def of abnormality, mental disorders, behavioural approach to explaining and treating phobias
1/56
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
57 Terms
Defintions of abnormality
Deviation from social norms
Anyone who behaves differently (deviates) from the standards of acceptable behaviour that is set by a social group, and adhered tp by those socialised into that group.
Deviation of these socially created norms is classed as abnormal
Deviation form social norms example
in the past homosexuality was classified as abnormal and regarded as a mental disorder. It was also against the law in the UK. This judgement was based on social deviation - it was made a judgement by society at that time. Other forms of sexual behaviour continue to be classified as abnormal, such as paedophillia and voyeurism. The reason that such behaviours are judged as abnormal; is because they deviate from social norms of what is acceptable
Strength of deviations from social norms definition
this definition does not distinguish between desirable and undesirable behaviour, a feature that is absent from the statistical infrequnecy model
The social deviancy model also takes into account the effect that behavior has on others. Deviance is defined in terms of transgression of social rules and (ideally) social rules are established in order to help people live together. According to this definition, abnormal behaviour is behaviour that damages others. This definition therefore offers a practical and useful way of identifying undesirable and potentially damaging behaviour which may alert others to the need to secure help for the person concerned.
weakness of deviations from social norms definition
What is socially acceptable now may not have been socially acceptable 50 years ago. For example today homosexuality is acceptable in most countries in the world, but in the past it was included under sexual and gender identity disorders in the DSM. Similarly, 50 years ago in Russia, anyone who disagreed with the state ran the risk of being regarded as insane and placed in a mental institution. In fact, Thomas Szasz (1974) claimed that the concept of mental illness was simply a way to exclude nonconformists from society. Therefore, if we define abnormality in terms of deviation from social norm, there is a real danger of creating definitions based on prevailing social morals and attitudes.
Another limitation is that judgements on deviance are often related to the context of behavior. For example, a person on a beach wearing next to nothing is regarded as normal, whereas the same outfit in the classroom or at a formal gathering would be regarded as abnormal and possibly an indication of a mental disorder. Shouting loudly and persistently is deviant behaviour but not evidence of mental disturbance unless it is excessive - and even then it might be a mental disorder. This means that social deviance on its own cannot offer a complete definition of abnormality, because it is inevitably related to both context and degree.
Statistical infrequency
Defined by falling significantly above or below the statistical mean for a characteristic/ criteria.
many aspects being defined of what is normal by referring to typical values
average shoe size
what age is most typical for a woman to have a baby.
example of statistical infrequency
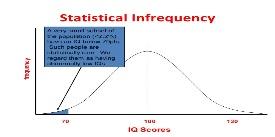
A characteristic e.g fear of dogs, you can ask everyone in your class to say how fearful they are of dogs on a scale of 1 through 10 where 1 is no fear and 10 is extreme fear/panic. We would expect most people to give a middle figure (4,5) - their ratings would cluster around the middle. There would be few people on the ends of the scale. The frequency distribution should look something like the graph shown above - approximately a normal distribution. The abnormal ratings are those at either end because they are not the ‘norm’
strength of statistical infrequency
One STRENGTH of this definition is
That it provides a clear, objective measurement of abnormality. By using statistical data, it avoids subjectivity and personal bias, making it a more scientific approach to identifying uncommon behaviours
weakness of statistical infrequency
Statistical infrequency is sometimes appropriate to define abnormality - for example, intellectual disability is defined in terms of the normal distribution using the concept of standard deviation to establish a cut off point for abnormality. Any individual whose IQ is more than two standard deviations below the mean is judged as having a mental disorder - however such a diagnosis is only made in conjunction with failure to function adequately. Thus suggests that statistical infrequency is only one of a number of tools
The cut off point is subjective - if abnormality is defined in terms of statistical infrequency, we need to decide where to separate normality from abnormality. For example, one of the symptoms of depression is ‘difficulty sleeping’. Some people think abnormal sleep is less than 6 hours a night on average, others might think 5 hours should be the cut off point
The main issue is that there are many abnormal behaviors that are actually quite desirable - for example few people have an IQ that is over 150, but this abnormality is desirable and not undesirable. Equally there are some ‘normal’ behaviors that are undesirable. Experiencing depression for example is relatively common. Therefore, using statistical infrequency to define abnormality means that we are unable to distinguish between desirable and undesirable characteristics
failure to function adequately definition
from an individual's point of view, abnormality can be judged in terms of not being able to cope with everyday living. Functioning refers to just going about day to day life, eating regularly, washing clothes, communication etc - not functioning adequately causes distress and suffering for the individual and/or others.
Important to add others because in some cases individuals may not be under distress like in mental disorders such as schizophrenia as they generally lack awareness of what is wrong with their behaviour. There may be situations where a person is not coping with life in a ‘normal’ way - e.g no reg job and unwashed clothes. If does not cause distress to self or others then a judgement of abnormality is inappropriate
strength of failure to function adequately definition
this definition of abnormality does recognise the subjective experience of the patient - it allows us to view mental disorder from the point of view of the person experiencing it. In addition, ‘failure to function’ is also relatively easy to judge objectively because we can list behaviours (can dress self, can prepare meals - as in WHODAS) and thus judge abnormality objectively - this definition of abnormality therefore has a certain sensitivity and practicality.
weakness of failure to function adequately definition
Who is the person to judge - limitation of this approach is that the judgement depends on who is making the decision, i.e it is subjective - people who are experiencing emotional distress may notice this and seek help as they have judged their behavior as abnormal themselves. However sometimes they can feel content in their abnormality and simply cope with what they are struggling with. For example schizophrenics are potentially dangerous for example Peter Sutcliffe (the yorkshire ripper) - under delusion that they are defending themselves or others from evil, so functioning ‘adequately’.
An important issue is that failure to function adequately is limited by being culturally relative. Definitions of adequate functioning are related to cultural ideas of how one's life should be lived. The ‘failure to function” criterion is likely to result in different diagnoses when applied to people from different cultures, because the standard of one culture is being used to measure another. This may explain for example, why some lower class and non white patients (whose lifestyles differ from the dominant culture) are more often diagnosed with mental disorders - this means that the use of this model is limited by its cultural relativism.
The behaviour may be functional - another limitation is that some apparently dysfunctional behaviour can actually be adaptive and functional for the individual. For example, some mental disorders, such as eating disorders or depression, may lead to extra attention for the individual. Such attention is rewarding and thus quite functional rather than dysfunctional. For example, transvestism is classed as a mental disorder but individuals are likely to regard it as perfectly functional. This failure to distinguish between functional and dysfunctional behaviours means that this definition is incomplete.
deviation from ideal mental health
a definition of abnormality, which suggests that abnormal behaviour should be defined by the absence of particular (ideal) characteristics. Jahoda proposed six principles of ideal mental health, including having a positive view of yourself and being resistant to stress.
6 categories for ideal mental health
Self attitudes: having high self esteem and strong sense of identity
Personal growth and self actualization ; the extent to which an individual develops their full capabilities
integration ; such as being able to cope with stressful situations
Autonomy; being independent and self regulating
Having an accurate perception of reality
Mastery of the environment; including the ability to love, function at work and in interpersonal relationships, adjust to new situations and solve problems.
This deviation from ideal mental health definition proposes that the absence of these criteria indicates abnormality, and potential mental disorder.
Overlap with this and failure to function adequately - in both definitions not being able to cope with stressful situations is a sign of abnormality.
example for deviation of ideal mental health
If someone fails to meet these criteria, they may be considered to have an abnormal mental state. For instance, a person experiencing low self-esteem, inability to cope with stress, and difficulty forming relationships may be classified as having poor mental health because they do not meet the "ideal" state.
strength of deviation from ideal mental health definition
One STRENGTH of this definition is it provides a positive and holistic approach to mental health by focusing on what is needed for well being rather than just the absence of illness. It also sets clear criteria for personal growth and psychological well being, helping individuals strive for better mental health.
weakness of deviation from ideal mental health
it sets the bar pretty high for what is considered ‘ideal’ mental health. Not everyone can meet all the criteria all the time, so a lot of people could be seen as "abnormal" even if they’re doing fine in their lives. Plus, it doesn’t really consider cultural differences—what’s considered ideal in one culture might not apply in another.
characteristics of mental disorders
emotional characterises of PHOBIAS
persistent, excessive and unreasonable fear
coupled with fear are feelings of anxiety and panic
cued by presence or anticipation of a specific object or situation and are out of proportion to the actual danger posed
Cognitive and behavioural characteristics of PHOBIAS
behavioural
avoidance
opposite response ‘fight or flight’ - freeze or faint - freezing = adaptive response because predator may think prey is dead
avoidance interferes with persons life - distinguished between everyday fears and phobias
cognitive
Irrational nature of a persons thinking and the resistance to rational arguments
people recognise fear is excessive and unreasonable, although feature may be absent in children
this distinguished between delusional mental illness and(not aware of unreasonableness of their behaviour) and a phobia
emotional characteristics of DEPRESSION
lack of self esteem and feelings of worthlessness
sadness and loss of pleasure in normal activities
possible feelings of anger
behavioural characteristics of DEPRESSION
appetite may be affected; some people have a reduced appetite where others eat considerably more than usual.
shift in activity level - either reduced or increased. may experience reduced energy
sleep may be affected; the sufferer may sleep more or less
Cognitive characteristics of DEPRESSION
A person will experience negative thoughts about themselves and a sense of self worthlessness
They will experience negative thoughts about the world and expect things to turn out badly
Negative thoughts are irrational and do not reflect the reality about themelseves
Emotional characteristics of OCD
Possible feelings of disgust
Obsessions and compulsion lead to anxiety and stress
Feelings of embarrassment or shame
Behavioural characteristics of OCD
Repetitive and unconcealed behaviours are completed they may be physical e.g hand washing or mental e.g counting
Patients feel the need to complete these behaviours to reduce anxiety
cognitive characteristics of OCD
at some point they will realise their thoughts on obsessions and compulsions are excessive or unreasonable
obsessional themes in thoughts (such as germs are everywhere) which are seen as uncontrollable
intrusive thoughts or impulses that are perceived as inappropriate or forbidden
the behavioural approach to explaining phobias
Phobias
a group of mental disorders characterised by high levels of anxiety in response to a particular stimulus or group of stimuli. The anxiety interferes with normal living.
emotional characteristics
The primary emotional characteristic of a phobia is marked and persistent , and is likely to be excessive and unreasonable. Coupled with fear and feelings of anxiety and panic
These emotions are triggered by the presence or anticipation of a specific object or situation (e.g spiders, flying, heights, seeing blood) and are out of proportion to the actual danger posed.
behavioural characteristics
One obvious behaviour is avoidance. When a person with a phobia is faced with the object or situation that creates fear the immediate response is to avoid it. For example a person with a phobia of spiders avoids being near them. However some people may freeze or faint, the stress response is often described as fight or flight - but is actually fight, flight or freeze - its an adaptive response (prey pretends to be dead). Avoidance in the feared situation interferes significantly with the person's normal routine, occupation, social activities or relationships, and there is marked distress about having the phobia What distinguishes phobias from more everyday fears is that they dont interfere with everyday living. |
cognitive characteristics
These characteristics relate to thought process, in the case of phobias, a defining characteristic is the irrational nature of the person's thinking and the resistance to rational arguments
For example a person with a fear of flying is not helped by arguments that flying is actually the safest form of transport
A further defining characteristic is that the person recognises that their fear is excessive or unreasonable, although this feature may be absent in children. This characteristic distinguishes between a phobia and a delusional mental illness (e.g schizophrenia) where the individual is not aware of the unreasonableness of their behaviour
two process model
Mowrer 1947 proposed the two-process model to explain how phobias are learned. The first stage is classical conditioning and then, in a second stage, operant conditioning occurs. Both processes are needed to explain why phobias begin in the first place and then continue.
Classical conditioning : INITIATION
A phobia is acquired through ASSOCIATION - the association between a neutral stimulus (NS) such as a white furry rat, and a loud noise results in a new stimulus response being learned, as demonstrated by little Albert:
little Albert
11 month old - showed no fear response to white furry objects (NS) + UCS (loud noise) results in a new stimulus response being learned which would be fear.
UCS was a loud noise and the original UCR was fear. By pairing the loud noise with the furry object acquired the same properties as the UCS and produced the response of fear which was now the CR (conditioned response) because this is a learned response. When albert saw a white furry rat he cried because presumably it was now associated with fear.
same for when bitten by a dog
being bitten (UCS) creates fear (UCR)
dog (NS associated with being bitten (UCS)
dog (now CS) produces fear response (now CR)
Operant conditioning : MAINTENANCE
Through classical conditioning a phobia is acquired however the phobia is maintained through operant conditioning.
The likelihood of a behaviour being repeated is increased if the outcome is rewarding. In the case of a phobia, the avoidance or escape from the phobic stimulus reduces fear and thus is reinforcing. This is an example of negative reinforcement (escaping an unpleasant situation). The individual avoids the anxiety created by, for example, the dog by avoiding them entirely
A03 - the importance of classical conditioning
People with phobias often do recall a specific incident when their phobia appeared e.g being bitten by a dog
However, not everyone who has a phobia can recall such an incident. It is possible that such traumatic incidents did happen, but have since been forgotten. Sue et al suggests that different phobias may be the result of different processes, for example, agoraphobics were most likely to explain their disorder in terms of a specific incident, whereas arachnophobics (spiders) where most likely to cite modelling as the cause
This demonstrates the role of classical conditioning in developing phobias, but other processes may be involved in their maintenance.
can provide some convincing explanations for phobias e.g people remember traumatic events
A03 - Diathesis stress model
A problem with the two-process model is that it does not explain that when a neutral stimulus becomes associated with a fearful experience the result should be a phobia, but this doesn't always happen. However this could be explained by research that has found that not everyone who is bitten by a dog develops a phobia. This research was explained by the diathesis-stress model. This proposes that we inherit a genetic vulnerability for developing mental disorders. However, a disorder will only manifest itself if triggered by a life event, such as being bitten by a dog. Therefore a dog bite would only lead to a phobia in those people with such a vulnerability. Therefore, the behavioural explanation is incomplete on its own.
A03 0 biological preparedness
The fact that phobias do not always develop after a traumatic incident may be explained in terms of biological preparedness. Seligman suggests that animals, including humans are genetically programmed to rapidly learn an association between potentially life-threatening stimuli and fear. These are referred to as ancient fears- things that would have been dangerous in our evolutionary past. It would have been adaptive to rapidly learn to avoid such stimuli. This concept would explain why people are much less likely to develop fears of modern objects such as toasters and cars that are much more of a threat than spiders. Such items were not a danger in our evolutionary past. This suggests that the behaviour approach cannot explain all phobias.
overview
Classical Conditioning | Said to have occurred when the Conditioned Stimulus produces the Conditioned Response |
Unconditioned Stimulus (US or UCS) | A stimulus which produces an Unconditioned Response without conditioning being required |
Unconditioned Response (UC or UCR) | An automatic or inherent response to the Unconditioned Stimulus |
Conditioned Stimulus (CS) | Initially neutral (stimulus) with respect to the Unconditioned Response which is, by conditioning, associated with the Unconditioned Stimulus |
Conditioned Response (CR) | The response to the Conditioned Stimulus once classical conditioning has been established |
Extinction | The gradual weakening of a conditioned response that results in the behaviour decreasing or disappearing. This happens when a conditioned stimulus is no longer paired with an unconditioned stimulus. |
Stimulus Generalisation | A tendency for the conditioned stimulus to evoke similar responses after the response has been conditioned |
practice question : Kirsty is in her twenties and has had a phobia of balloons since one burst near her face when she was a little girl. Loud noises such as ‘banging’ and ‘popping’ cause Kirsty extreme anxiety, and she avoids situations such as birthday parties and weddings, where there might be balloons.
Suggest how the behavioural approach might be used to explain Kirsty’s phobia of balloons. (4 marks)
Kirsty’s phobia has developed through classical conditioning – she has formed an association between the neutral stimulus (balloon) and the response of fear
the conditioned response is triggered every time she sees a balloon (or hears similar noises)
her phobia has generalised to situations where balloons might be present, such as parties and weddings, and to similar noises, ‘banging’ and ‘popping’
her phobia is maintained through operant conditioning – the relief she feels when avoiding balloons becomes reinforcing.
Credit other relevant features of conditioning applied to Kirsty’s phobia.
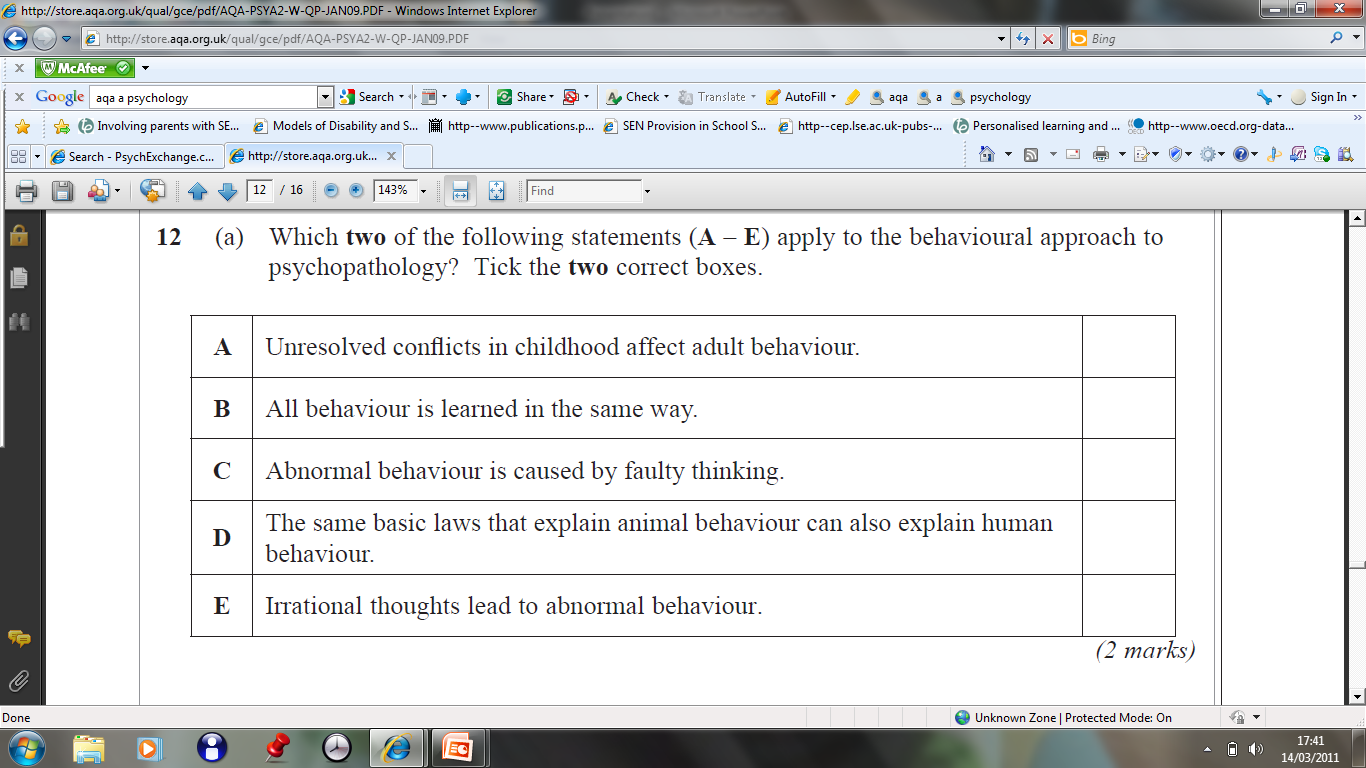
B and D
The behavioural approach to treating phobias
Systematic desensitisatioon
Joseph Wolpe 1958 developed this technique where phobics were introduced to the feared stimulus gradually and through counterconditioning would learn a new association.
counterconditioning
is where the patient is taught through classical conditioning. to associate the phobic stimulus with a new response i.e relaxation instead of fear in this way their anxiety is reduced - they are desensitized
relaxation
the therapist teaches the patient relaxation techniques eg deep breathing exercises - slowing down breathing helps us relax. Progressive muscle relaxation is also used where one muscle at a time is relaxed.
desensitisation hierarchy
SD works by introducing the person to the feared situation one step at a time so it is not overwhelming. At each stage the patient practices relaxation so the situation becomes more familiar, less overwhelming, and their anxiety diminishes
flooding
An alternative to the gradual exposure as used in SD, is to have one long session where their phobia being experienced at its worst, Session continues until their anxiety has been dealt with.
For example a person who is afraid of clowns is placed in a room full of clowns or spiders. Someone has to sit with a large hairy spider on their hand. The person with the spider remains in a position until they become calm.
The first step is patient is taught how to relax their muscles completely (relaxed state is incompatible with anxiety)
This usually lasts throughout one long session
A person’s fear response has a time limit, as adrenaline levels naturally decrease a more relaxed state can be acquired as we only have a finite amount of adrenaline.
A03 - systematic desensitisation
Point: research has found that SD is successful for a range of phobic disorders
Evidence: for example McGrath et al 1990 reported that about 75% of patients with phobias respond to SD. The key success appears to lie with actual contact with the feared stimulus.
Explain: This suggests that in vivo techniques are more successful than ones just using pictures or imagining the feared stimulus.
Link: Often a number of different exposure techniques are involved - in vivo, in vitro and also modelling where the patient watches someone else who is coping well with the feared stimulus
This demonstrates the effectiveness of SD but also the value of using a range of different exposure techniques.
A03 - not appropriate for all phobias
Point: However SD may not be appropriate for all phobias
Evidence: Ohman et al 1975 suggest that SD may not be as effective in treating phobias that have an underlying evolutionary survival component (e.g fear of the dark, fear of heights or fear of dangerous animals), than in treating phobias which have been acquired as a result of personal experience.
Explain/elaborate: ??
Link: this suggests that SD can only be used effectively in tackling some phobias.
A03 - symptom substitution
Point: Behavioural therapies may not work with certain phobias because the symptoms are only the tip of the iceberg.
Evidence:if the symptoms are removed the cause still remains, and the symptoms will simply resurface. For example, according to the psychodynamic approach phobias develop because of projection. Freud 1909 recorded the case of little hans who developed a phobia of horses. The boy's actual problem was an intense envy of his father, but he could not express this directly and his anxiety was projected onto the horse. The phobia was cured when he accepted his feelings about his father.
Explain/elaborate: This suggests that symptoms may resurface, possibly in another form (symptom substitution)
Link: This demonstrates the importance of treating the underlying causes of a phobia rather than just the symptoms.
strengths of behavioural therapies
Point: A strength of behavioural therapies for dealing with phobias is that they are generally fast and require less effort and are cheaper than other psychotherapies.
Evidence: for example CBT requires a willingness for people to think deeply about their mental problems, which is not true for behavioural therapies.
Explain/elaborate: This lack of thinking means that the technique is also useful for people who lack insight into their motivations or emotions such as children or patients with learning difficulties. A further strength of behavioural therapy is that it can be self administered - a method that has proved successful with fro example, social phobia.
Link: these benefits were confirmed in the study described in research methods, which also found that self administered therapy was as effective as therapist guided therapy.
A03 - flooding
Individual differences
Point: Flooding is not appropriate for every patient.
Evidence:it can be a highly traumatic procedure. Patients are obviously made aware of this beforehand but, even then, they may quit during the treatment, which reduces the ultimate effectiveness of the therapy for some people.
Explain/elaborate: The therapy is therefore less effective for some people.
A03 - effectiveness
Effectiveness
Point: Flooding is an effective quick treatment for patients who stick with it.
Evidence: for example, choy et al reported that both SD and flooding were effective but flooding was the more effective of the two at treating phobias
Explain/elaborate: On the other hand another review concluded that SD and flooding were equally effective in the treatment of phobias. This shows that flooding is an effective therapy, albeit just one of several options.
A03 - relaxation may not be necessary
Point: The success of both SD and flooding may be more to do with the exposure to the feared situation than relaxation, and the expectation of being able to cope is most important.
Evidence: for example kelin et al 1983 compared SD with supportive psychotherapy for patients with either social or specific phobias. They found no difference in effectiveness.
Explain/elaborate: This suggests that the ‘active ingredient’ in SD or flooding may simply be the generation of hopeful expectancies that the phobia can be overcome.
This suggests that the cognitive factors are more important than the behavioural approach generally acknowledges.
WHODAS