PATHO: Electrolyte Balance & Exemplars
1/92
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
93 Terms
Fluid & Electrolyte Balance definition
The various body fluids and electrolytes (intracellular, extracellular, intravascular, and transcellular) that when in balance promote homeostasis.
electrolyte imbalances
abnormal plasma concentrations of electrolytes
deficit and excess
chloride is
main extracellular anion
chloride concentration is
proportional to sodium
typically follows sodium
where is chloride found
in stomach
chloride is a component of
hydrochloric acid
hypochloremia causes
• Vomiting, diarrhea (lost from stomach)
• NG suctioning
• Alkalosis (acid being left)
hypochloremia signs and symptoms
• Weakness
• Headache, nausea
• Hyponatremia
• Fluid excess – cerebral edema, seizures
Hyperchloremia causes
• Dehydration
• Acidosis
Hyperchloremia signs and symptoms
• Decreased urine output
• Thirst d/t dehydration
• Hypernatremia
• Tachy
• may be asymptomatic
potassium is a
Predominant ICF electrolyte
potassium maintains
resting membrane potential
potassium abnormalites can
quickly lead to lethal complications, particularly cardiac issues
potassium and cell
potassium should be inside the cell not outside
Hypokalemia causes
• Decreased intake, GI loss thru suctioning, loop diuretics
• Fluid overload
• Alkalosis
• prolonged anorexia
Hypokalemia signs and symptoms
• Flat T waves, ST depression, v-fib
• Decreased DTRs
• Respiratory arrest
• Confusion
Hyperkalemia causes
• Renal failure
• Tissue trauma, burns
• Hypoxia
• Acidosis
• Insulin deficiency
• Results in K+ movement from ICF to ECF
Hyperkalemia signs and symptoms
• Peaked T waves, wide QRS, bradycardia, heart blocks, dysrhythmias (decreased contractility)
• Numbness, tingling
• N/V/D
where is majority of calcium found
in bone
small amount of ionized (free) calcium bound to proteins in serum
what is calcium essential for
coagulation, muscle contraction,
what does calcium act as
messenger in some hormonal pathways
Hypocalcemia causes
• Renal failure
• Decreased PTH secretion
• Vitamin D or calcium deficiency in diet
Hypocalcemia signs and symptoms
• Tetany
• Numbness, tingling
• Hyperactive reflexes
• Positive Chvostek & Trousseau signs
• Bone pain, fractures
• Prolonged QT intervals, cardiac arrest
Hypercalcemia causes
• Malignancy
• Hyperparathyroidism, hyperthyroidism
• Immobilization
• Excessive consumption of Ca+ or Vit D (dairy, green leafy vegetables, salmon)
Hypercalcemia signs and symptoms
• Anorexia, N/V
• Muscle weakness d/t blockage of Na+ channels
• AV block
• Lethargy, coma (everything is slowed down)
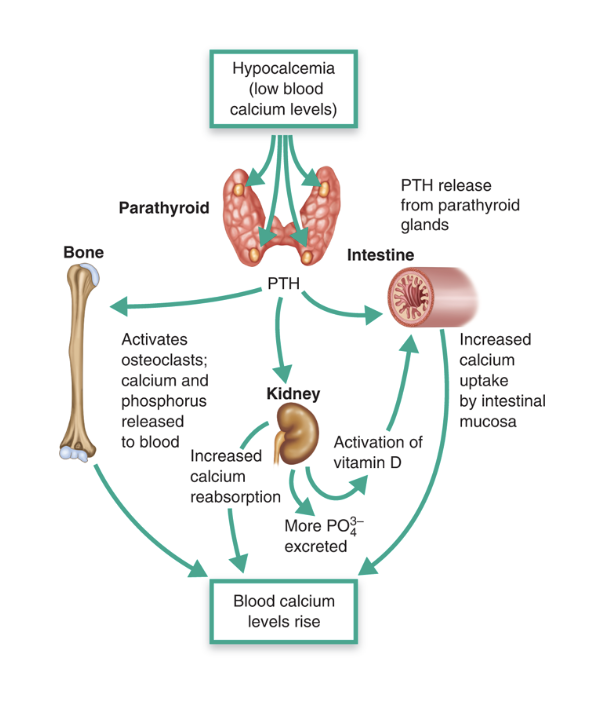
PTH/ hormonal regulation and fluid electrolyte balance
hypocalcemia→ pth→ blood calcium levels rise
phosphorus role
Bone formation,
what does phosphorus act as
biffer in acid-base balance
what is phosphorus involoved in
blood cell and platelet function
phosphorus relationship
Has inverse relationship with calcium – if one is elevated, other is decreased and vice versa
Hypophosphatemia causes
• Malnutrition, alcohol abuse
• Heat stroke, burns
• Hyperparathyroidism
• Hypercalcemia
Hypophosphatemia signs and symptoms
• Joint stiffness, bone pain
• Bleeding disorders
• Seizures
Hyperphosphatemia causes
• Chronic renal failure
• Acidosis
• Hypocalcemia
• Chemotherapy
Hyperphosphatemia signs and symptoms
• Tetany (decrease in calcium= excitability)
• Decreased BP
• Cardiac dysrhythmias
magnesium is a
intracellular cation
what is magnesium regulated by
PTH
what does magnesium have a role in
ATP generation, smooth muscle relaxant
Hypomagnesemia causes
• Alcohol abuse
• Hypocalcemia
• Decreased protein
• DKA
Hypomagnesemia signs and symptoms
• Hypertension, tachycardia
• Tetany
• Cardiac dysrhythmias (PVCs, v-tach)
• Seizures
Hypermagnesemia causes
• Renal failure
• Laxative abuse
• Burns
Hypermagnesemia signs and symptoms
• Hypotension
• Lethargy
• Cardiac dysrhythmias (tall T waves, wide QRS, prolonged QT)
• Decreased DTRs
• flushing→ respiratory failure
when do burns occur
when soft tissue exposed to high-energy heat producing elements
what happens to skin functions after a burn
All functions of skin become impaired – risk for infection, sensation impairment
after a burn cells are unable to
regulate water absorption
sodium pump fails, water and electrolytes leak out into interstitial spaces
after a burn there is loss of
circulatory volume (from loss of regulation of water absorption)
hemoconcentration and increased blood viscosity occur
after burn what response happens
Systemic inflammatory response – cellular mediators disrupt every system
superficial burn
epidermis, sunburn
first degree burn
superfical partial thickness
epidermis and papillary dermis involved; blistering, full pain sensation
2nd degree
Deep partial thickness
epidermis, papillary dermis, and reticular layer of dermis; blistering, does not blanch, no pain sensation
2nd degree
full thickness
all epidermal, dermal layers, and subcutaneous tissues affected; skin charred, pale, painless, need surgery
3rd degree
Full Thickness and Deeper Tissue
destruction of epidermis, dermis, and underlying subcutaneous tissue, tendons, muscle, and bone
3rd degree
amputation probably
Zone of coagulation
area that has been completely burned
zone of stasis
fibrin deposits, vasoconstriction, may be viable
Zone of hyperemia
typically will recover, vasodilation d/t inflammation
thermal burns
scalding, radiation; occurs from a heat source
chemical burns
Direct contact, inhalation and ingestion with corrosive and caustic substances
electrical burns
passage of electrical current through the body to the ground or electrical flames or radiation; leads to internal damage along pathway of electrical charge
how to determine percent of body affected
rules of nines
burn complications
Scarring
Contractures
Hypovolemia
Infection
Inhalation Injuries – ARDS – increased mortality
Skin Graft (Donor Site)
Hypermetabolism – need proper nutrition to heal
Pain management
kidney functions
• Regulate body fluids and electrolytes
• Excrete waste products
acute kidney injury
abrupt reduction in kidney function; accumulation of nitrogenous wastes (azotemia)
acute kidney injury levels
BUN- inceased
creatinine- increased
GFR- decreased
AKI is often
reversible
prerenal AKI
reduced blood flow to the kidney
reducked arterial blood volume
intrinsic AKI
direct damage to the kidneys
postrenal AKI
obstruction of the urinary collecting system
kidney stones, bladder tumor, prostate
AKI – Pre-renal
Decreased blood flow to kidney d/t decreased volume from hypovolemia, heart failure, or vasodilation (sepsis)
when is RAAS initiated
AKI- pre renal
what does RAAS do
increase resorption of H2O and Na+
AKI – Intrarenal/Intrinsic
Direct damage to kidneys
Glomerulonephritis
Nephrotoxins
Rhabdomyolosis
when do you have greatest risk for CKD
AKI- intrinsic
AKI – Postrenal
Obstruction of urinary collecting system; cessation of urine flow
AKI – Postrenal obstructions
Tumors, kidney stones, ureteral strictures
AKI – Postrenal obstructions leads to
hydronephrosis (water/fluid in kidneys)
AKI Signs and Symptoms
• Rise in BUN, urea, & creatinine
• Decreased GFR and urine output
• Edema
• Electrolytes - decreased Ca, increased PO4, increased K+
• Acute Tubular Necrosis
Acute Tubular Necrosis
Vasoconstriction & direct damage – inflammatory response, promotes renal tubule epithelial injury; obstructs filtrate
AKI Phases: initiation phase
phase of reduced perfusion or toxicity in which kidney injury is evolving
AKI Phases: extension phase
continued hypoxia following the initial ischemic event and inflammatory response; blood flow returns to proximal tubules
AKI Phases: maintenance phase
cells undergoing repair; can last weeks to months, urine output is lowest
AKI Phases: recovery phase
glomerular function returns but tubules cannot yet concentrate filtrate; return to normal can take 3-12 months
chronic kindye disease is
ESRD – end-stage renal disease
Chronic Kidney Disease (CKD): Diabetic nephropathy
more than 50% of cases; increased glucose leads to basement membrane thickening, increased glomerular permeability; proteinuria, albuminuria
Chronic Kidney Disease (CKD): Hypertensive nephrosclerosis
increased pressure in glomerulus leads to damage of cells, scarring of glomerulus; damage to arterioles – other vessels compensate leading to thickening
Chronic Kidney Disease (CKD): chronic glomerulonephritis
direct injury, antibody deposition & chronic inflammation
CKD Manifestations
retinopathy
peripheral neuropathy
dyspnea on exertion
anorexia
N/V
bone pain
muscle loss
seizures
hypertension
heart failure
amenorrhea
uremic frost
pruitus
CKD and cardiovascular disease
chronic inflammation, hyperlipidemia , hypertension, heart failure
CKD and metabolic acidosis
retain H+ ions
CKD and mineral bone disease
normally, kidneys produce activated Vit D (calcitriol) when Ca falls; end up with hypocalcemia and hyperphosphatemia; high level of bone turnover, fractures
CKD complications
Anemia
hyperkalemia
hypervolemia
uremia
anemia
lack of erythropoietin production; heart remodeling
hyperkalemia
decreased aldosterone secretion, decreased K+ excretion
hypervolemia
decreased excretion of Na+ and H2O
uremia
urea accumulates in bloodstream; N/V, headache fatigue, uremic frost, metallic taste, lethargy, irritability, pruritis