Nitrous Oxide Analgesia
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
97 Terms
Who can administer it
only by appropriately licensed individuals, or under the direct supervision thereof, according to state law (DDS, Dental Hygienist, Dental Assistant in Indiana
-dentist must be present
HB 1067
Sec. 10.7. (a) A dental hygienist or dental assistant may administer
nitrous oxide under the supervision of a licensed dentist if the dental
hygienist or dental assistant has:
(1) been employed in a dental practice for at least one (1) year or has graduated from a program accredited by the Commission on Dental Accreditation of the American Dental Association;
(2) satisfactorily completed a three (3) hour didactic educational program or curriculum, consisting of HB 1067—LS 6482/DI 119 5 pharmacology, biochemistry, anatomy of nitrous oxide administration, and the mechanics of operating a nitrous unit, accredited by the Commission on Dental Accreditation of the American Dental Association; and
(3) demonstrated clinical competency on at least five (5) patients under the direct supervisionof a licensed Indiana dentist whose license is in good standing
(Dentist responsibility)
(b) The licensed Indiana dentist supervising the clinical competency
under subsection (a) shall provide to the dental hygienist or dental
assistant a signed affidavit certifying the competency. (c) Upon
receipt of the affidavit provided to a dental hygienist or dental
assistant under subsection (b), the provider of an educational
program or curriculum described in subsection (a) shall issue a
certificate of completion to the dental hygienist or dental assistant.
The certificate of completion must be publicly displayed in the
dental office of the dental hygienist or dental assistant. (d) Before
permitting a dental hygienist or dental assistant to administer nitrous
oxide, the supervising dentist shall verify that the dental hygienist or
dental assistant has completed the requirements of subsection (a).
Physical and chemical properties of dinitrogen monoxide (N2O)
Boiling point of N2O is -88.5 C so it is a gas at room temperature
N2O is a colorless, non-irritating, slightly sweet-smelling, non-flammable gas at room temperature
N2O can become combustible if it comes in contact with a combustible substance (oil, grease) or flame
Known as “laughing gas” due to the euphoric effects it produces when inhaled
-most commonly prepared by heating ammonium nitrate which decomposes into nitrous oxide and water
-above 240 degrees the exothermic reaction may accelerate to the point of detonation, so the mixture must be cooled
-85 – 90% of N2O is used in healthcare settings
can be habit-forming; long term use has been associated with vitamin B-12 deficiency anemia, suppressed hemopoiesis, neuropathy, tinnitus, numbness in extremities, and teratogenic defects
History
Dr. Horace Wells-father of anesthesia; pioneered use of NO2 for it; tooth extraction 1st procedure that used it as a anesthetic
Joseph Priestley (1772) -discovered oxygen and nitrous oxide gases called nitrous oxide “dephlogisticated nitrous air”
Humphrey Davy (1798) -British chemist who was the first person to inhale 100% nitrous oxide and described the sensation of euphoria
Gardner Quincy Colton, MD -introduced nitrous oxide to the medical profession (1863)
1868- Edmund Andrews added 20% oxygen to the nitrous oxide gas mixture
1872- Liquid nitrous oxide became available
1881- S.S. White began supplying nitrous oxide in metal cylinders
1887- Sir Fredrick Hewitt incorporated O2 into a machine that delivered both gases
1975- Fail-safe O2 mechanism introduced to prevent the delivery of 100% N2O
The individual credited for the discovery of nitrous oxide was
________________.
A. Humphrey Davy
B. Joseph Priestley
C. Gardner Quincy Colton
D. Horace Wells
The individual who has posthumously been recognized as the
“Father of Anesthesia” is ____________.
A. Humphrey Davy
B. Joseph Priestley
C. Gardner Quincy Colton
D. Horace Wells
The first clinical procedure using nitrous oxide as an anesthetic
agent was _______________.
A. limb amputation
B. tooth extraction
C. abscess drainage
D. laceration repair
b, d, b
Anatomy/physiology of N2O/O2
Respiratory system
designed to perform the function of exchanging gases, carbon dioxide (CO2) and oxygen, (O2) across pulmonary capillary membranes
Respiration is driven at 2 anatomic sites:
1) Automatically by the brainstem (medulla oblongata)
2) Voluntarily by the cerebral cortex
Its function is to promote gas exchange to and from the alveoli and the blood
Anatomy of the upper airway
N2O enter the respiratory tree at the nose
The nose warms the incoming air and filter particles
Anatomic conditions that affect air passage through the nose may interfere with N2O/O2 delivery
The nasopharynx is located behind the nasal cavity
The soft palate separates the nasopharynx from the oropharynx
The oropharynx opens into the mouth and serves as a link between the nasopharynx and the laryngopharynx
The laryngopharynx begins at the epiglottis, which directs material prevents objects from entering the trachea during swallowing
The larynx lies inside the laryngopharynx
If the larynx is irritated, the defensive cough reflex is initiated
Thyroid cartilage and cricoid cartilage provide protection to the underlying pharynx
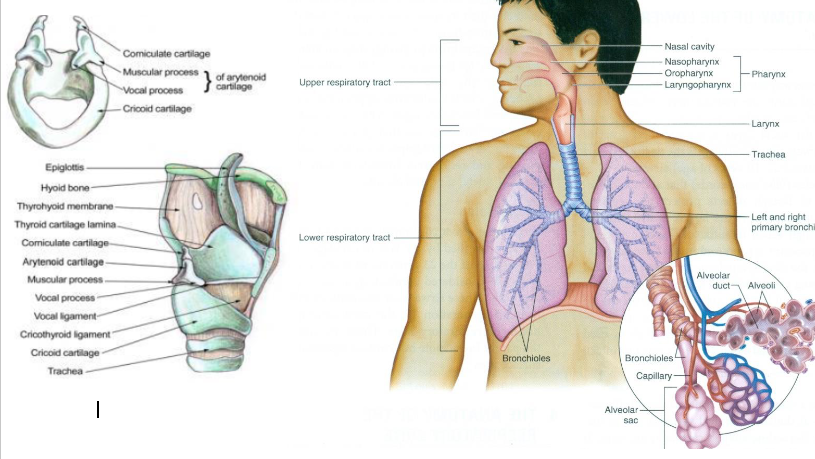
Anatomy of the lower airway
The glottal opening at the vocal cords in the larynx is the narrowest part of the adult airway
The cricoid ring is the narrowest part of the pediatric airway
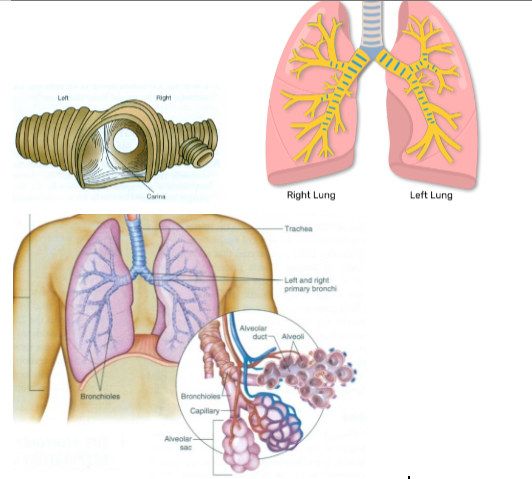
The trachea bifurcates into the right and left bronchi
The carina is located at this bifurcation and will initiate and strong cough reflex if an object passes through the larynx
The right bronchus is where foreign objects are more commonly directed toward the right lung
The left bronchus is more that twice as long as the right bronchus and diverges more from the trachea
Bronchioles are a continued division of the bronchi
Alveolar sacs “pouch” to form thin-walled alveoli
The exchange between air and blood takes place in the 300 million alveoli
Physiology of respiration
The medullary center of the brainstem controls the automatic process of breathing
Active inspiration is controlled primarily by the diaphragm and external intercostal muscles
Air continues to flow until pressures from the inside the lung are equivalent to atmospheric pressure
Expiration occurs passively; it only becomes active when changes in respiratory demand occur
The amount of gas inspired into the lungs depends on the physical characteristics of the individual- larger individual’s chest cavities hold more volume than smaller individuals
Minute ventilation is the amount of gas brought into the lungs each minute
Example: 500 mL X 12 respiration/minute = 6 L/minute
Excess gas forced through into the nasal hood will escape because it is not consumed by the patient
Alveolar ventilation is the amount of air per minute entering the alveolar units capable of gas-blood exchange
Anatomic dead space = the portion of inhaled gas that does not enter the lungs (about 150 mL)
After N2O is terminated, N2O is forced into the alveoli and exhaled through the lungs
N2O exits the blood faster than Nitrogen (N2) that replaces it diluting the supply of O2; this is called Diffusion Hypoxia which is why it is recommended to administer 100% oxygen for 5 minutes after termination of N2O
There is dispute as to the necessity of administering 100% oxygen after the termination of N2O
Some studies have found that O2 levels stabilize independently within 12 seconds to 15 minutes
Signs of Diffusion Hypoxia include post-operative headache, lethargy and nausea
Pulse oximetry measures the oxygen saturation of arterial blood (amount of oxygen carried by hemoglobin)
Normal level = 96 – 100%
<90% is a warning of impending loss of oxygen to the brain
The use of a pulse oximeter is required for moderate sedation (American Society of Anesthesiologists)
Hypoventilation can occur during sedation as a result of respiratory depression so observing the airway during treatment is important
Observing the airbag on the Nitrous Oxide delivery machine is a way to monitor continuous patient respiration
Capnometry used infrared light technology to measure the concentration of CO2 at expiration
Normal adult lung capacity
(6000 mL or 6L)
1. Tidal volume (500 mLor 8%) – normal amount of air inhaled and exhaled during breathing
2. Inspiratory volume (3100 mLor 52%) – maximum amount of air that can be forcefully inhaled after tidal inspiration
3. Residual volume (1200 mLor 20%)
4. Expiratory volume (1200 mL or 20%)
Minute ventilation
(volume) is the amount of gas brought into the lungs each minute
Calculated by multiplying the tidal volume by the rate of respiration
12-20 respirations is the normal
Determines the amount of gas mixture (N2O/O2) that should be given to a patient
Monitoring of patients experiencing moderate sedation (>50% N2O)
Non-anesthesiologists who treat patients in a hospital are legally required to adhere to the ASA practice guidelines
Practitioners treating patients outside of a hospital setting are responsible for treating the complications associated with sedation
Periodic monitoring of patient’s response to verbal commands
Use of a Pulseoximeter with an alarm
Airway management
Monitor possible airway obstruction caused by dorsum of the tongue occluding with the posterior pharyngeal wall
The universal distress signal for choking is for one to grasp the throat with both hands
If there is a foreign body obstruction, apply abdominal thrusts
Summon emergency personnel if the patient is unconscious
Hyperextension (head tilt – chin lift) or a jaw thrust maneuver should relieve an airway obstruction that is not caused by a foreign body
Should vomiting occur, place the patient in an upright position or turn them to the side and clear vomitus from the oral cavity
If the ______ is irritated, the defensive cough reflex is initiated.
A. larynx
B. trachea
C. carina
D. Nasopharynx
a) larynx
What level of oxygen saturation would be considered normal for
a healthy individual?
A. 66%
B. 76%
C. 86%
D. 96%
D) 96%
The term used to define the decrease in blood oxygen saturation
caused by rapid exit of nitrous oxide is _____ _____.
A. diffusion hypoxia
B. pulmonary effusion
C. arterial anoxia
D. aortic stenosis
a) diffusion hypoxia
The bronchus with minimal divergence from the trachea and more
likely to receive a foreign body is on the patient’s ____ side.
A. right
B. left
a) right
Signs and symptoms of nitrous oxide and oxygen sedation
Psychologic
Patient is relaxed and comfortable
Patient acknowledges a reduced sense of fear and anxiety
Patient’s mood may be categorized as happy, pleasant, satisfied, or ambivalent
May observe signs of vasodilation on the skin in head and neck area
Body movement
Shoulders dropping, legs uncrossing, arms positioned looser on armrests
Patients usually take deeper respirations
Patient describes a feeling of “warmth”
Patient may describe a feeling of tingling in their extremities
Eye and Facial signs
Before sedation, the patient’s eyes will follow the clinician’s actions and movements; as sedation continues, the patient’s eye movement will decrease and may appear to have a “glazed” appearance
Muscles in the patient’s forehead and brow will be relaxed, smiles easily
Signs and symptoms of nitrous oxide and oxygen over sedation
Patient may experience fits of uncontrollable laughter or crying
Patient may complain of nausea or floating sensation and may vomit
Disassociation or out-of-body experiences may occur
Patient’s words may become slurred or not coherent
Patient may experience dizziness, light-headedness and spinning sensations
Patient may describe sensation of tingling or shaking throughout their entire body
Patient may become unconscious
Each of the following are signs of an appropriate level of nitrous oxide/oxygen sedation except one. Which one is the exception?
A. Patient is comfortably warm
B. Patient smiles easily
C. Patient is unable to keep mouth open
D. Patient indicates tingling sensation in extremities
C) Patient is unable to keep mouth open
Each of the following are signs of administering too much nitrous oxide except one. Which one is the exception?
A. Slow eye blink rate
B. Dizziness
C. Nausea
D. Slurred speech
E. Floating sensation
A) Slow eye blink rate
All patients appropriately sedated with N2O/O2 will have intact
cough and gag reflexes.
A. True
B. False
true
Which of the following is an appropriate sequence of events of
sedation which will lead to a relaxed and comfortable patient?
A. Awareness of surroundings to detachment of environment
B. Active eyes to slowed blink rate to inability to keep eyes open
C. Appropriate verbal response to slurred, inaudible speech
D. Slight tingling in extremities to vasodilation in face and neck
D) slight tingling in extremities to vasodilation in face and neck
Nitrous oxide interaction with the cardiovascular system
N2O does not negatively affect blood pressure, heart rate, cardiac output or blood flow to major organs
Vasodilation can occur with N2O administration which can cause flushing around the patient’s face and neck
Nitrous oxide interaction with the respiratory system
Upper respiratory infections and sinusitis may impact adequate air exchange causing inadequate sedation
Patient with COPD (emphysema, chronic bronchitis) are susceptible to hypoxia because of airway resistance
Recommend a medical consult for patients with COPD
Patients with Cystic Fibrosis who incur bullae as a complication of the disease should not be administered N2O
N2O should be avoided for patients with pneumothorax
Nitrous oxide interaction with the CNS system
N2O has the ability to suppress the CNS Evidence of injury to the CNS (numbness, weakness in extremities, ataxic gait) has been shown in cases of chronic exposure to N2O
Nitrous oxide interaction with the Hematopoietic system
Megaloblastic bone marrow changes have been found in patients exposed to high concentrations of N2O
N2O may interfere with DNA synthesis and production of erythrocytes causing anemia
Patients with Vitamin B12 deficiencies should obtain a medical consult
GI system
If a patient has a bowel obstruction, N2O should not be administered due to the fact that it diffuses into the GI system faster than it exits
Reproductive system
N2O crosses the placenta to the developing baby
The literature cites that N2O is safe to use on pregnant patients, but a medical consultation is recommended
Avoid N2O administration during the 1 st trimester
Cancer
N2O does not combine with any blood elements nor does it affect metastatic cells
Patients taking bleomycin sulfate (lymphoma, testicular tumors, breast cancer) are at increased risk for pulmonary fibrosis
Mind altering conditions
N2O use should be avoided in patients intoxicated with drugs or alcohol
Avoid use in patients recovering from addiction- may exacerbate or trigger a relapse
Avoid use in patients taking antidepressant or psychotropic drugs
Avoid use in patients with claustrophobic tendencies
Other concerns
Avoid N2O use in patients with middle ear problems such as tympanic membrane grafts
Avoid use in patients who have recent eye surgery
N2O may potentiate the effects of drugs that induce sleep
An absolute contraindication to the use of N2O/O2 sedation
would be a patient with __________.
A. angina
B. a gastric ulcer
C. Parkinson disease
D. being treated for cancer with bleomycinsulfate
D) being treated for cancer with bleomycinsulfate
On which of the following body systems does nitrous oxide have
the greatest impact?
A. Central nervous system
B. Hepatic
C. Skeletal/muscular
D. Cardiovascular
a) CNS
An indication for use of N2O/O2 sedation is a patient who _____.
A. has severe claustrophobia
B. has a hypersensitive gag reflex
C. has a current upper respiratory tract infection
D. is currently intoxicated
E. is in the first trimester of pregnancy
B) has a hypersensitive gag reflex
A relative contraindication for the use of N2O/O2 sedation
includes the following with one exception. Which situation is the
exception?
A. Patient with psychotic illness taking several medications
B. Patient who does not have the mental capacity to understand
the procedure
C. Patient has undiagnosed anorexia with nutritional deficiencies
D. Patient is being treated for Hepatitis C
D) patient is being treated for hepatitis C
Analgesic properties
Nitrous oxide has the ability to manage both pain and fear
A mixture of 80% oxygen and 20% nitrous oxide has the analgesic equipotence as 15 mg of morphine
Nitrous oxide has the ability to raise the patient’s pain threshold prior to administering intraoral injections
Anxiolytic properties (sedative effects)
A person’s ability to cope with fear and pain can depend on factors such as age, gender, previous experiences and personality
Nitrous oxide produces sedation, a sense of well-being and a calming effect
Nitrous oxide use in pediatric patients has been shown to facilitate positive behavior and lowered anxiety levels on sequential visits
Amnestic properties
Patients state that after nitrous oxide administration, they cannot recall the severity of pain or anxiety of its duration during the procedure
The passage of time tends to become compressed or unclear while under nitrous oxide sedation
Onset of action
Rapid onset of action (< 30 seconds) with peak effects occurring in < 5 minutes
Onset of action is similar to intravenous (IV) sedation The depth of sedation can easily be lightened or deepened by adjusting the level of nitrous oxide delivered to the patient
Elimination and recovery
Nitrous oxide is eliminated from the body rapidly moving out of the bloodstream and back to the lung alveoli for expiration
A miniscule amount (0.004%) of N2O is metabolized in the gastrointestinal tract by anaerobic Pseudomonas bacteria
Physical and cognitive recovery is facilitated with administration of 100% O2 for a minimum of 5 minutes after termination of nitrous oxide
When N2O is turned off, nitrous oxide molecules diffuse rapidly from the brain back into the bloodstream
The molecules diffuse into the pulmonary arteries and across the lung alveoli
This rapid diffusion of N2O molecules and lowering of oxygen in the lungs can theoretically cause “diffusion hypoxia”
Diffusion hypoxia can be avoided by administering 100% oxygen to the patient for a period of 5 minutes
The sedative effects of the onset of action with N2O/O2 sedation
are usually seen within the first ___ minutes.
A. 5
B. 15
C. 30
D. 60
Each of the following is considered an anxiolytic effect of
N2O/O2 sedation except one. Which one is the exception?
A. Calm
B. Relaxed
C. Stressed
D. Comfortable
A, C
Review Pt’s medical history
prior to decision to use nitrous oxide
1. Allergies and previous allergies or adverse drug reactions
2. Current medications including dose, time, route and site of administration
3. Diseases, disorders, or physical abnormalities and pregnancy status
4. Previous hospitalization to include the date and purpose
If the patient is less than 18 years of age or has a guardian you should gain permission from the parent or guardian before administering nitrous oxide
Update the patient’s health history before each appointment
ASA Physical status classification system
ASA I: Normal, healthy patient. Non-smoker, minimal use of alcohol. Able to tolerate mildphysical exertion. No organic, physiologic, biochemical or psychiatric disturbances.
ASA II: Mild systemic disease without substantive physical limitations. Examples: current smoker; alcohol user; pregnant; obese (BMI<40); well-controlled diabetes,hypertension; or mild lung disease. Systemic diseases cause no significant compromise of normal activity.
ASA III: Severe systemic disease with substantive functional limitations. Examples: poorly-controlled diabetes or hypertension; COPD; Obesity (BMI>40); active hepatitis;alcohol dependence or abuse; implanted pacemaker; moderate reduction of ejection fraction; end-stage renal disease (ERSD) undergoing regular dialysis; prematureinfant (<60 weeks); history (<3 months) of MI, TIA or CVA; coronary artery disease (CAD)/stents.
ASA IV: Severe systemic disease that is a constant threat to life. Examples: Recent (<3months) MI, TIA, CVA, or CAD (stents); ongoing cardiac ischemia or severe valve dysfunction; severe reduction of ejection fraction; sepsis; disseminate intravascular coagulation; ERSD or advanced renal disease (ARD) not undergoing regularly scheduled dialysis.
ASA V: Moribund patient not expected to survive without an operation. Examples: rupturedabdominal/thoracic aneurysm, massive trauma; intracranial bleed with mass effect;ischemic bowel with significant cardiac pathology or multiple organ/systemdysfunction.
ASA VI: Declared brain-dead patient whose organs are being removed for donor purposes
E: Patient requires emergency procedure such that a delay in treatment would lead to asignificant increase in threat to life or body part
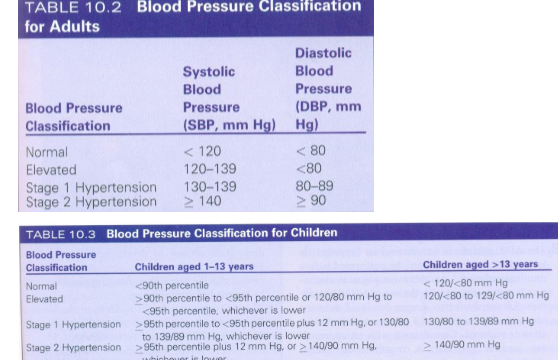
Blood pressure
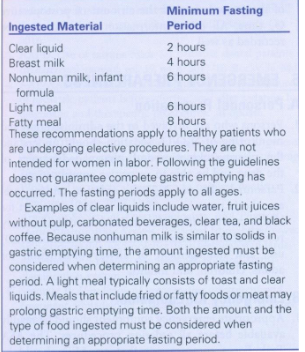
American society of anesthesiologists fasting guidelines
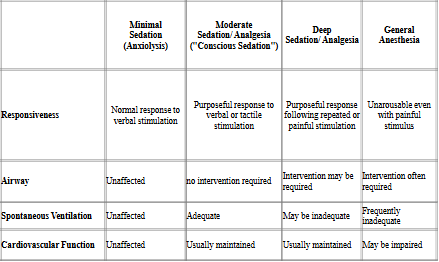
American Association of anesthesiologists levels of sedation (physical status)
Levels of nitrous oxide analgesia
1. Plane 1: relative
2. Plane 2: relative
3. Plane 3: Total (vomiting common)
Plane 1: minimal sedation
-this is the level of analgesia used in dentistry
-minimally depressed level of consciousness
-patient independently and continuously maintains an airway
-patient responds appropriately to requests made by
doctor
Total adult inspiratory capacity = Tidal volume (500 mL) + Inspiratory reserve (3100 mL) = 3600 mL (3.6 L)
Capacity of Reservoir Bag on N2O O2 machine= 3000 mL(3 L)
Pharmacokinetic properties
Oxygen makes up 21% of the earth’s atmosphere
The human body is 61% oxygen
N2O is heavier than air
Pharmacokinetic Properties
Nitrous oxide expresses its action on the body by moving across partial pressure gradients (moves from a higher to a lower pressure gradient)
The interaction between the drug, the brain and other tissues until equilibrium is reached is expressed in values called “Partition Coefficients”
The difference between the partial pressures of a gas (N2O) and a liquid (blood) indicates how quickly the drug crosses the pulmonary membrane and enters the bloodstream
N20 is a relatively insoluble drug with a blood-gas partition coefficient of 0.47 which means that equilibrium is achieved fast and it crosses the blood-brain barrier rapidly (clinical onset rapid)
N2O does not combine with any blood elements and is not stored in the body; it is eliminated from the body primarily through the lungs
The O2 component does not dissociate from N2O so it is not available for use in the body
Second-gas effect
Because high concentrations of N2O promote the rapid uptake of the gas, there is a simultaneous effect occurring when other gases are administered
This means that a second gas administered can be drawn in much faster than it would be if given alone
This second gas effect is the reason that N20 is often used during induction of general anesthesia
High altitudes effect
Due to the barometric pressure change at high altitudes require an increase in N2O concentrations to obtain the same sedative effects achieved at sea level
Pharmacodynamics
Nitrous oxide is the least potent of all inhalation general anesthetic agents
The MAC (Minimum Alveolar Concentration) of N2O is 104 – 105% which means that at normal atmospheric pressure it cannot produce profound surgical anesthesia
This limited potency and MAC value add to its safety
Which of the following represents a blood pressure value that is classified as elevated?
A. 116/76
B. 126/78
C. 140/90
D. 160/100
According to the SAS Physical Status Classification System, a 52 year old patient with hypertension being controlled by daily medication would be classified as an ____.
A. ASA I
B. ASA II
C. ASA III
D. ASA IV
Nitrous oxide is ______ than air.
A. Lighter
B. Heavier
N2O is eliminated from the body primarily through the ______.
A. liver
B. Skin
C. lungs
D. Kidneys
N20 is often used during induction of general anesthesia because it promotes the rapid uptake of more potent general anesthesia agents. This property is called ______.
A. the concentration effect
B. diffusion hypoxia
C. respiratory depression
D. the second-gas effect
B, B, B, C, D
Indications for use of nitrous oxide/oxygen for analgesia/anxiolysis
1. fearful, anxious or obstreperous (resisting control) patient
2. certain mentally, physically or medically compromised patients
3. Patient whose gag reflex interferes with dental care
4. Patient for whom profound local anesthesia cannot be obtained
5. Cooperative child undergoing a lengthy dental procedure
AAPD guidelines
Children who are ASA I or II are appropriate for all levels of sedation
For children who are ASA III or IV or who have special needs or abnormal airways a medical consult should occur before administering nitrous oxide
A responsible adult should accompany the child patient to and from the appointment
Practitioner must be able to manage all emergency and rescue situations
Informed consent must be obtained from the accompanying adult each time nitrous oxide is administered to a child
Ingestion of no heavy or fried food for 6 hours and no liquids for 2 hours prior to the procedure
Induction of nitrous oxide
Appropriate minute volume ranges between 4 – 5 L/minute for children and 6 – 7 L/minute for adolescents
The initial oxygen flow rate for a child 3 – 5 years of age should be set at 3 – 5 L/minute
AAPD recommends titration of nitrous oxide in 10% intervals
Rapid induction is a technique used in pediatric dentistry in which a high concentration of nitrous oxide is administered at the outset to calm a mildly uncooperative child
Monitoring requirements for minimal sedation (<50% N2O) include observation and assessment of the level of sedation
Recovery
Deliver 100% O2 for 5 minutes after treatment is completed
Patient should demonstrate the ability to talk, sit up and is feeling normal
Patient should be discharged to an appropriate, responsible person
Documentation should include the indication for the used of nitrous oxide sedation, the dosage and flow rate, duration of the procedure, and post-operative oxygenation time
The initial flow of oxygen for a child 3 – 5 years of age should begin between ____ L/minute.
A. 0.1 – 2.0
B. 3.0 – 5.0
C. 5.0 – 7.0
D. 7.0 – 9.0
Informed consent must be obtained from a child’s parent/guardian each time nitrous oxide sedation is administered.
A. True
B. False
The titration method of nitrous oxide administration where a high concentration of nitrous oxide is given at the outset is called ______.
A. behavioral command
B. pharmacologic restraint
C. rapid induction
D. total control
B, A, C
Infection control
1) Place plastic barriers over the N2O O2 machine
2) Keep the machine behind the patient during the procedure to minimize its exposure to aerosols
3) Sterilize or dispose of nasal hood after use
Cover the delivery unit with a protective barrier

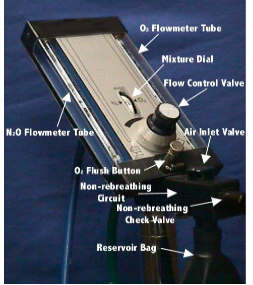
Components of a continuous flow nitrous oxide-oxygen machine
(continuous flow means a constant flow of gases is provided regardless of the patient’s breathing pattern)
1. Gas cylinder and gauges
2. Reducing valves (regulators)
3. Flowmeters and mixers
4. Reservoir bag
5. Conducting tubing
6. Nasal hood
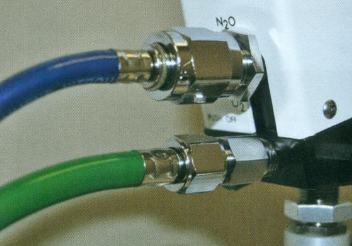
Nitrous oxide tank = blue Oxygen tank = green; FDA
A full “E” size cylinder of oxygen contains 660 L of O2 under a pressure of 2100 psi
A full “E” size cylinder of N2O contains 1600 L of N2O gas under pressure of 750 psi
A full N2O tank contains 95% liquid N2O and 5% N2O gas
A typical N2O tank will register “full” until more than 75% of the liquid has been depleted
After the liquid has been depleted the gauge will register the amount of N2O gas that is left in the tank
Clinical usage
On average, 2.5 tanks of oxygen are used for every 1 tank of nitrous oxide
Connecting tubes connect O2 and N2O tanks to the machine
Reducing valves (regulators)
Located within the regulator mechanism to reduce the high pressure in the tanks (750 psi or 2100 psi) to a pressure that the conducting tubing and the lungs can handle (50 psi)
As the pressure is reduced, there is a momentary increase in pressure that can ignite any grease or oil that is on the valves and cause a catastrophic explosion (tank valve wrenches should remain with machine)
Nitrous Oxide Press pressure regulator
Nitrous oxide and oxygen pressure gauges
indicating content of gas in each cylinder

Safety feature pin index safety system
prevent improper attachment of oxygen and nitrous oxide tanks

Hydrocarbons such as oil or grease should not be used near valves, gauges, regulators or any fittings on the nitrous oxide/oxygen delivery system because they may cause ______.
A. leaking of the gas cylinder
B. malfunctioning of the regulator
C. a catastrophic explosion
D. rusting inside the gauges
Which of the following statement is true?
A. The color of the oxygen tank is green, the color of the
nitrous oxide tank is blue
B. The color of the oxygen tank is blue, the color of the nitrous
oxide tank is green
C, A
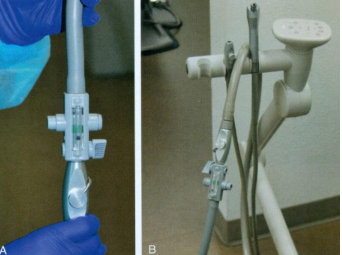
Conduction tubing
Engage the delivery unit to the high volume evacuation system
Administration of N2O/O2
Obtain a blood pressure reading and pulse rate before administering N2O/O2
Begin with placing the patient in a comfortable position (upper torso slightly reclined and legs slightly elevated)
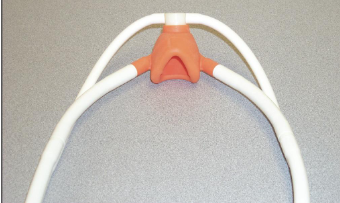
Secure the nasal hood on the patient
Selection of an appropriately-sized nasal hood should be made
Nasal hoods are made of silcone or rubber latex and should adapt to the face to provide an airtight seal
Instruct patient to breathe through their nose and to keep lips sealed
Nasal hoods should be sterilizable or disposable
Small inner mask receives anesthetic gas from machine
Larger outer mask connected to high volume evacuator to remove exhaled gases
Open the oxygen and nitrous oxide tanks by turning the valve on top of the cylinders counterclockwise with the dedicated wrench that comes with the stand
Begin procedure with administration of 100% oxygen
Display volume of gas/minute passing through connecting tube controlled by a mixing valve
Not an accurate measure of the gas the patient is actually inspiring
flow rate of 5 to 6 liters/minute generally is acceptable to most patients
flow rate can be adjusted after observation of the reservoir bag
continual clinical observation of the patient's responsiveness, color, and respiratory rate and rhythm must be performed
Patient should not be left unattended at any time during the administration of nitrous oxide analgesic

Titration
process of administering a drug incrementally to a specific level of sedation
is a safety feature the chances of an unintentional overdose
minimizes the possibility of a severe, life-threatening reaction
No allergic reactions have ever been reported to N2O
Because of the principle of biovariability, patients may require different levels of N2O on different days and different procedures
A patient who does not show any signs or symptoms of sedation when administered N2O is considered hyporesponsive
Concentrations of N2O delivered may vary during a procedure
If a patient indicates that they are becoming uncomfortable with the level of sedation, reduce the concentration of N20 being administered
When administration of N2O is terminated, the patient should be delivered 100% O2 for a minimum of 5 minutes
Calculating % Gas
4 L O2+ 2 L N2O
Total delivery = 6 L
2 L N2O / 6 L Total = 33% N20
4 L O2 / 6 L Total = 67% O2
3 L O2+ 3 L N2O
Total delivery = 6 L
3 L N2O / 6 L Total = 50% N20
3 L O2 / 6 L Total = 50% O2
Reservoir bag
3 L rubber or silicone bag
Provides reserve gas when patient’s respiratory demands exceed the flow of the machine
Serves also to monitor patient’s respiration
Bag is attached to oxygen flush for emergencies
Increase gas flow by pressing the O2 flush button if the reservoir bag collapses
Reduce gas flow to reservoir bag if it is bulging
Introduction of 100% oxygen for 1 to 2 minutes followed by titration of nitrous oxide in 10% intervals is recommended

Constant oxygen flow technique
1) Set O2 flow at a constant rate
2) Add N2O in increasing increments
3) O2 flow rate is kept constant throughout
Constant liter flow technique (titration)
1) Set O2 flow rate
2) Increase N2O flow rate .5 L / minute
Decrease O2 flow rate .5 L / minute
3) Continue to titrate the levels of O2 and N2O until desired level of gases are achieved
During treatment, it is important to continue the visual monitoring of the patient's respiratory rate and level of consciousness

The concept of biovariability when administering drugs is based on the premise that __________.
A. the majority of people react the same way to the same drug
B. individuals may not react similarly to the same drug on different days
C. individuals are likely to require the same amount of a drug when prescribed at different times
D. all people will react the same to a drug regardless of the dose
The patient who does not show any signs of sedation when
administered nitrous oxide is considered to be _______.
A. hyporesponsive
B. hyperresponsive
As you begin nitrous oxide/oxygen administration, you notice that as the patient inhales, the reservoir bag collapses. What should you do next?
A. Ask the patient to take deeper respirations
B. Ask the patient to take shallower respirations
C. Increase the flow of oxygen to the patient
D. Decrease the flow of oxygen to the patient
As you begin nitrous oxide/oxygen administration, you notice that as the patient inhales, the reservoir bag is bulging? What should you do next?
A. Ask the patient to take deeper respirations
B. Ask the patient to take shallower respirations
C. Increase the flow of oxygen to the patient
D. Decrease the flow of oxygen to the patient
B, A, C, D
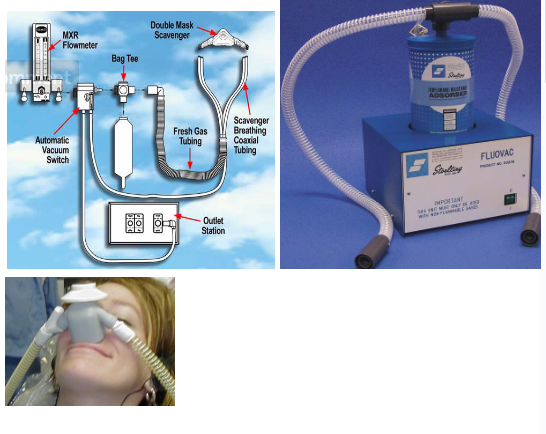
Nitrous oxide scavenging unit
exposure to ambient nitrous oxide be minimized through use of effective scavenging systems and periodic evaluation and maintenance of the delivery and scavenging systems
The major source of trace N2O that contaminates the ambient air in the dental office is caused by patients talking when nitrous oxide is being administered
Nitrous oxide scavenging unit controls N2O ambient air levels
Once the nitrous oxide flow is terminated, 100% oxygen should be delivered for 5 minutes
The patient must return to pre-treatment responsiveness before discharge
Checking
All newly installed facilities for delivering nitrous oxide/oxygen must be checked for proper gas delivery and fail-safe function prior to use
Manufacturers recommend that routine maintenance be performed on the flowmeter every 2 years
Children
Inhalation equipment must have the capacity for delivering 100%, and never less than 30%, oxygen concentration at a flow rate appropriate to the child's size, and must have a fail-safe system that is checked and calibrated regularly according to the practitioner's state laws and regulations
If nitrous oxide/oxygen delivery equipment capable of delivering more than 70% nitrous oxide and less than 30% oxygen is used, an in-line oxygen analyzer must be used
Manufacturers recommend that routine maintenance be performed on the delivery system flowmeter every ___ years.
A. 2
B. 5
C. 8
D. 10
The major source of trace nitrous oxide that contaminates the ambient air is a dental office is from ________.
A. cracked reservoir bags
B. leaking valve stems on the cylinder
C. the patient talking
D. improperly soldered central piping
A, C
Assessing adequate recovery
Patient should be alert and oriented before being dismissed
If the patient indicates they are still feeling dizzy after 100% oxygen administration, administer oxygen for a additional 5 minutes
Vital signs should be stable
Document adequate recovery in patient’s char
Postop procedures
Turn off the gas cylinders on the portable unit immediately after use
Central system cylinders are usually turned off at the end of the day
Bleed the lines on the portable unit at the end of the day to purge gas left in the lines
Which of the following is the appropriate procedure to follow when a patient indicates that they are still dizzy following administration of 100% oxygen for 5 minutes?
A. Direct the patient to wait in the reception area for 15 minutes
B. Contact an adult to accompany the patient from the office
C. Administer 100% O2 for an additional 5 minutes
D. Dismiss the patient and document that the patient should not receive nitrous oxide sedation at the next visit
Which of the following would indicate that the patient has not adequately recovered from nitrous oxide sedation?
A. After receiving 5 minutes of O2, the patient is feeling normal
B. Postoperative vital signs are within close range of preoperative values
C. Patient indicates an altered sense of time taken for the procedure
D. Patient indicates a “groggy, lethargic” feeling
C, D
Monitoring nitrous oxide
1) Check O2 and N2O gauges prior to use
2) Insure scavenging system is working
3) Insure flowmeter is working
4) Insure fail-safe mechanism is working so that no less than
30% oxygen can be delivered to the patient
5) Review patient’s medical history
6) Initiate patient on 100% O2
7) Fit nasal hood snugly to patient’s face
8) Turn on scavenger system (HVE)
9) Initiate N2O flow at 25-30% for adults
10) Monitor patients vital signs throughout the procedure
11) Once procedure is finished, return flowmeter to 100% O2 for 5 minutes before nasal hood is removed
Informed consent must be obtained from the parent and documented in the patient's record prior to administration of nitrous oxide/oxygen
Patient's record must include indication for use of nitrous oxide/oxygen inhalation, nitrous oxide dosage
Patient record
1) Patient received ___ % N2O - ___ % O2 at a total flow
rate of ___ L / minute for approximately ___ minutes
2) At termination of the procedure the patient received
100% O2 for ___ minutes at a flow rate of ___ L / minute
3) Patient tolerated the procedure well and was dismissed
from the office in good condition
4) Vital signs (blood pressure, pulse, respirations) should be
recorded for before, during and after the procedure
It is acceptable to leave the patient alone while administering
nitrous oxide/oxygen sedation.
A. True
B. False
The purpose of the O2 flush button is to _____.
A. fill the reservoir bag when necessary
B. substitute for CPR in an emergency situation
C. flush the patient with O2 at the end of the procedure
D. monitor the patient’s respiration
False, A
Safety features of nitrous oxide
1) Color coding of tanks
2) Tanks are labelled O2 and N2O
3) Pin index system between the tanks and the machine yoke prevents attaching the wrong tank to the machine
4) Fail safe feature disallows <30% O2 and automatically shuts off the N2O tank if the O2 tank is empty
5) Oxygen is initiated at 2-3 L/minute automatically
6) Audible alarm sounds if O2 tank is depleted
7) Connecting tubing for O2 tank will not fit the connecting tubing for the N2O tank
8) O2 flush button used to deliver a large volume of O2 if an emergency occurs
Storage of nitrous oxide and oxygen
Cylinders should be stored away from the operatory
No grease, oil or any other organic substance should come in contact with any gas or gas delivery equipment
Cylinders should not be subjected to extreme temperatures
Cylinders must be inspected on a regular basis
Cylinders should be secured and stored in a location that is not readily accessible or visible to others
Adverse effects of nitrous oxide/oxygen inhalation
1. Most common adverse effect- 1-10 % of patients experience nausea and vomiting
2. Fasting is not required for patients undergoing nitrous oxide analgesia, however recommend only a light meal be consumed in the 2 hours prior to the administration of nitrous oxide
3. Evidence that diffusion hypoxia can occur as a result of rapid release of nitrous oxide from the blood stream into the alveoli diluting the concentration of oxygen is disputed. This may lead to headache and disorientation and can be avoided by administering 100% oxygen for 5 minutes after nitrous oxide has been discontinued
Combining nitrous oxide sedation with other methods
Problems with nitrous oxide sedation usually occur when in is administered with oral medications:
1) Benzodiazepines (diazepam, midazolam, halcion)
2) Opioids (Meperdine, Oxycodone)
3) Chloral hydrate
4) Antihistamines (hydroxyzine)
*Any additional drug, other than a local anesthetic, renders a patient in the category of moderate sedation
Treatment of oxide
1. Turn off nitrous oxide tank
2. Remove nasal hood from patient
3. Turn patient’s head away from clinician
4. If patient is cooperative, replace hood on patient’s face and administer 100% oxygen for 3-5 minutes
The dangers of nitrous oxide use and abuse
1. Oxygendeprivation of the brain
2. Diffusion hypoxia (disputed)
3. Bone marrow suppression
4. Decreased fertility
5. Liverand kidney disease
6. Peripheral neuropathy
7. Mixture of N2 O / O 2 is flammable
Signs and symptoms of nitrous oxide oversedation
1) Persistent closing of mouth and rigidity in perioral area
2) Complaints about nausea or vomiting (vomiting occurs more in children)
3) Complaints of sedation becoming too intense
4) Extreme sluggishness or sleepiness
5) Agitation or uncooperativeness
6) Uncontrolled crying or laughing
Treatment of oversedation
1) ABC: Airway (maintain) Breathing (assess) Cardiac (rhythms, pulse)
2) Administer 100% oxygen at a flow rate of 10 L / minute
3) Be prepared to administer CPR
4) Naloxonehydrochloride (Narcan) can produce reversal effects of nitrous oxide sedation
The drug able to reverse the effects of nitrous oxide is
A. acetaminophen
B. naloxone hydrochloride (Narcan)
C. amoxicillin
D. lidocaine
B
BLS
Training and certification in basic life support (BLS) are required for all clinical personnel
Emergency kit
must be readily accessible; Emergency equipment must be able to accommodate children of all ages and sizes
Oxygen delivery system
positive pressure oxygen delivery system capable of administering >90% oxygen at a 10 liters/minute flow for at least 60 minutes (650 liters, "E" cylinder) must be available
Documentation
There should be documentation that all emergency equipment and drugs are checked and maintained on a regularly scheduled basis
