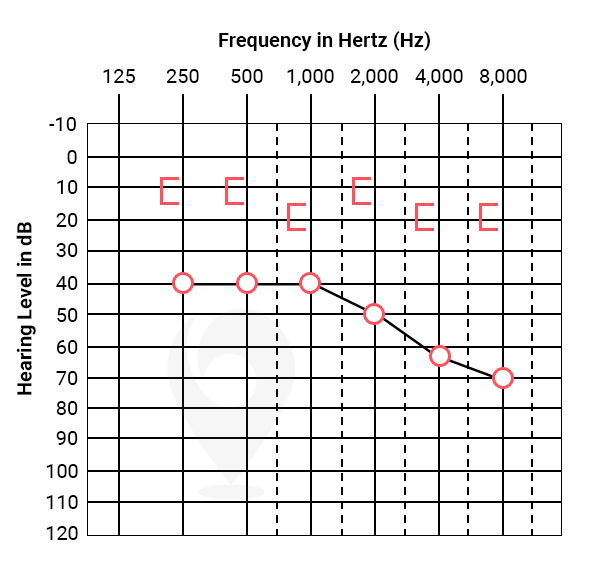
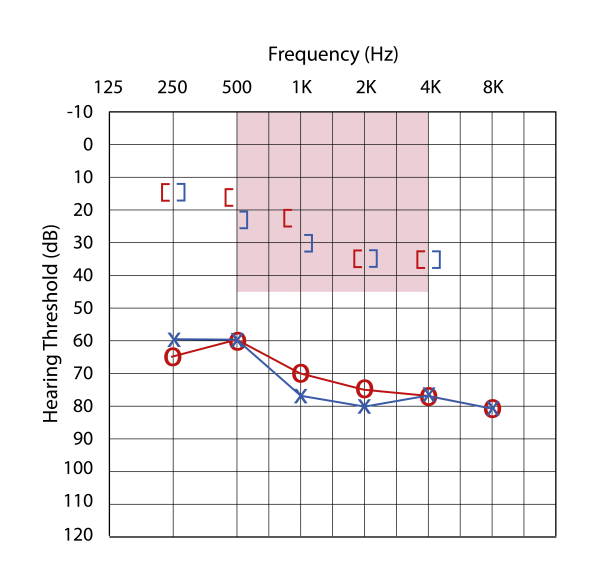
Audiogram
person’s individual threshold displayed.
“O”
Right ear (red) -air conduction
“X"
Left ear (blue) -air conduction
SF
Sound Field -air conduction
“∆“
Right ear (masked) -air conduction
“⎕“
Left ear (masked) -air conduction
“<“
Right unmasked -bone conduction
“>”
left unmasked -bone conduction
“[“
right masked -bone conduction
“]”
left masked -bone conduction
“┐”
forehead -bone conduction
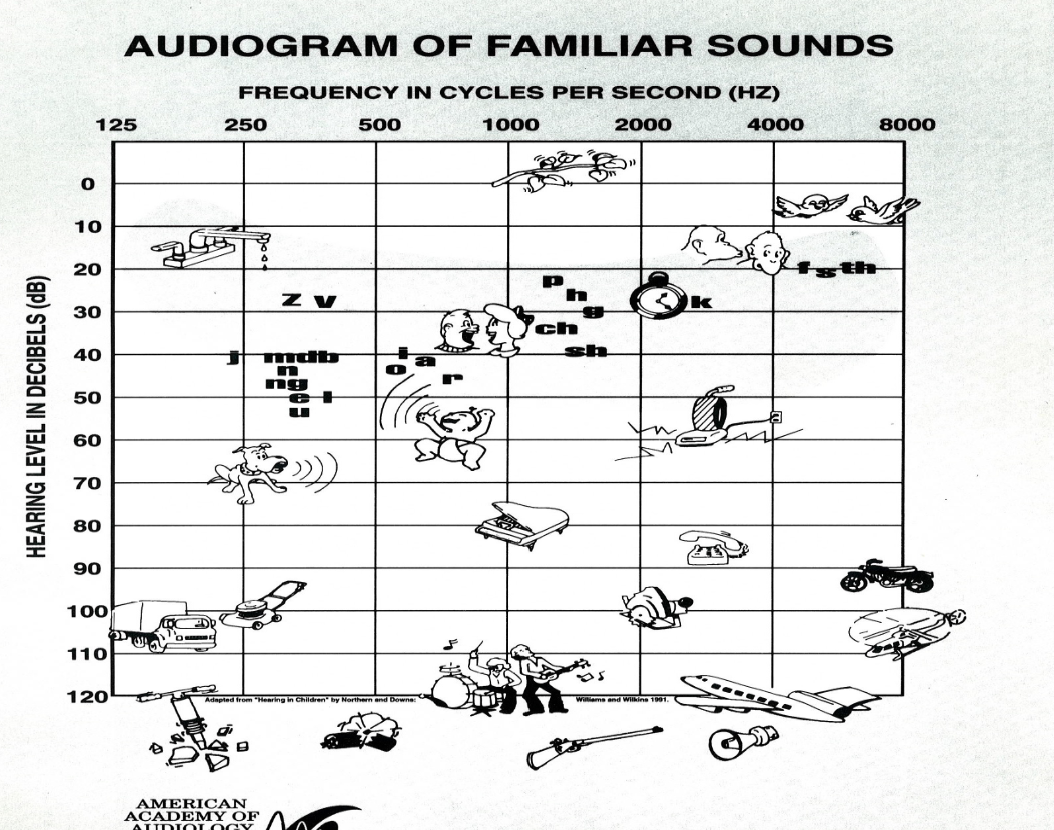
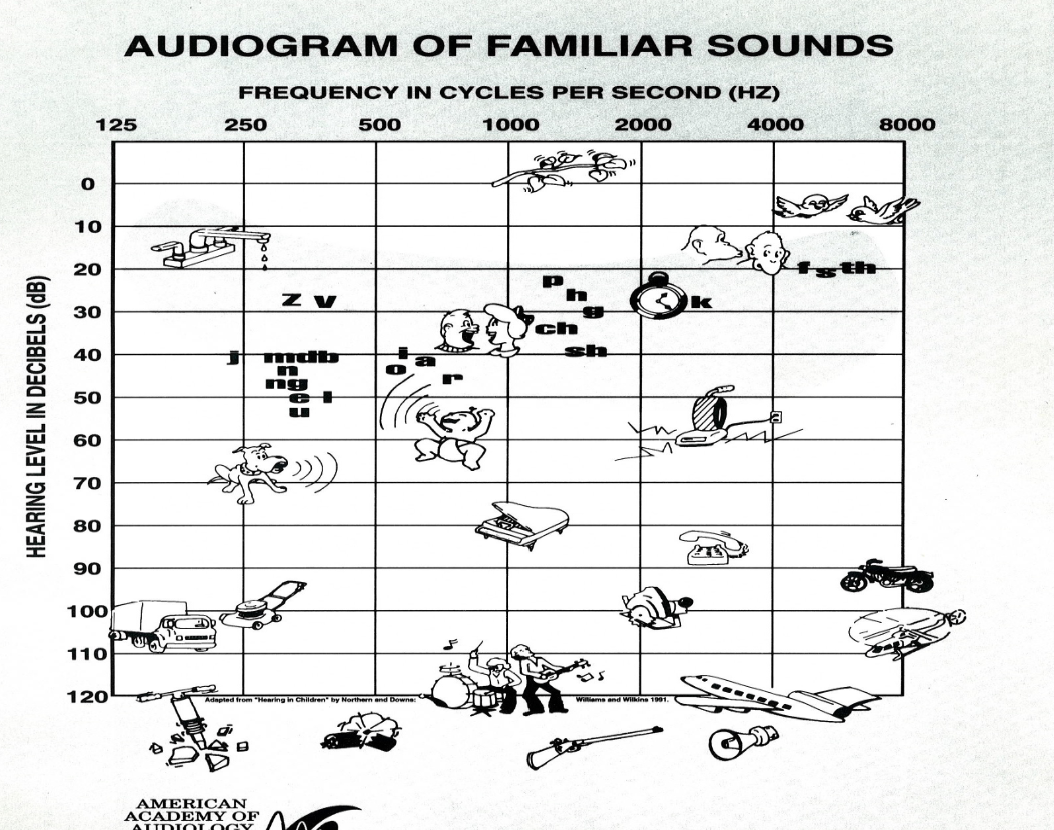
Normal loss (school aged)
0 - 15 dB HL
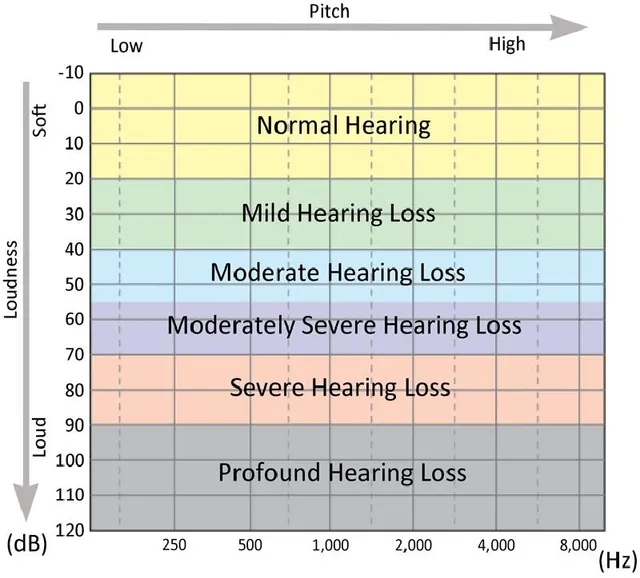
Slight (school aged)
16 - 25 dB HL
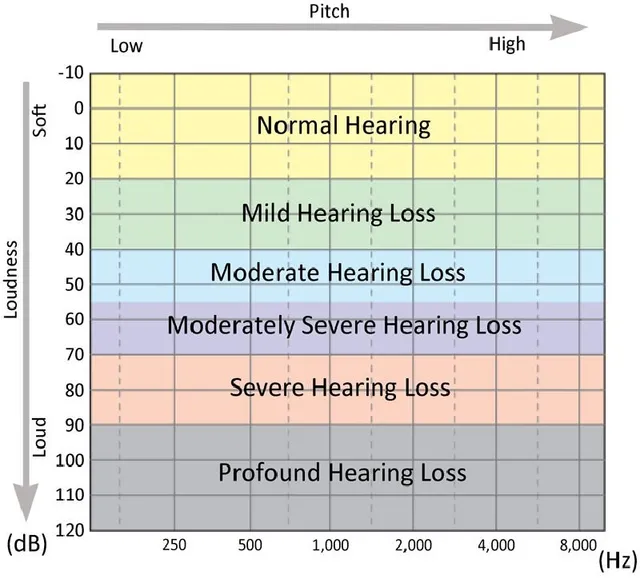
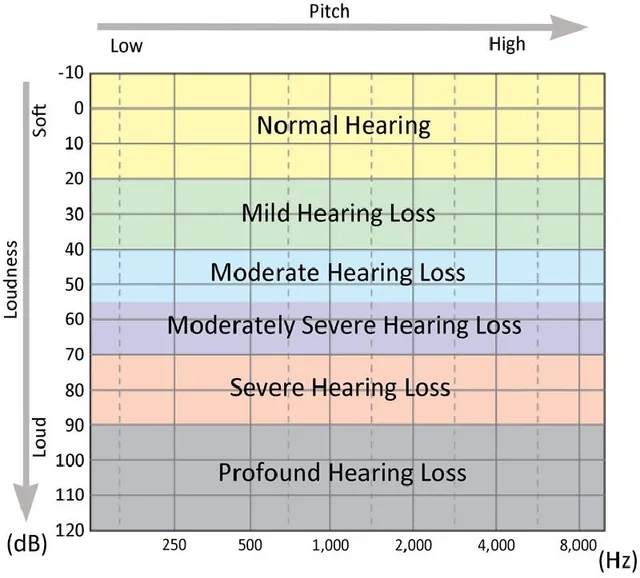
Normal (adult)
0 - 20 dB HL
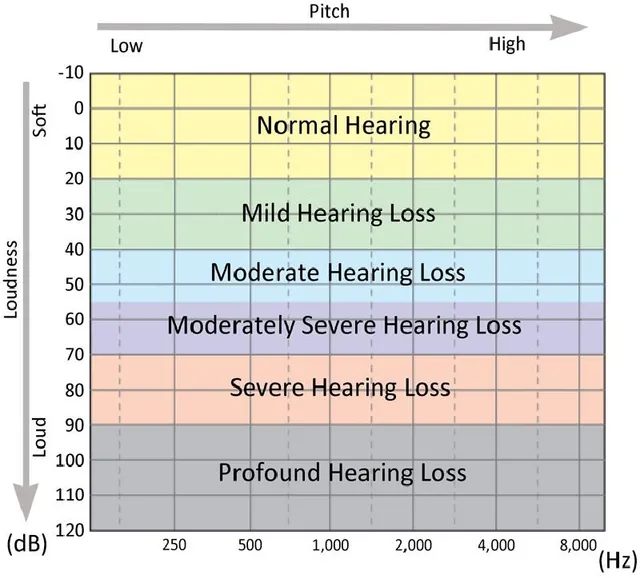
Mild
21 - 40 dB HL
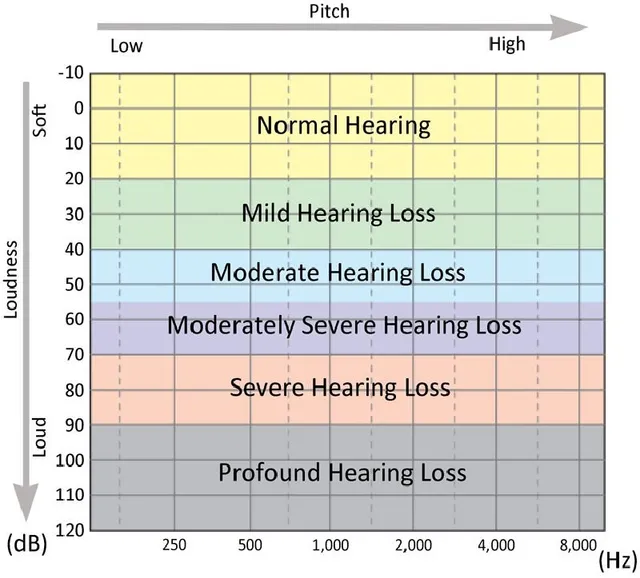
Moderate
41 - 55 dB HL
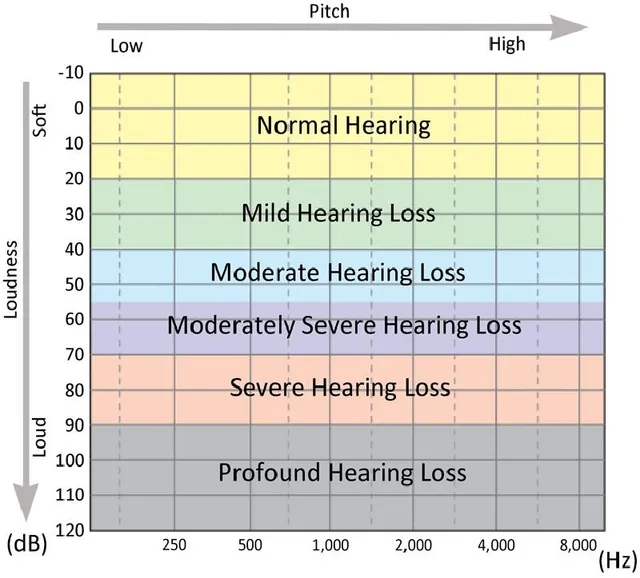
Moderately Severe
56 - 70 dB HL
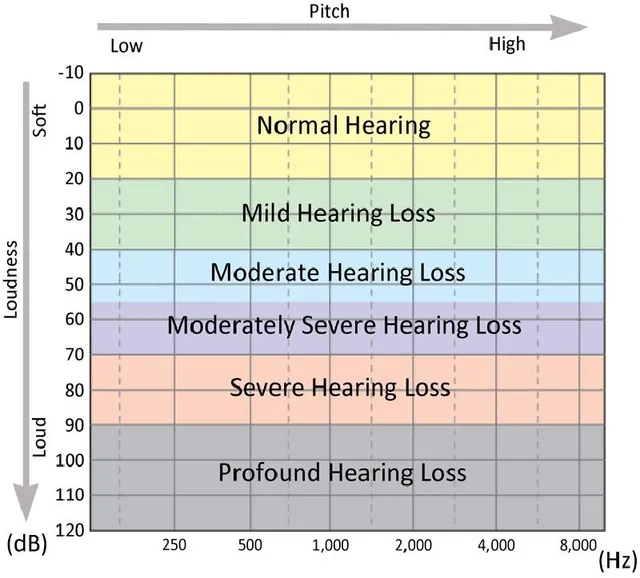
Severe
71 - 90 dB HL
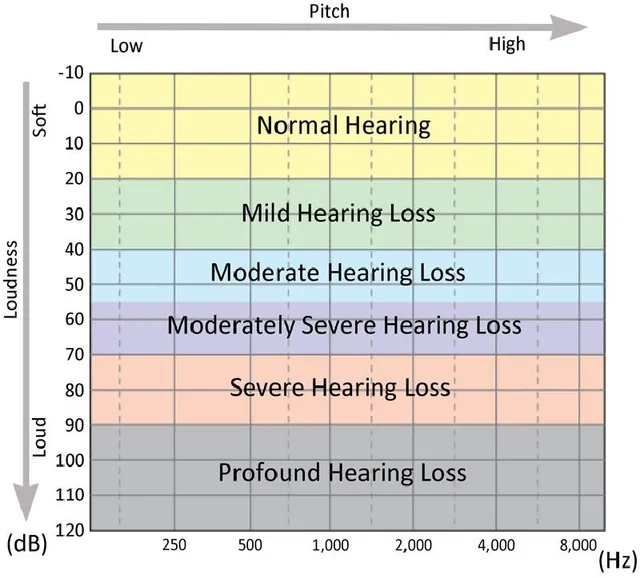
Profound
91+
visual reinforcement audiometry
For babies starting at 6 - 8 months of age, baby is distracted by distractor, second audiologist plays sound through speaker and baby turns head towards sound and reward stimuli.
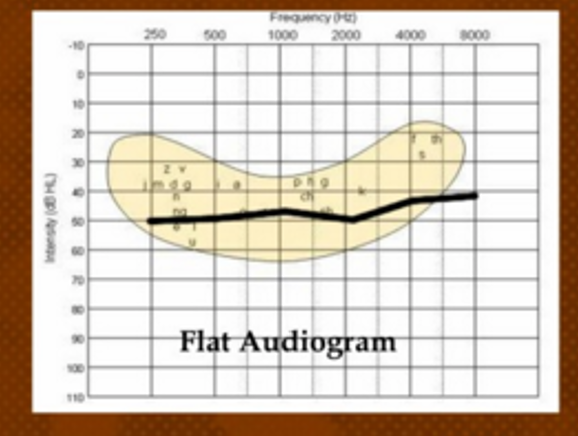
flat configuration
hearing loss starts and stops in the same range
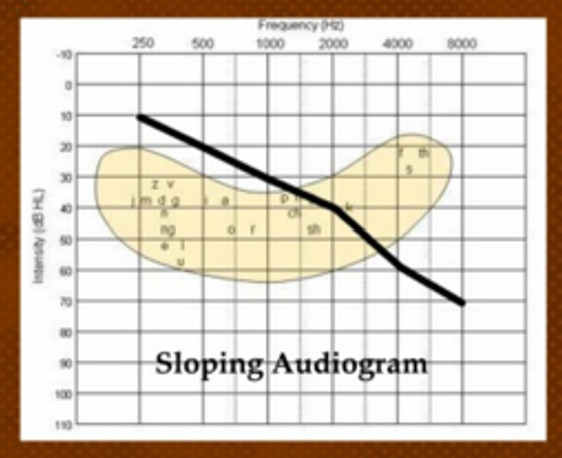
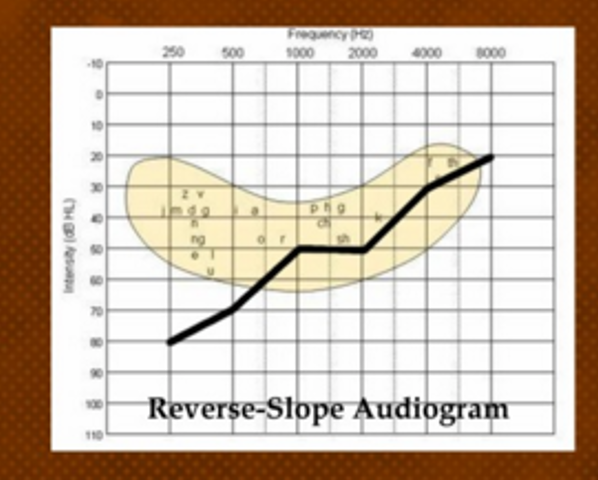
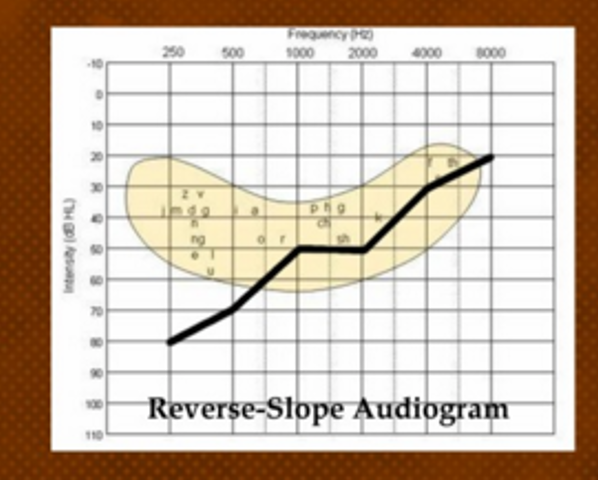
Sloping configuration
hearing loss begins better than it ends
Rising configuration
hearing loss is worse and then rises to better
High Frequency
can be used instead of sloping, when a HL is just in the high pitches
Low frequency configuration
used interchangeably with rising
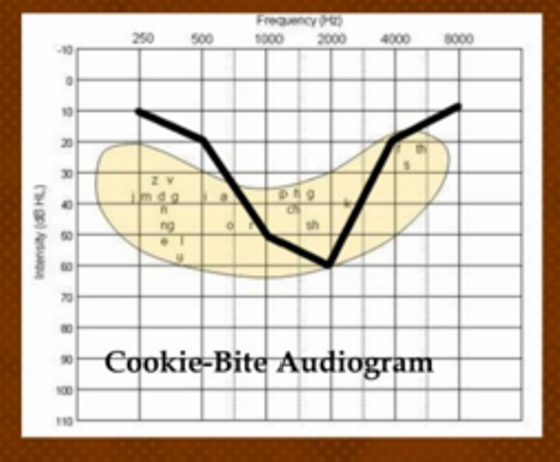
cookie bite configuration
when the hearing loss is normal at both ends and the loss is in the mid pitches only
Interpretation of results
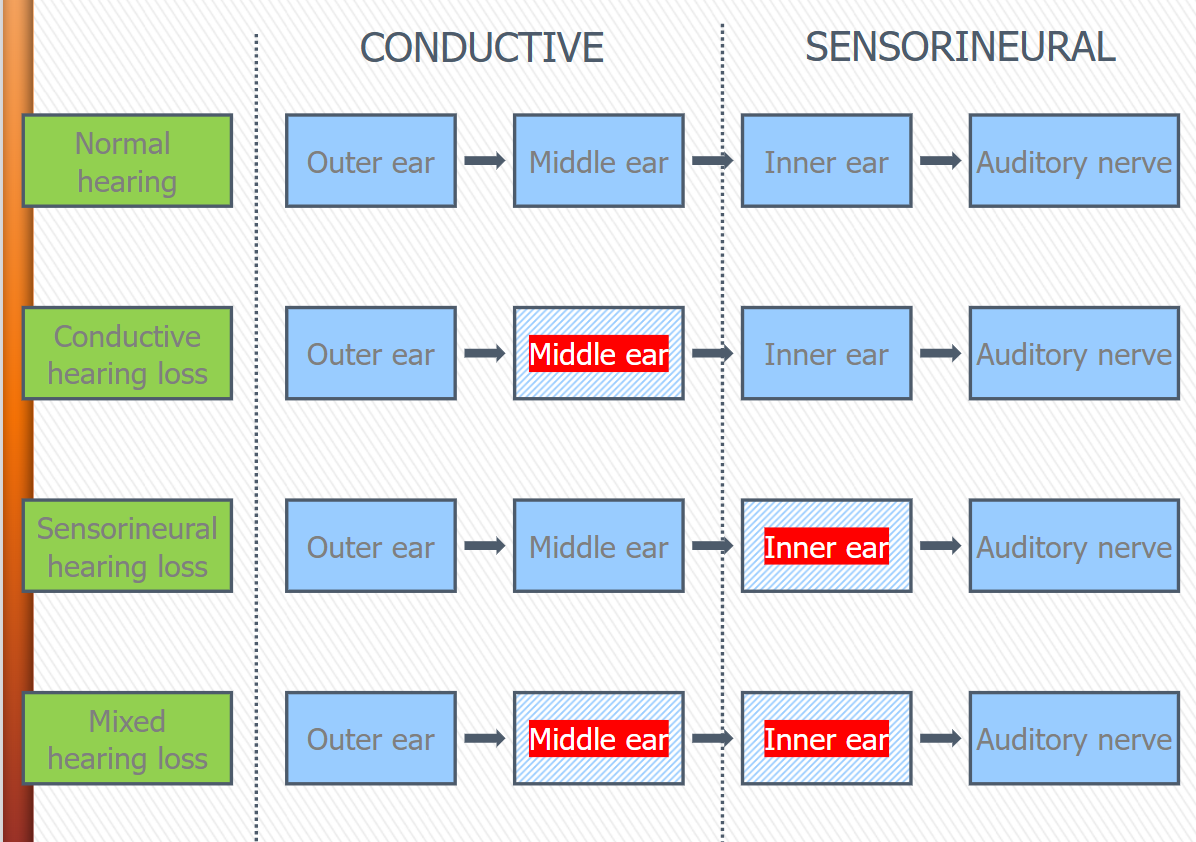
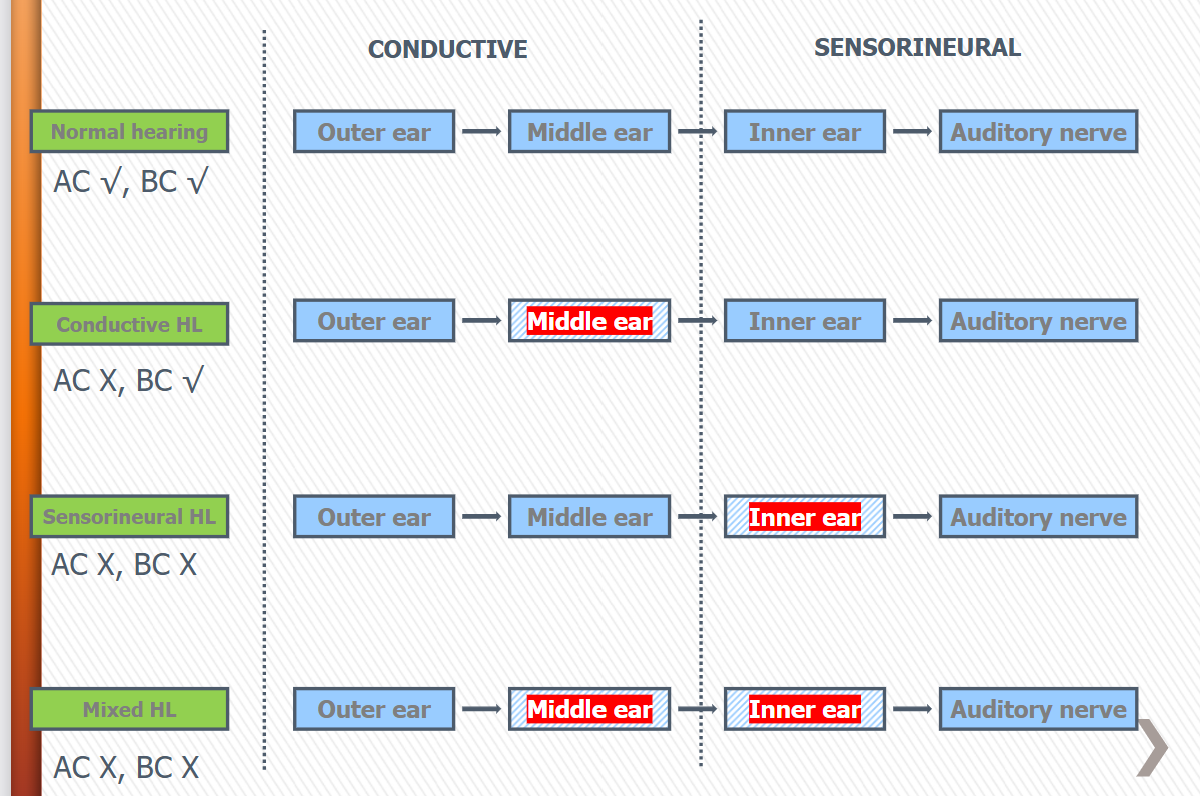
Normal hearing
hear is within normal hearing limits
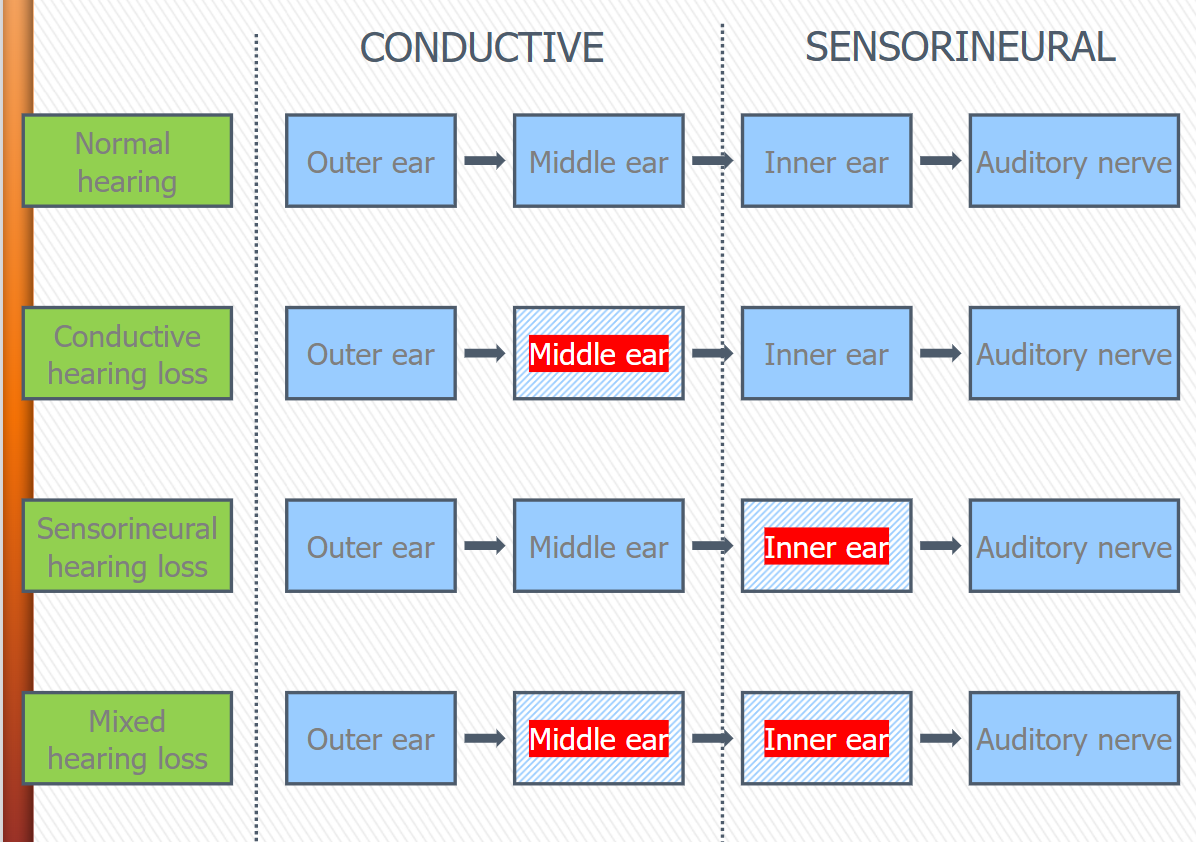
Conductive hearing loss
(CHL) hearing loss is within the outer or middle ear - when there is a loss in air conduction but not bone conduction
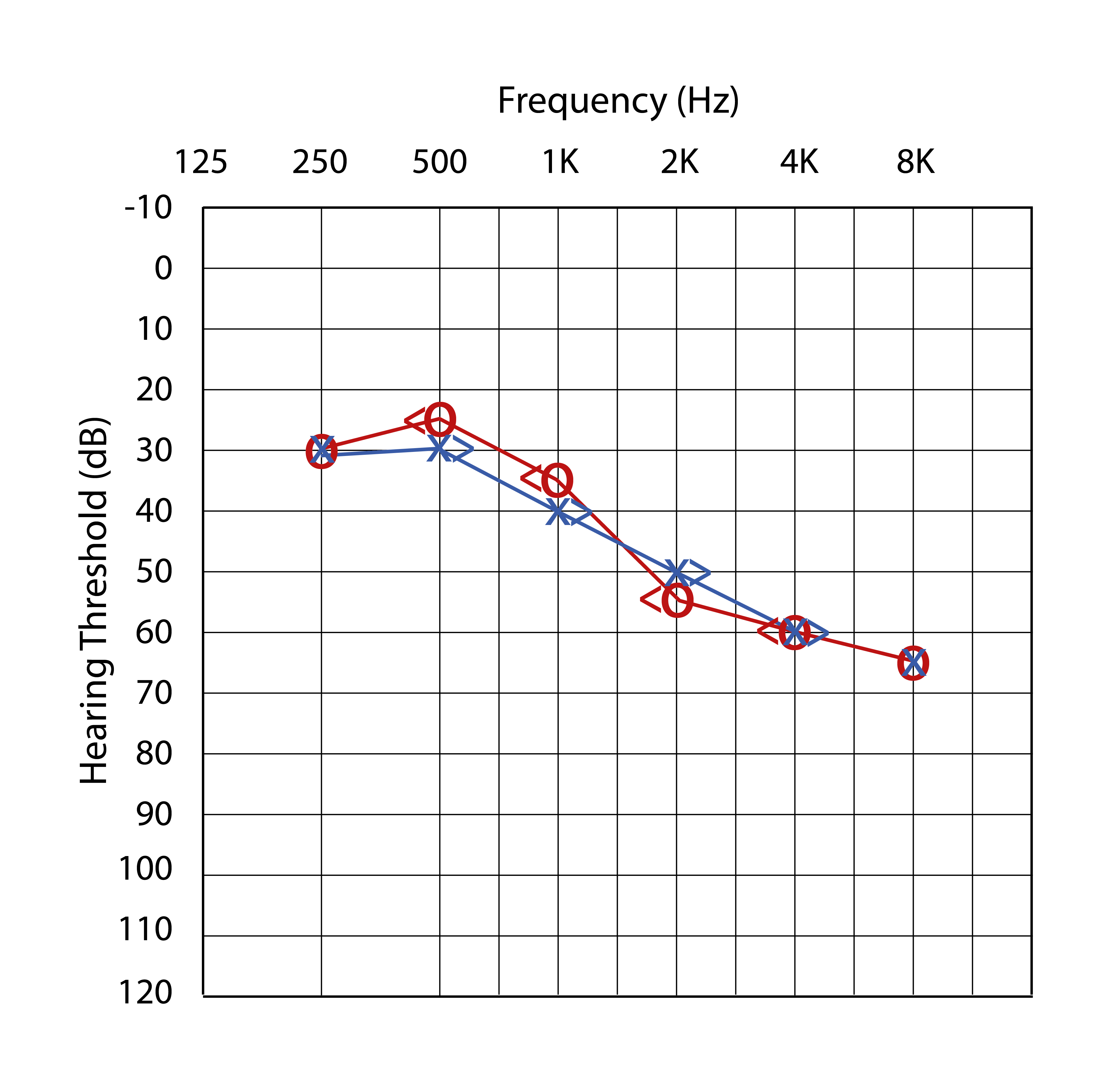
Sensorineural hearing loss
(SNHL) there is a hearing loss in bone conduction as well, bone and air conduction are the same loss
Mixed hearing loss
There is a bone conduction hearing loss and a worst loss with air conduction as well.
peripheral auditory system
external ear (pinna, external auditory meatus)
middle ear (tympanic membrane, ossicles, middle ear cavity)
inner ear (cochlea and vestibular system)
Auditory nerve (VIIIth Cranial nerve)
Central auditory system
auditory nerve
parts of the brain (cochlear nucleus, superior olivary complex, lateral lemniscus, inferior colliculus, medial geniculate body, and cortex)
middle ear
sound conduction into the inner ear with minimal loss due to impedance mismatch
External ear
sound conduction into the middle ear
localization
Inner ear
transduction of sound from mechanical input to neural output
Auditory nerve
carrying the neural impulse to the brain
Air conduction (AC)
transmission through outer, middle, inner ear, and higher up.
sounds presented by headphones, insert earphones, loudspeakers
Bone conduction (BC)
Transmission that stimulates the inner ear directly through mechanical vibration of the skull
Sounds presented through a bone vibrator
Temporary
true TTS is due to damage from loud sounds. K+ does not have time to leave the cell-swelling
Permanent
Destruction of hair cells or basilar membrane, chronic or acute noise exposure. NIHL.
Hearing losses, bone vs air
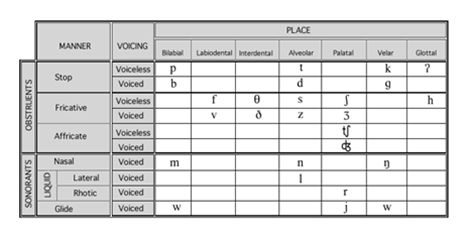
Place of articulation, manner of articulation, and voicing
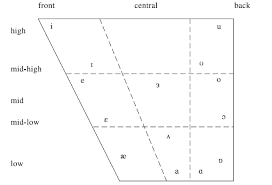
Vowel Quadrilateral
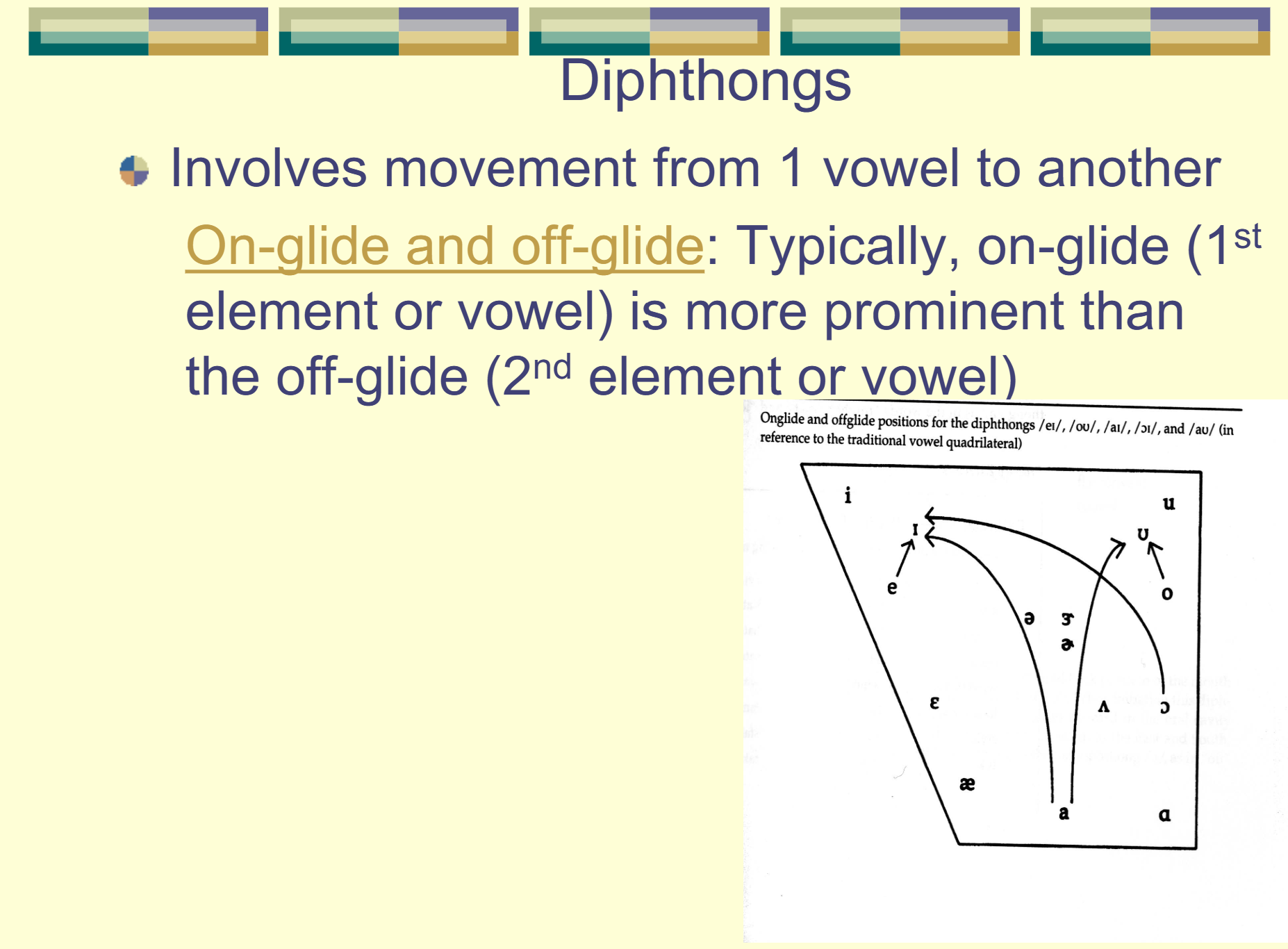
Dipthongs
Anterior/Ventral
In front, toward face
posterior/dorsal
behind toward the back of the head
Lateral
toward the side of the head
medial
toward middle of head
superior
above toward top of head
inferior
below toward the feet
cranial/cephalic
toward the head
caudal
toward the tail
Outer Ear
Conductive - Pinna, EAM (external auditory meatus), Tympanic membrane
Middle Ear
Conductive - TM, ossicles (malleus, incus, and stapes), and ligaments and muscles
Inner Ear
Sensorineural mechanism - Vestibular Apparatus, cochlea (basilar membrane and organ of corti), and auditory nerve
Conductive Loss
problem with the outer and/or middle ear
sensory
issue is in the cochlea
neural
issue is in the VIIIth cranial nerve
Sensorineural
issue with the cochlea and/or VIIIth nerve
Mixed
conductive and sensorineural both involved
central loss
central auditory system dysfunction
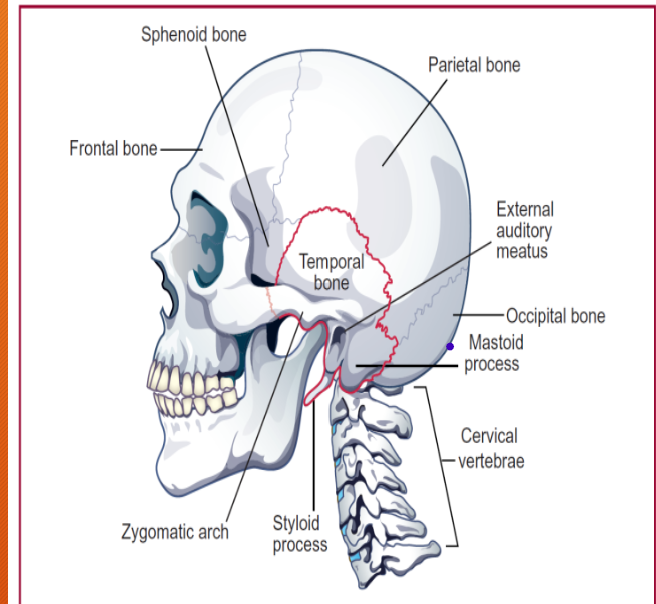
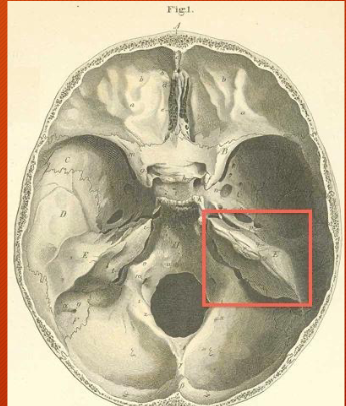
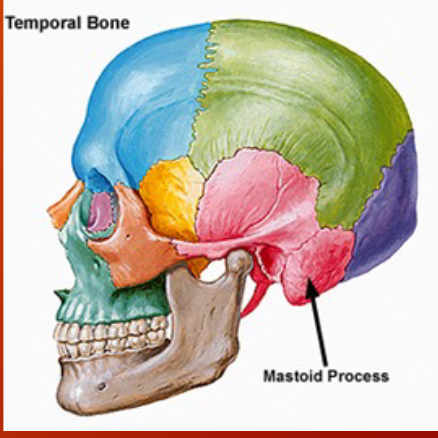
Temporal Bone
Encases most of peripheral auditory structures except cartilaginous part of the external ear and the short portion of the auditory-vestibular nerve between the opening of the internal auditory meatus and the brainstem -complexly shaped. Protects inner ear structures, contains two important openings: external and internal auditory meatuses.
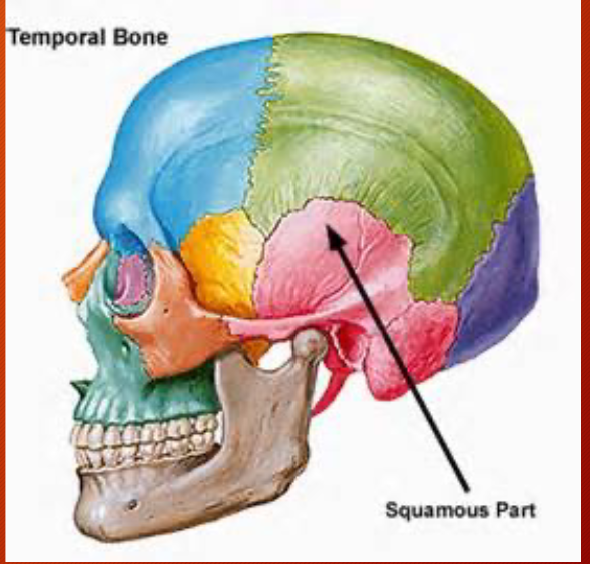
4 portions: squamous, petrous, mastoid, and tympanic
Squamous - Temporal Bone
Protects the temporal lobe of the brain
Petrous - Temporal Bone
Floor of the cranium, very hard, thick, protective, surrounds the inner ear (balance and hearing)
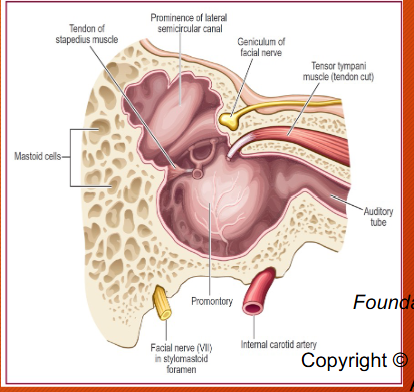
Mastoid - Temporal Bone
air filled (honeycomb, strong and light). Upper front par - tympanic antrum is air filled and lined by prolongation of the mucous membrane of the tympanic cavity. Tympanic antrum bound above by the tegmen tympani which separates it from the middle fossa of the base of the skull; below by the mastoid process; laterally by the squama just below the temporal line and medially by the lateral semicircular canal of the internal ear which projects into its cavity. It opens in front into that portion of the tympanic cavity which is known as the attic or epitympanic recess.
Mastoiditis
Infection of the mastoid. Sequela of untreated middle ear infections. bacterial in nature. Chronic or acute in nature, and can result in removal of the bone.
Tympanic - Temporal bone
The base and walls of the middle ear space
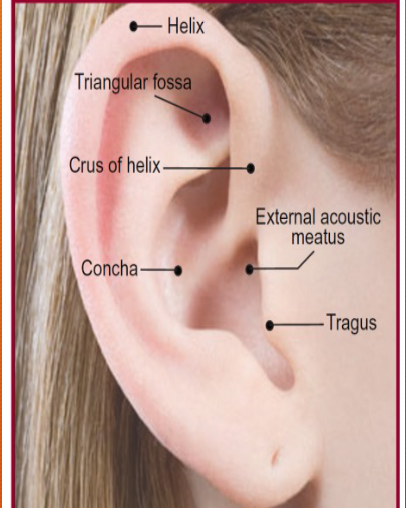
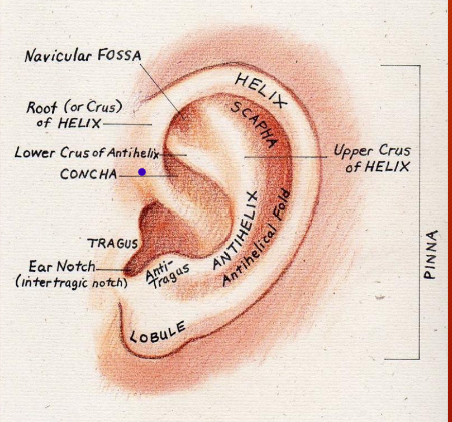
Pinna or Auricle
Poorly innervated, very variable, vestigial muscles, 4 dB increase in sound level, minimal localization. Structures are composed of cartilage; the cartilage continues part way into the external auditory meatus. Structures of the pinna play a role in localizing enviro sounds in the up-down and front-back dimensions and high pitch sounds from back of the hear.
Funnels sound into ear. Has a resonance around 5000-6000 Hz. Blocks high frequency sounds that are coming from behind the ear.