Surface Anatomy Of The Forebrain - The Occipital Lobe
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
16 Terms
How many major anatomical areas of the occipital lobe are identified and on which surface are the named structures located?
Both named structures — the cuneus and the lingual gyrus — are located on the medial surface of the occipital lobe
Describe the anatomical boundaries and shape of the cuneus.
The cuneus is a wedge‑shaped region on the medial occipital lobe.
Boundaries:
Above: Parieto‑occipital sulcus
Below: Calcarine sulcus
What are the two sulci that form the boundaries of the cuneus, and what other lobes do these sulci help demarcate?
The cuneus is bordered by two major medial‑surface sulci:
Parieto‑occipital sulcus (superior boundary)
Also separates the parietal lobe from the occipital lobe
Marks the posterior border of the precuneus
Calcarine sulcus (inferior boundary)
Houses the primary visual cortex (V1) in its walls
Describe the anatomical position of the lingual gyrus in relation to the calcarine sulcus.
The lingual gyrus sits below the calcarine sulcus on the medial surface of the occipital lobe
Because the cuneus lies above the calcarine sulcus, the lingual gyrus is positioned directly beneath the cuneus, with the calcarine sulcus separating them
Why is the positional relationship of the lingual gyrus to the calcarine sulcus functionally important?
The calcarine sulcus contains primary visual cortex (V1)
The cuneus (above) receives the lower visual field, and the lingual gyrus (below) receives the upper visual field
Because the lingual gyrus sits just below the calcarine sulcus, it forms one half of the cortical “shell” around V1 — crucial for organising the map that makes vision meaningful
What is the primary function of the occipital lobe?
The occipital lobe is devoted almost entirely to visual processing
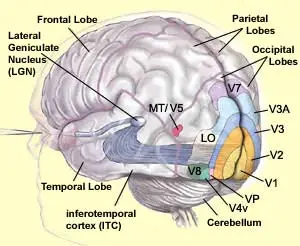
It contains a hierarchy of visual areas:
V1 – primary visual cortex
V2 – secondary visual cortex
V3 – visual association cortex
Where precisely is the primary visual cortex (V1) located within the occipital lobe?
Primary visual cortex (V1) sits inside the walls of the calcarine sulcus on the medial surface of the occipital lobe
Some surrounding medial cortex also contributes, but most of V1 is buried deep within the sulcus, making it not visible on the external surface of an intact brain
Describe the topographic organisation of V1, V2, and V3 in terms of their spatial arrangement relative to one another.
V1 sits in the calcarine sulcus and the immediately surrounding medial cortex
V2 forms a ring around V1, lying just outside it
V3 lies beyond V2, forming the next outer zone and extending into the temporal lobe
What is the significance of V3 (visual association cortex) extending into the temporal lobe?
V3 stretches into the temporal lobe because visual processing continues there after the occipital lobe finishes the early steps
The temporal lobe handles recognising objects and faces, so V3’s extension helps link basic vision to meaningful visual recognition
What is the clinical consequence of complete destruction of the primary visual cortex (V1) in one hemisphere?
Complete destruction of V1 on one side → contralateral homonymous hemianopia.
Example: Right V1 lesion → loss of the left visual field in both eyes
The other (ipsilateral) field is spared because all visual input from one hemisphere projects to the opposite V1
Why might macular (central) vision be partially spared following posterior cerebral artery (PCA) territory infarction involving V1?
Macular (central) vision is often spared because the occipital pole — which represents the macula — has a dual blood supply
It receives blood from both the PCA and branches of the MCA
So when the PCA is infarcted, the MCA can still perfuse the occipital pole, preserving central vision
How does damage confined to V1 differ clinically from damage extending to V2 and V3?
Damage limited to V1:
→ Loss of conscious vision in the opposite visual field (hemianopia/scotoma)
→ Basic visual detection is gone in that regionDamage extending into V2 and V3:
→ Adds higher‑level visual deficits: problems with motion, colour, and complex visual discrimination
→ Moves from “can’t see it” to “can’t interpret it”
Summarise the key anatomical features of the occipital lobe, including surfaces, named structures, and visual cortex organisation.
Lateral surface:
→ The lateral occipital gyriMedial surface:
→ Cuneus above the calcarine sulcus
→ Lingual gyrus below the calcarine sulcusVisual cortex layout:
→ V1 in the calcarine sulcus
→ V2 surrounds V1
→ V3 lies further out and extends into the temporal lobe
A patient sustains a right PCA infarction destroying right V1. What is the expected visual field deficit?
Right V1 processes the left visual field
Destroying right V1 → loss of the left visual field in both eyes
This produces a left homonymous hemianopia
Damage to the cuneus specifically would be expected to produce which visual field defect?
The cuneus represents the inferior (lower) visual field
So damage to the cuneus → loss of the opposite lower visual field
This produces a contralateral lower quadrantanopia
A patient with a lesion of the lingual gyrus is expected to lose vision in which part of the contralateral visual field?
The lingual gyrus represents the upper (superior) visual field
So a lesion here causes loss of the opposite upper quadrant
This is a contralateral superior quadrantanopia — the classic “pie on the floor” defect