Circulation III: Cerebral Hemorrhages
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
What is an Intracranial Hemorrhage
Intracranial hemorrhages are rupture of blood vessels within the brain. It is subdivided into four categories based on location/compartment within the skull
→ epidural
→ subdural
→ subarachnoid
→ intraparenchymal/intracerebral
all cause death through compression of the brain and tissue destruction
What are Intraparenchymal Hemorrhages
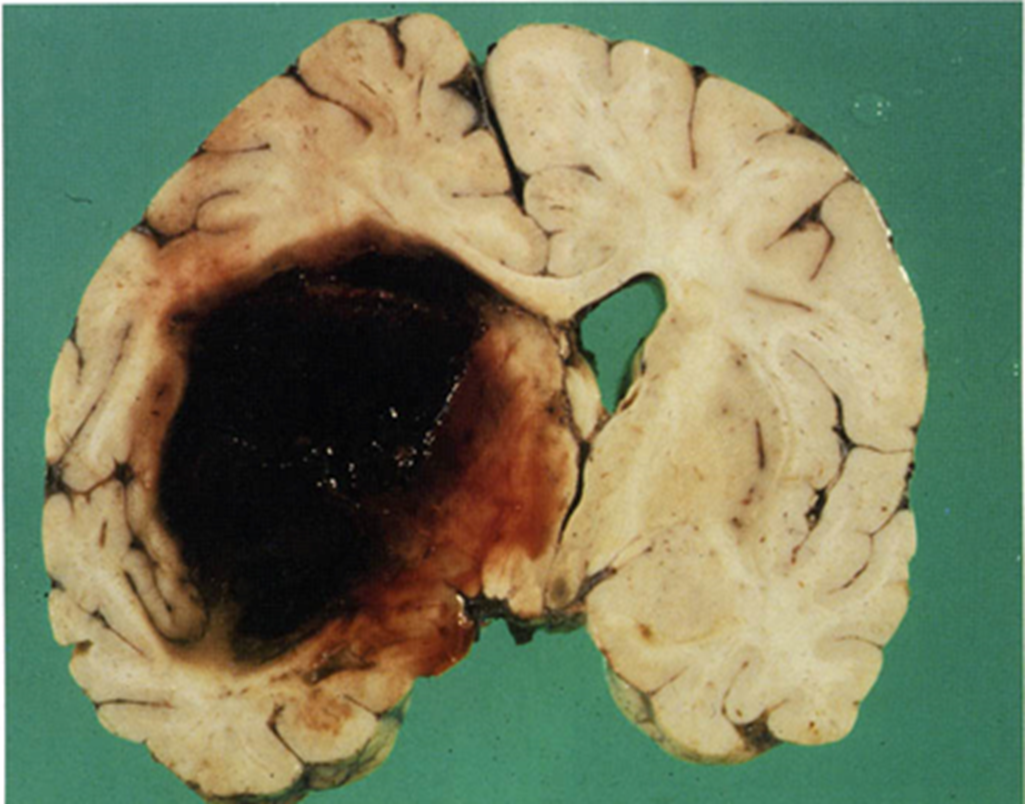
Intraparenchymal Hemorrhages result from rupture of vessels within the brain resulting in the formation of a hematoma
1) the resulting hematoma is walled off by brain tissue or it can rupture into a ventricle or subarachnoid space as an extension
→ forty percent of patients experience expansion of hematoma during the first 24 hours
What are the most common symptoms of an intraparenchymal hemorrhage
Intraparenchymal Hemorrhages typically present with focal neurologic deficits with symptoms that cause increased intracranial pressure
1) symptoms of increased intracranial pressure appear which are unlike ischemic strokes because they introduce new material into the brain
→ may cause headaches, nausea, vomiting, and diplopia
How are Intraparenchymal Hemorrhages imaged?
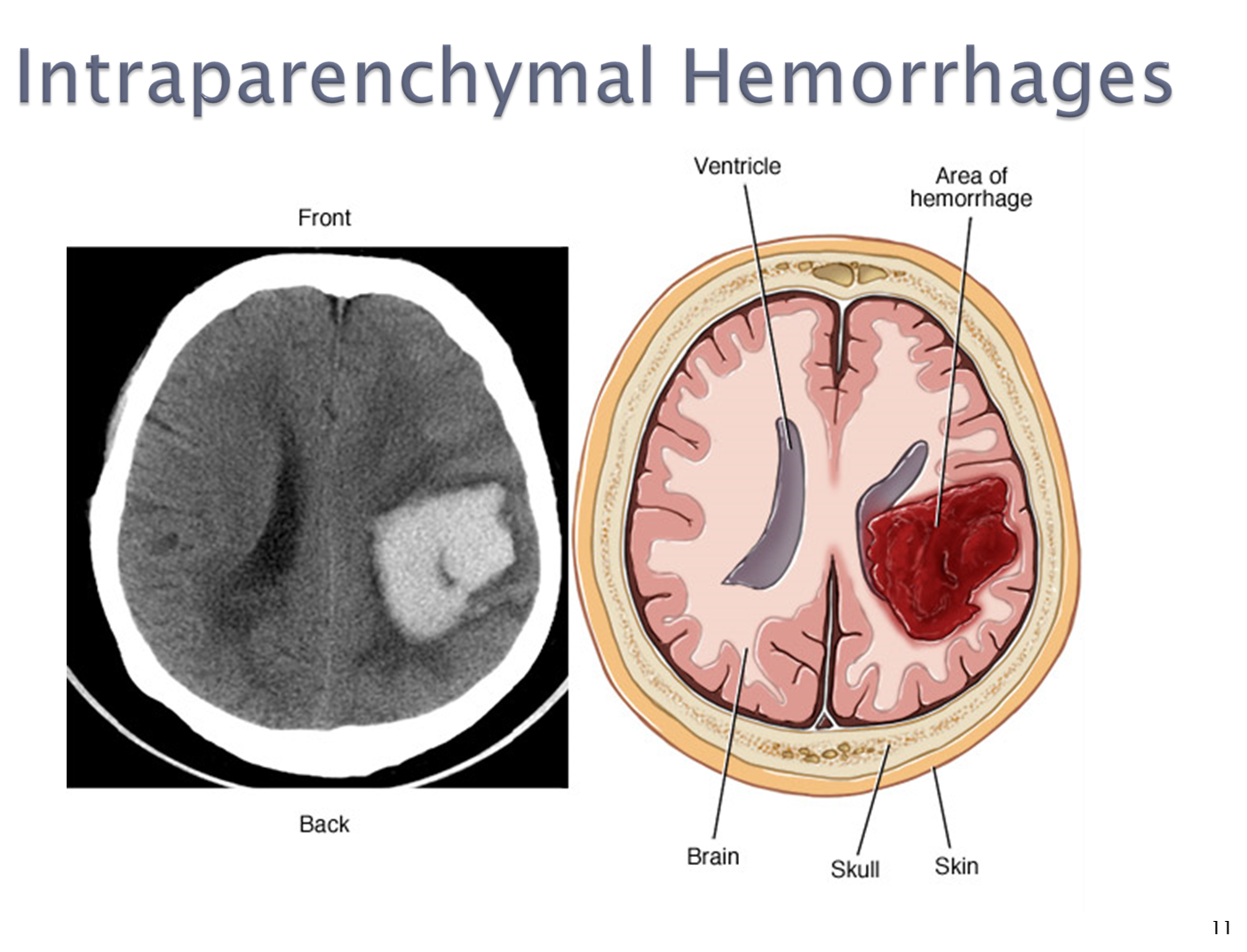
Intraparenchymal hemorrhages are best imaged using a CT scan
→ in an acute setting, blood will appear white bright in the brain
→ MRI or vascular studies may be used in order to find the underlying vascular lesions
What are Hypertensive Hemorrhages?
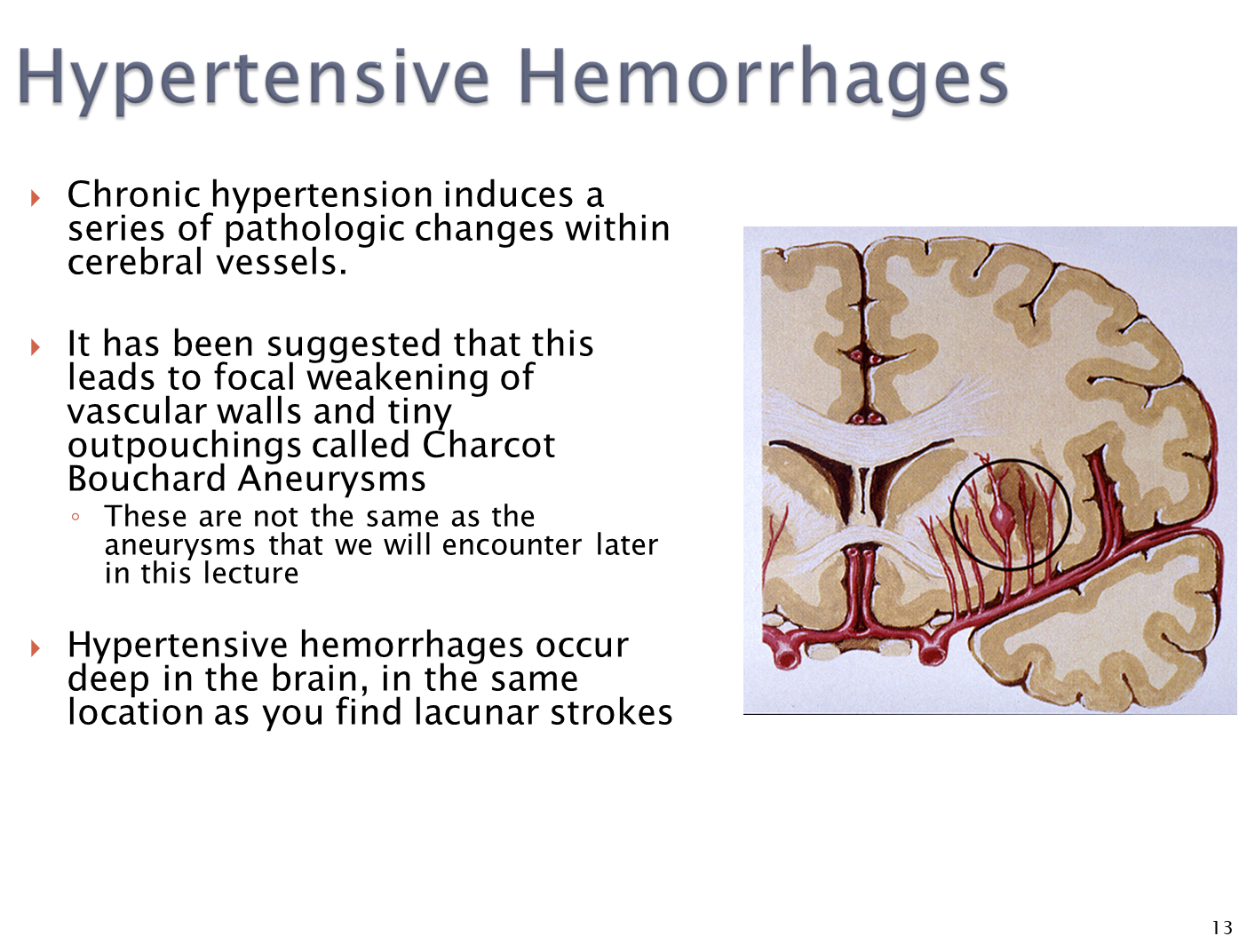
Hypertensive hemorrhages are a common cause of intraparenchymal hemorrhages where chronic hypertension causes pathological change in the cerebral vessel
1) hypertension over long periods of time leads to focal weakening of vascular walls leading to outpouchings called Charcot Bouchard Aneurysms
→ these hemorrhages will occur deeper in the brain
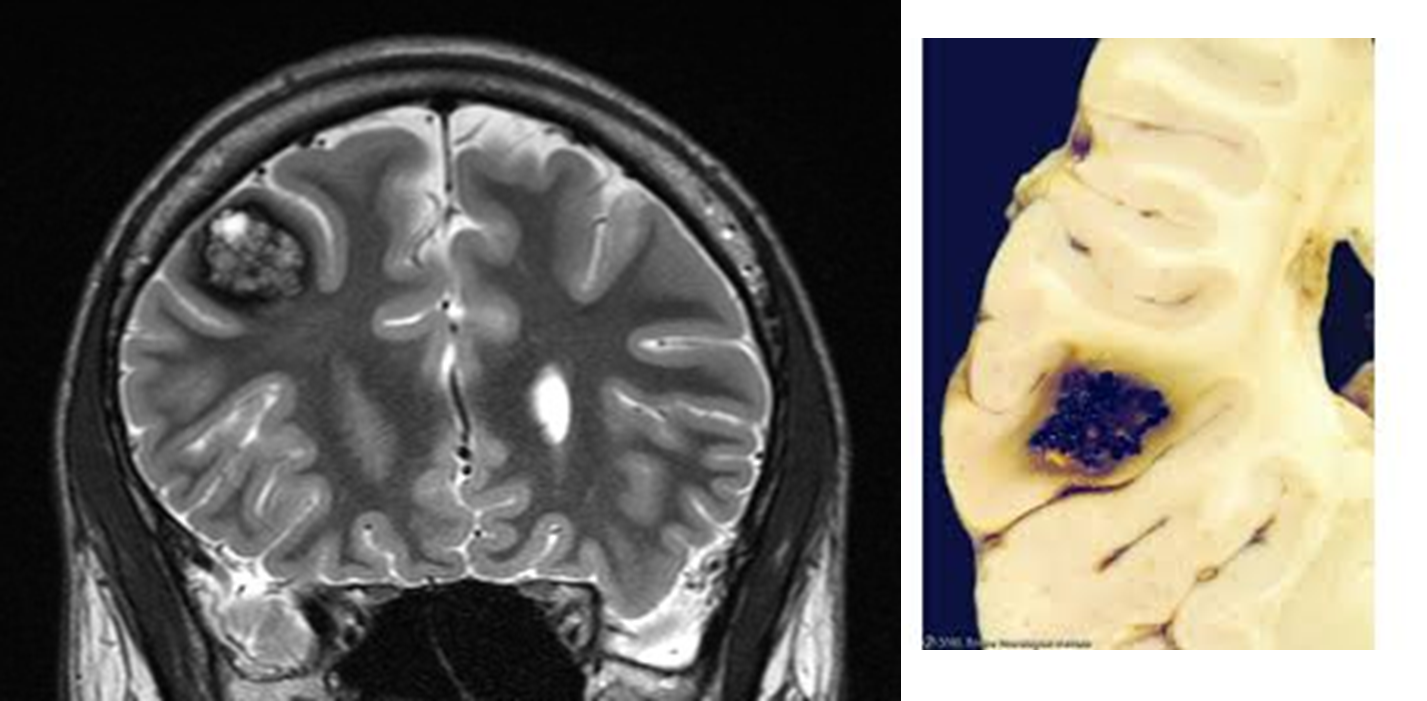
What are Arteriovenous Malformations
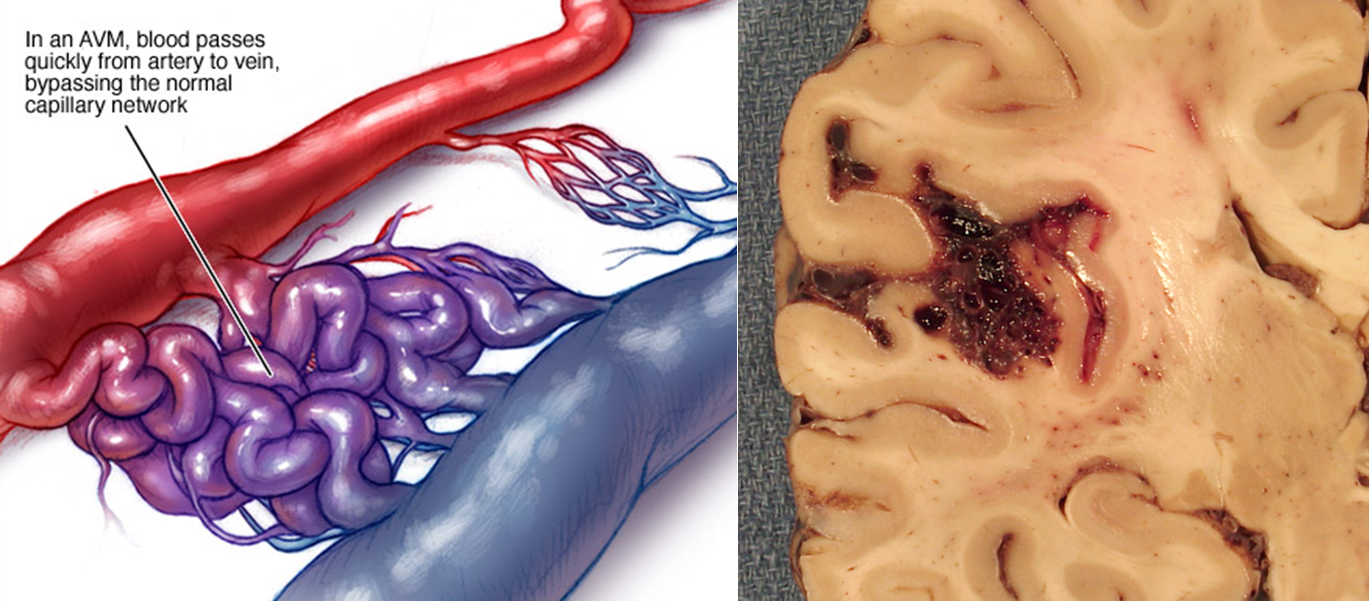
Arteriovenous malformations are congenital vascular malformations that can result in intraparenchymal hemorrhages
1) AVMs are congenital malformations where there is a direct connection between arteries and veins without a intermediate capillary bed
→ gliotic, or glial cells, are often mixed in with the vascular tissue
What are Cavernous Malformations
Cavernous malformations are a form of vascular malformation that can lead to intraparenchymal hemorrhage
1) causes tufts of dilated thin walled capillaries
→ opposed to arteriovenous malformations, there is no feeding arteries or draining veins
What is Amyloid Angiopathy?
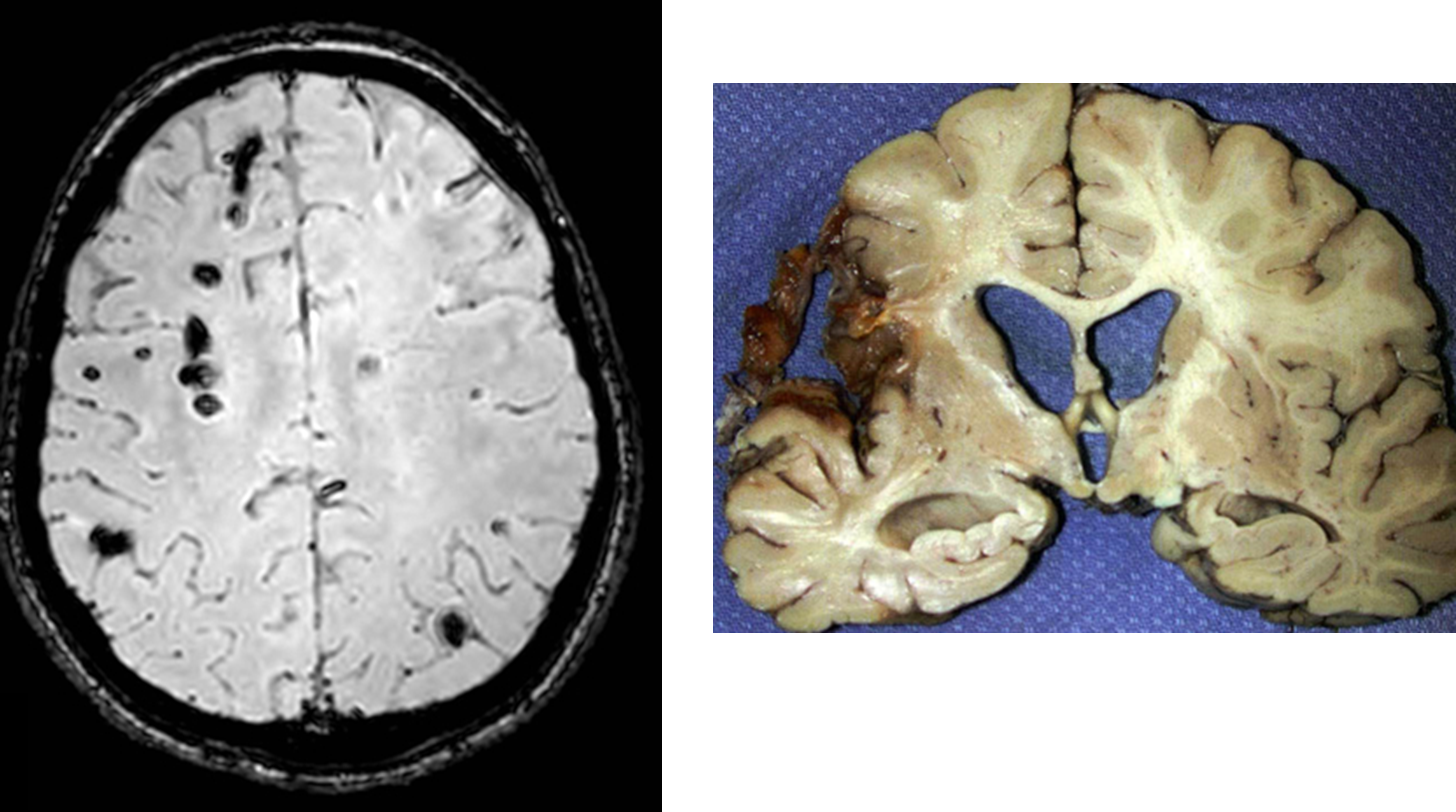
Cerebral Amyloid Angiopathy is when amyloid beta peptide deposits within small to medium sized blood vessels, often causing an intraparenchymal hemorrhage
1) May present with progressive cognitive decline and stroke like episodes
→ the peptides will weaken blood vessels causing microbleeds, which are often asymptomatic but can lead to bigger bleeds
2) These typically present superficially and are referred to as lobar hemorrhages
→ hemorrhages that are hypertensive in origin are often deeper
How is Intraparenchymal Hemorrhages treated?
1) Patients are stabilized before reducing the intracranial pressure
→ patients blood pressure is controlled and then we treat the underlying cause
2) Surgery is often not used, unless hemorrhage is surface level such as in a cerebral amyloid angiopathy
How is Non-communicating hydrocephalus treated?
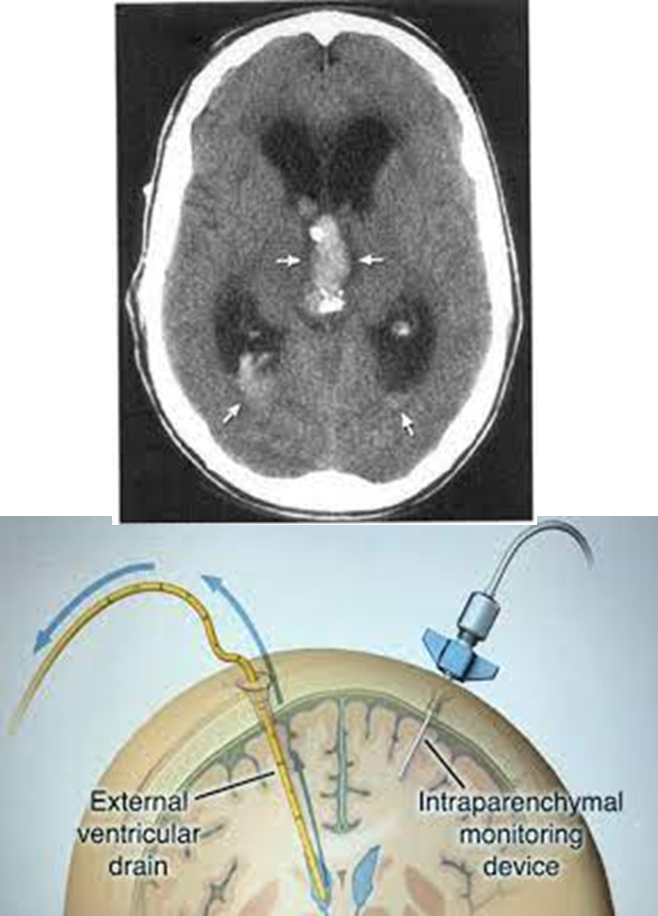
Patients with obstructive or non-communicating hydrocephalus are treated with the placement of an external ventricular drain
→ often occurs in patients with extension of hemorrhage into a ventricle
What is an Epidural Hemorrhage
Epidural hemorrhage is a bleed into the epidural space between the skull and dura, this is commonly caused by trauma to the middle meningeal artery
1) damage to the MMA usually occurs at the pterion a thin portion of bone where sutures meet
2) blood during a epidural hemorrhage will tend to accumulate quickly because it is under arterial pressure
→ patients will rapidly develop neurological problems with loss of consciousness
3) Can often lead to subfalcine or uncal herniation where the uncus herniates under the falx cerebri
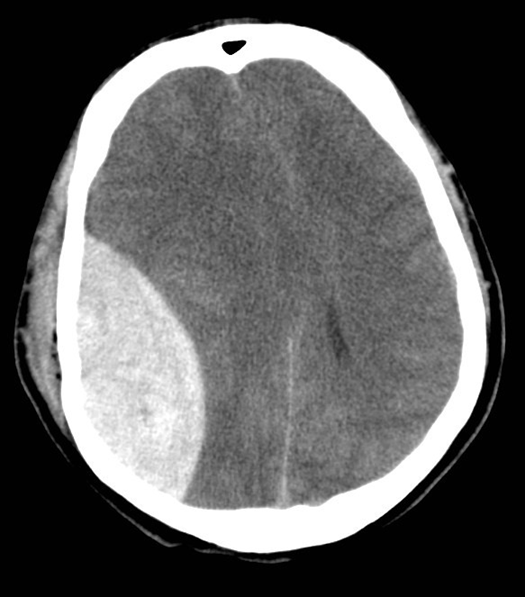
What do Epidural hemorrhages look like on CT? How is it treated if present?
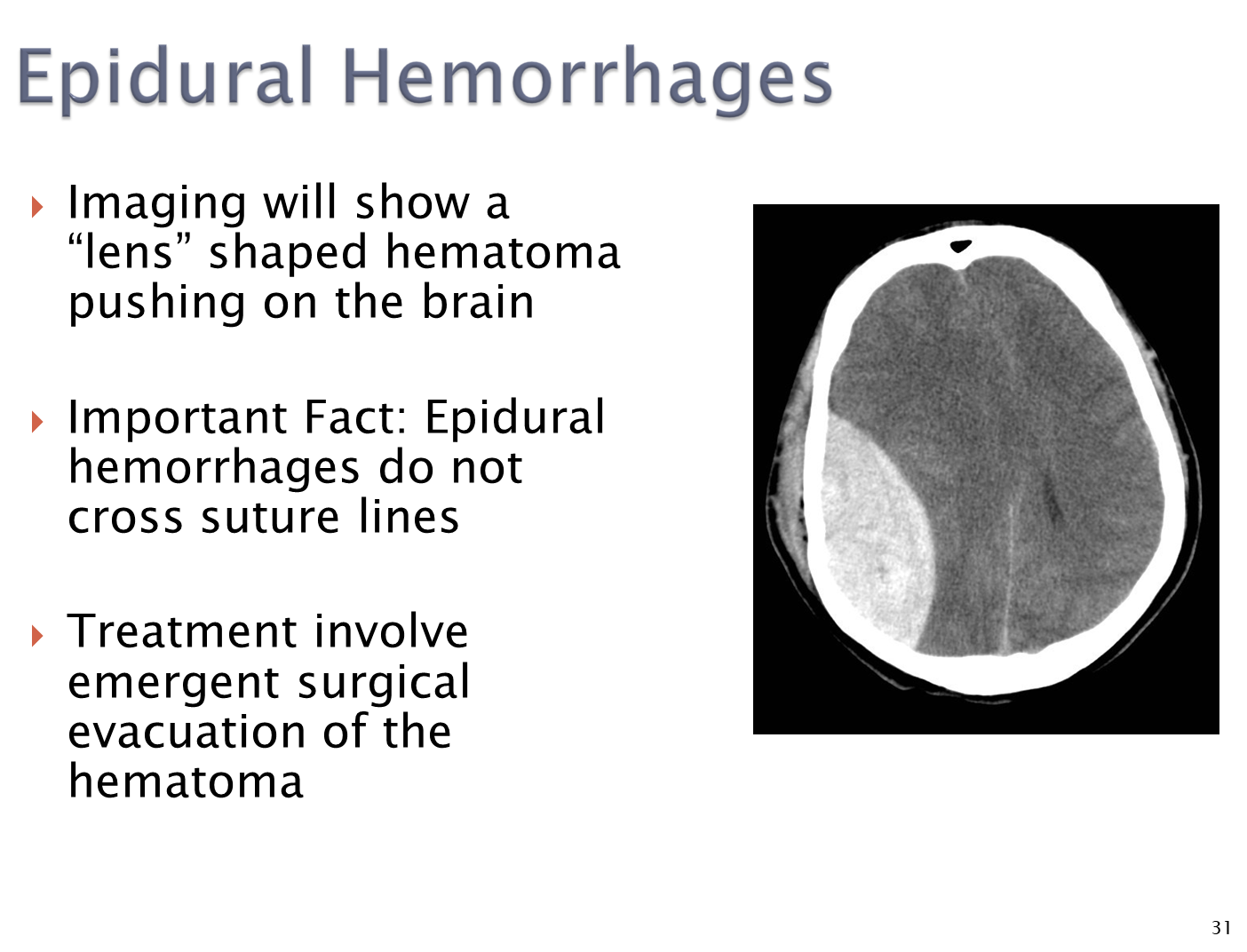
Will appear to have a large lens shaped hematoma that pushes onto the brain
→ epidural hemorrhages will not cross suture lines
→ treated with emergent evacuation of the hematoma
What are Subdural Hemorrhages
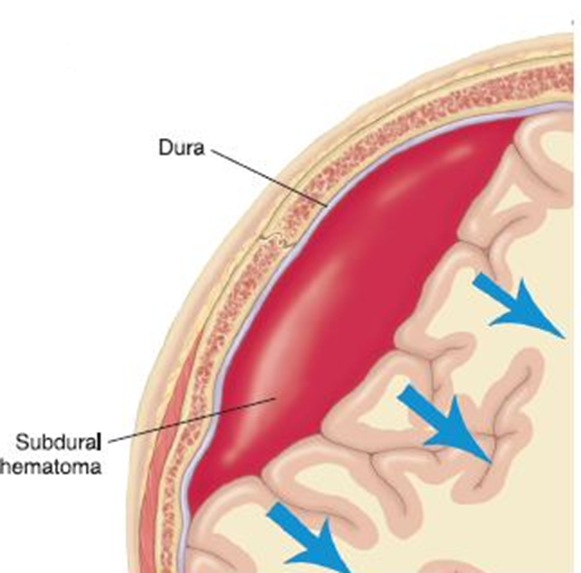
Subdural hemorrhage is a bleed into the subdural space between the dura and arachnoid layer
1) Subdural hemorrhages will occur due to laceration of bridging veins traversing the subdural space
→ patients who are older or have cerebral atrophy have friction on these veins making them susceptible to tearing
2) Bleeding is often slower because it is under venous pressure
→ may slowly enlarge over days, leading to a slower onset of symptoms than a epidural hemorrhage
How does a subdural hemorrhage present on a CT scan and how is it treated?
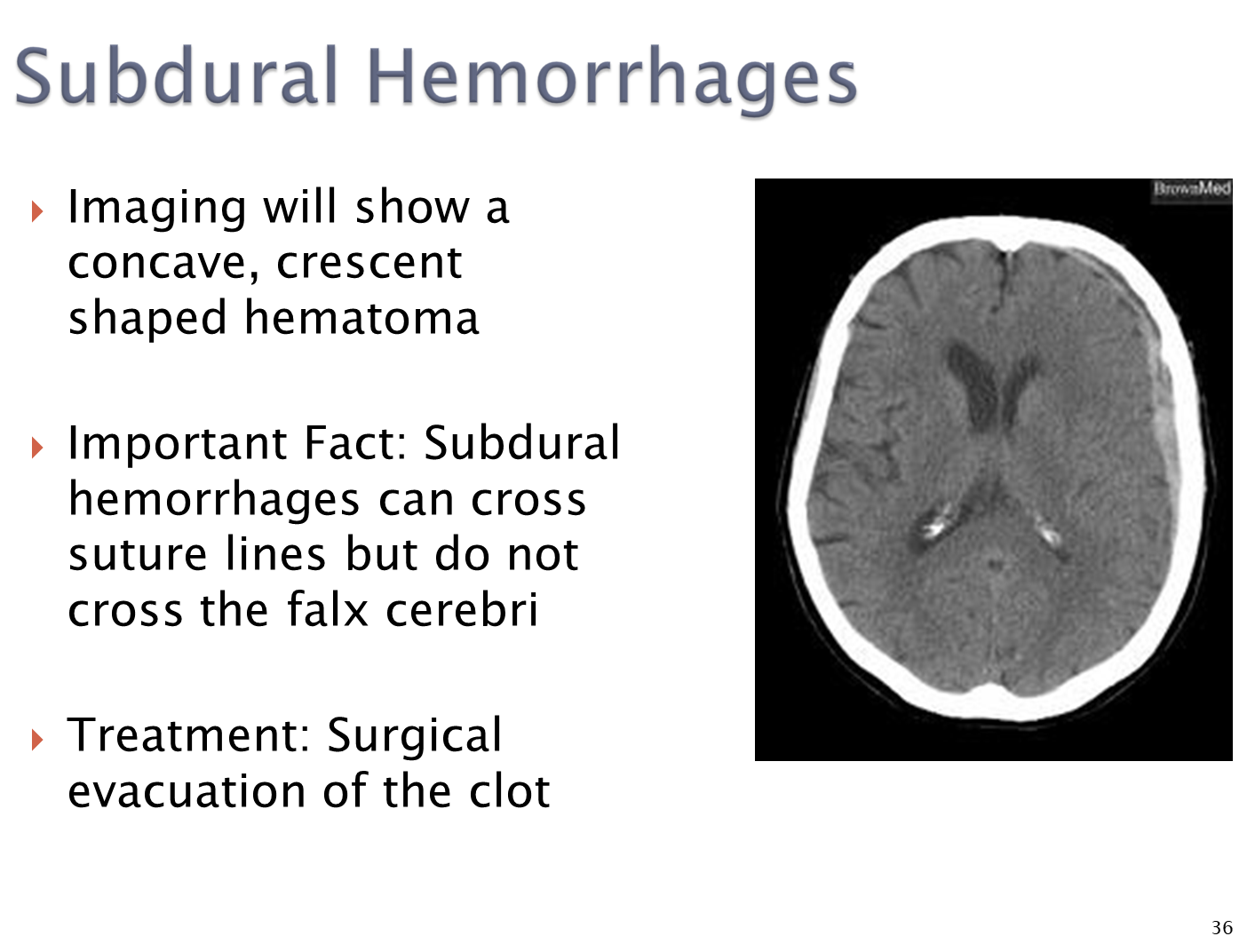
CT - concave crescent shaped hematoma
→ subdural hemorrhages can cross suture lines but will not cross the falx cerebri
→ treated with surgical removal of the clot
What are Subarachnoid Hemorrhages? What are the major risk factors
Subarachnoid hemorrhages occur when arteries rupture in the subarachnoid space typically due to trauma at the Circle of Willis
1) Patients with a history of smoking and alcohol use
→ family history of subarachnoid hemorrhages
→ hypertensive
2) Often are associated with two major diseases
→ autosomal dominant polycystic kidney disease
→ Ehlers-Danlos Syndrome
What are Saccular Aneurysms?
Saccular aneurysms or berry aneurysms are vascular lesions resulting from a focal defect in the vascular wall
1) leads to a thin or absent tunica media/internal elastic lamina of the arteries, leading to their rupture
→ a common cause of subarachnoid hemorrhages
2) These aneurysms will usually be asymptomatic until they rupture
→ often occur at bifurcations in the anterior circulation
What are the symptoms of subarachnoid hemorrhages
Subarachnoid hemorrhages will present with symptoms depending on the location of the hemorrhage
1) Anterior Communicating Artery
→ compresses the optic chiasm leading to cuts in the visual field
→ may also cause contralateral leg weakness
2) Middle Cerebral Artery
→ contralateral face and arm weakness
→ aphasia and neglect (failure to recognize a part of your body)
3) Posterior Communicating Artery
→ Cranial Nerve III Palsy
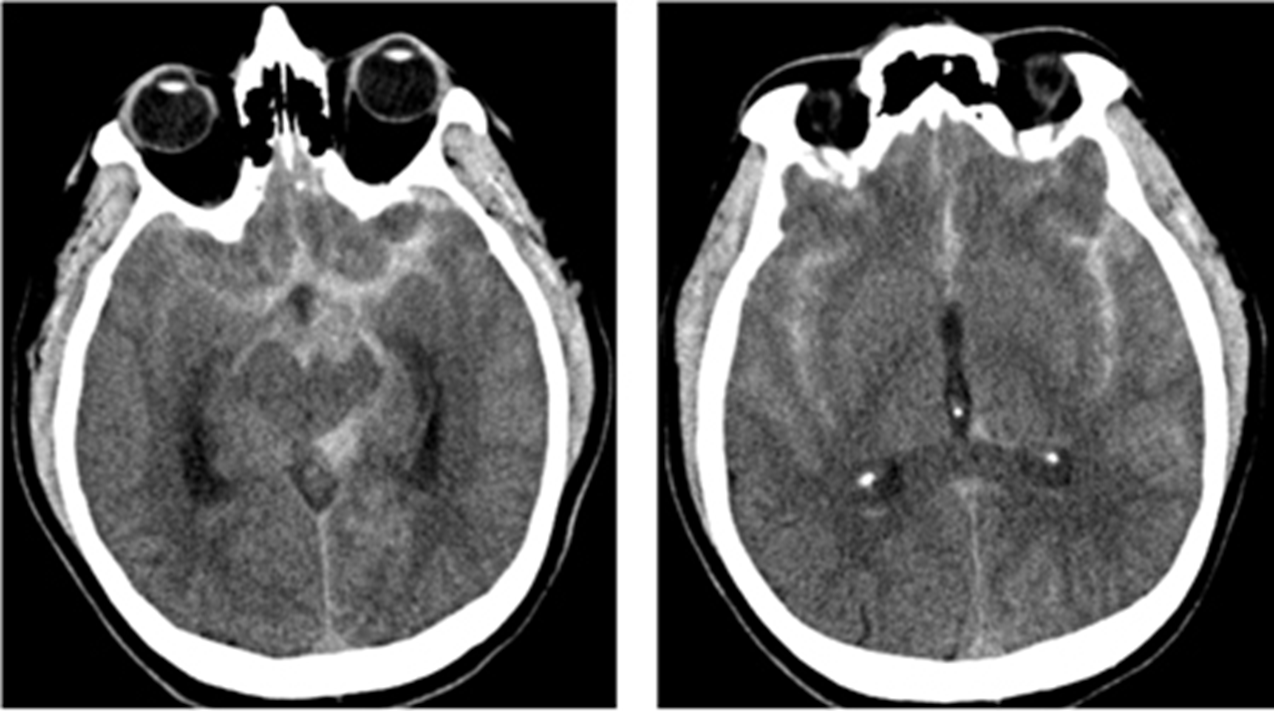
What do Subarachnoid Hemorrhages appear like on imaging? What additional tests might you do?
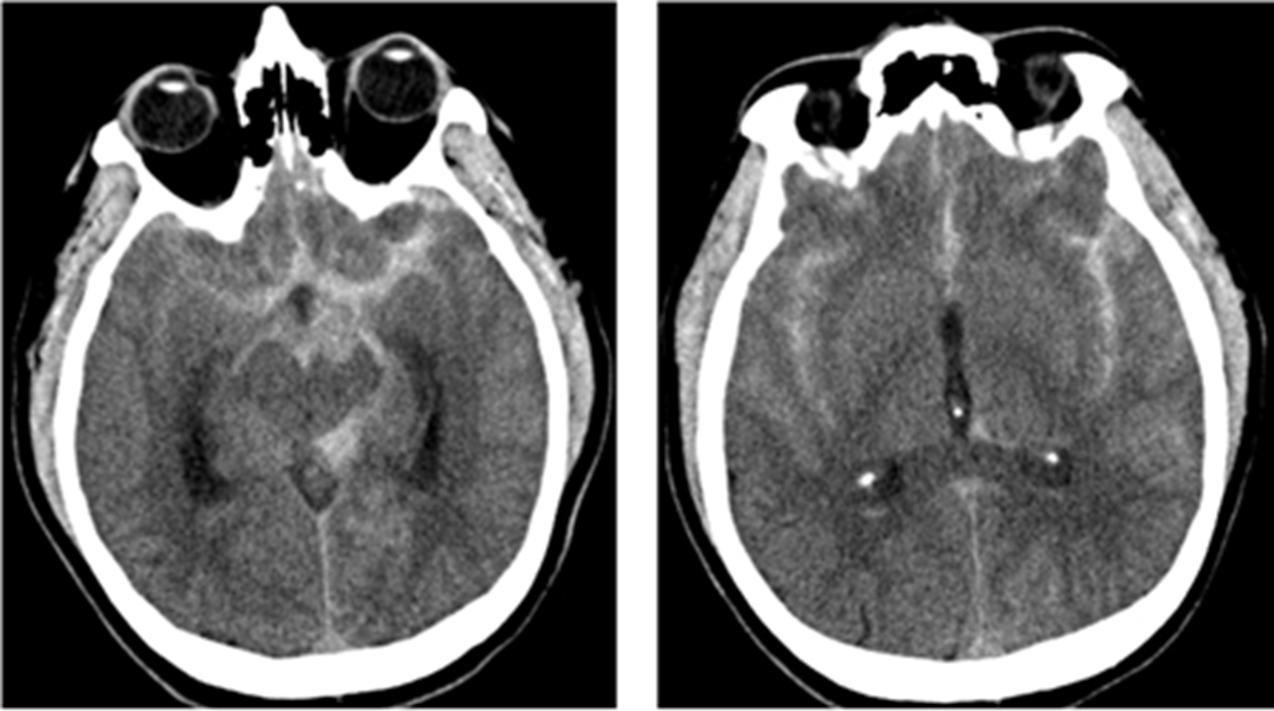
Subarachnoid hemorrhages will often present with a star sign on CT imaging
1) Star sign is where blood from subarachnoid hemorrhages tracks up in between the hemispheres of the brain, laterally between the sylvian fissure, and posteriorly to the midbrain
→ can often see blood accumulating in the sylvian fissure bilaterally
2) in patients with a negative CT but you are highly suspicious that they have a SAH, you do a lumbar puncture
→ would show elevated RBC in the CSF which do not clear in subsequent collections of CSF
→ xanthrochromia or yellowing of the CSF
3) Vascular imaging is needed to confirm the saccular/berry aneurysm
What are the four most common complications of subarachnoid hemorrhage
Rebleeding
Hydrocephalus
Seizures
Vasospasm (sudden narrowing of vessel) leading to infarction
What is the Glasgow Coma Scale?
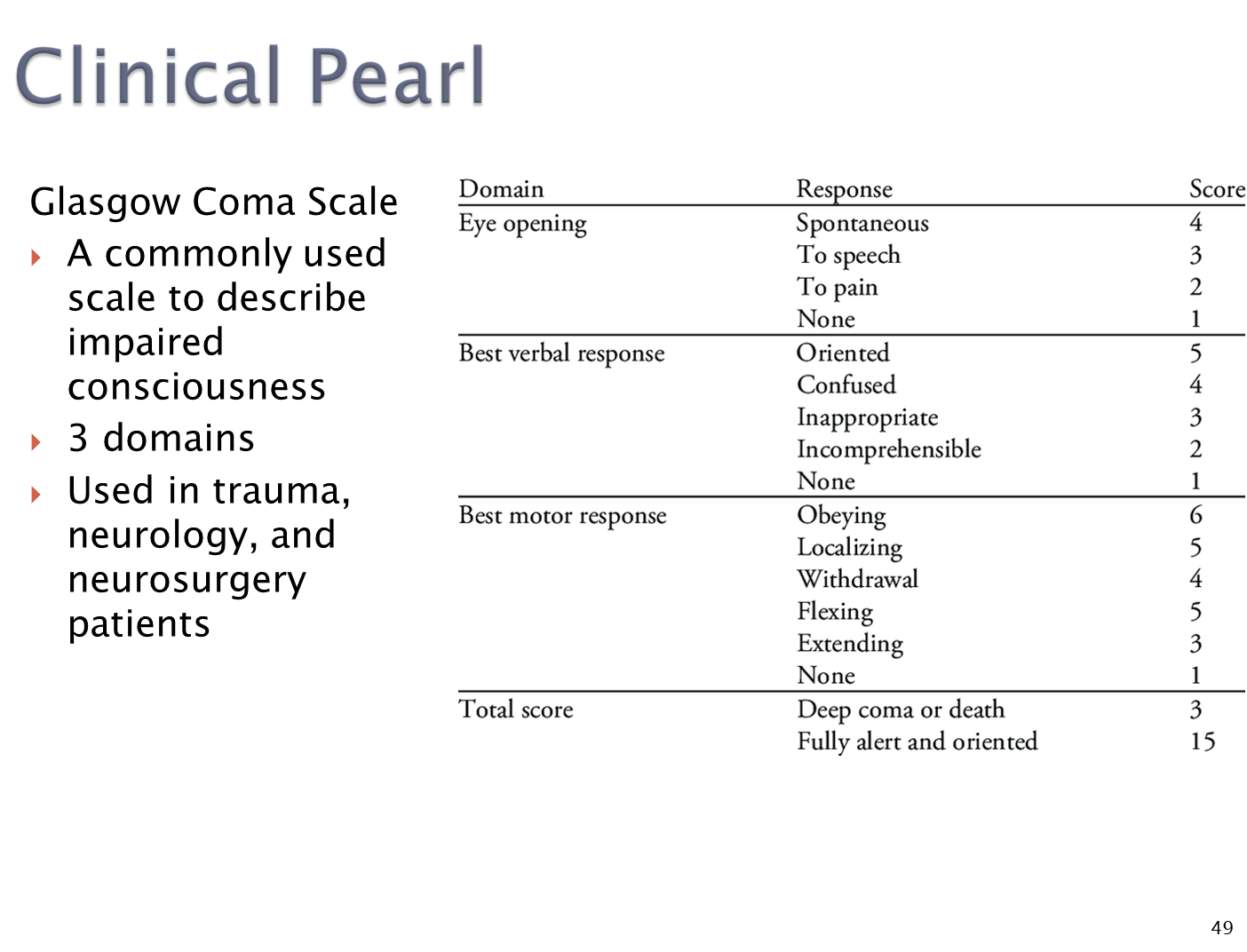
Scale used to describe impaired consciousness
What is the difference between a Decorticate and Decerebrate Posture?
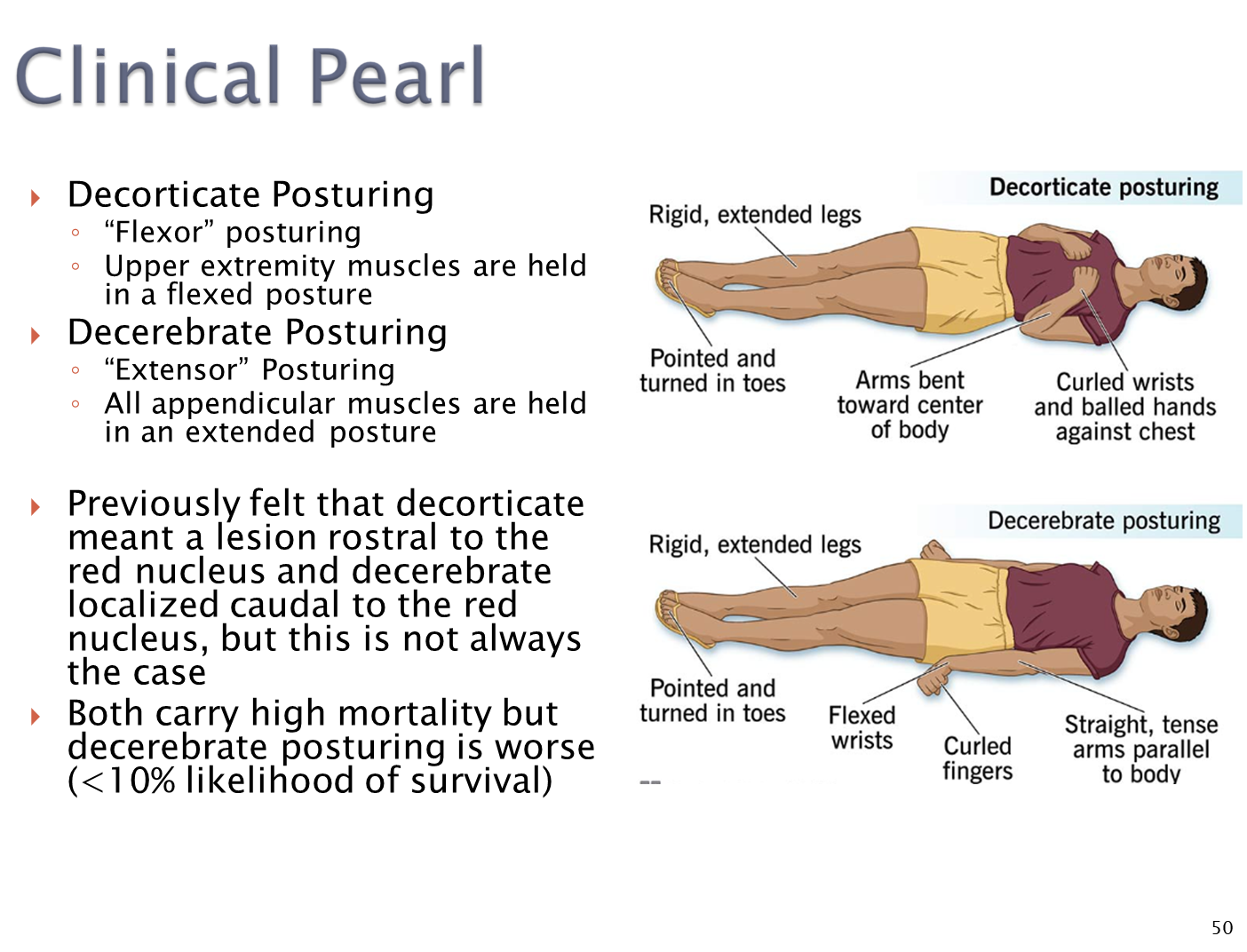
decorticate posture - caused by a brain injury of the red nucleus or higher
→ flexor posture
→ upper extremities are flexed
decerebrate posture - localized lower than the red nucleus
→ extensor posture
→ all appendicular muscle are extended