Step 1
1/148
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
149 Terms
"Inflammation of the epiglottis due to H influenze type b infection (now not as common due to Hb vaccine)
Presentation: Child with high fever, drooling, dysphagia & in the tripod position (hands on knees and head titled) to get more air
"Hand on my knees, Hb, epligottis"" Think of Thot Sh** by Meg thee Stallion
Tracheal deviation & precussion: None
Lung sound: Respiratroy stridor
Imaging: ""Thumb sign"" on lateral neck X-ray
What is it? Cause? Presentation? Lung sound? Imaging?
Tracheal deviation & precussion?
"Inflammation of the larynx and trachea usually caused by Parainfluenza virus
Presentation: Child with fever, barking ""seal-like"" cough
*croup = poop on a seal in a church; church have a particular influen(za)ce
Lung sound: Inspiratory stridor
Tracheal deviation & precussion: None
Imaging: ""Steeple sign"" on frontal neck x-ray (subglottic narrowing) *Difference b/w epiglottitis & croup
What is it? Cause? Presentation? Lung Sound?
Lung Abscess
Cause? Presentation? Imaging?
"Contained and localized pus collection in lungs; Cause: Asprirated oral flora anaerobes or S aureus
Presentation: Fever, night sweats, weight loss & cough with foul-smalling sputum (bc of pus)
Imaging: X-ray shows ""air-fluid level"" cavitation filled with pus
"
Pulmonary Edema
Caused by increase in (1) ______ pressure & (2) ______ pressure
What are 2 causes of increase in (1) ____ pressure? Histology?
What is causes of increase in (2) ____ pressure?
Presentation (including lung sounds & CXR)
Management
COPD: Emphysema
Spirometry (FEV1/FVC, RV, FRC, TLC & DLCO)
Imaging (CXR)
Pathophysiology
Presentation
Lung sounds & precussion
How do pts w/ emphysema breathe?
Two types of emphysema?
Cause?
Typical pt?
Where in lungs?
Histology?
"Spirometry:
Very very decreased FEV1 and decreased FVC --> Decreased FEV1/FVC
Obstruction --> Air trapping --> hyperinflated lungs --> Increased RV, FRC & TLC
Pathophysiology
Lung elastic tissue destruction --> Increased compliance --> EPP moves towards alveoli --> Dynamic airway collapse
Presentation: Pink Puffers
Cyanosis usually absent bc no V/Q mismatch since BOTH alevolar destruction & alveolar capillary destruction
Lung Sounds: Ronchi
Percussion: Hyperresonant
Pursed lips during expiration → keeps airway open bc creates build up pressure
Types:
Centriacinar:
Cause: ""C ~S for smoke"" Smoke → ↑ Neutrophil elastase (protease) release → tissue destruction (upper lobes, central respiratory bronchioles; sparing of distal)
Typical pt: >45 yo w/ a smoking history
Panacinar:
Cause: ɑ1-Antitrypsin (AAT) deficiency → ɑ1-Antitrypsin inhibits elastase → ↑Elastase activity with tissue destruction (lower lobes; BOTH central & distal alveoli)
Typical pt: 25-45 yo w/ family history; usually non-smoker (but smoking still makes it made); lung AND liver involvement
Histology: Polymerized mutant AAT (AAT made in liver so they bunch up in liver)→ PAS+ globules in liver → Liver cirrhosis
2 types
Lung sounds, percussion & tracheal dilation
"Spontaneous PTX
Lung sounds: Decreased or absent
Percussion: Hyperresonant
Tension PTX
Lungs are collapsing as air accumulates in the pleural space
Lung sounds: Decreased or absent
Percussion: Hyperresonant
Tracheal Deviation: Away from affected side bc air generates + pressure so the trachea moves away
"
"Class III AND Class II (beta blocker)
SoTOTAL
Class III antiarrhythmic AIDS
S in AIDS
Mechanism:
Class III :. Inhibition of K+ channels (delayed rectifier K current) —> QT prolongation
B Blocker :. Prolonged PR interval bc delay in conduction by pacemaker from SA/AV
Side Effects: Bradycardia
Acute? Chronic?
Murmur? What increases murmur?
Presentation?
Associations?
"Infection of lung tissue
Presentation: Fever. Cough (productive in lobar/bronchopneumonia & non-productive in interstitial) Sputum is yellow-green due to myeloperoxidase *looks like yellow* in neutrophils
Lungs sounds: Rales (sounds like rice crispy: snap, crackle & pop open) & bronchial breath sounds over lung paryenchma
Lung exam: Increased fremitus & dullness to percussion
Tracheal Deviation: None
Three Patterns
(1) Lobar (typical) Intra-alveolar exudates --> lobe consolidation; Cause: Strep pneumoniae
Congestion (<2 d): Microbe causes alveolar macrophages to release cytokines --> vasodilation + bacterial exudate
Red hepatization (2-4 d): Hepatization = bc lungs firm up like liver; Exudate begins to include RBCs (hence red), nuetrophils, firbin
Grey hepatization (4-6 d): RBCs become lysed and degraded thus loses red color & looks grey instead
Resolution: Macrophages replace neutrophils and digest the fibrinous exudate + Type 2 pneumocyte hyperplasia (which give rise to new Type 1 pneumocytes since they were destroyed by inflammation)
(2) Bronchopneumonia: Infection similar to typical/lobar but focused in bronchioles and nearby alveoli in lobes --> patchy opacities in lobes; Cause: Staph Aureus
(3) Interstitial (Atypical): Infection of interstitium (b/w alveoli) --> patchy diffuse opacities; mild course including low grade fever; Cause: Viral, Legionella, Mycoplasma
Histology:
*Recall: Aspiration pneumonia is not a pattern of PNA, but a way of getting PNA --> aspirated oral flora anaerobes (unconscious, seizure & alochol use disorder) and gram negative bacteria, Klebsiella"
Asthma
Definition
Presentation (lung sounds & percussion)
Diagnosis
Pathological Sputum Findings
Subtypes
"Definition: Episodic & reversible bronchoconstriction
Presentation: Coughing, dyspnea, hypoxemia but asymptomatic between episodes
Lung Sounds: Wheezing
Percussion: Hyperresonant during attack
Diagnosis
Normal when asymptomatic so must induce asthmatic episode via methacholine challenge (chilinomimetic like acetylcholine --> bronchoconstriction) and do spirometry:
Decreased FEV1/FVC AND Decreased Inspiration/expiration time (1/2 --> 1/4)
Pathological Sputum Findings
More esosinophils
Charcot-Leyden crystals (eosinophil granules)
Curschmann spirals
Subtypes:
(1) Atopic (extrinsic) - Type 1 hypersensitivity rxn due to allergn. Usually childhood onset with hx of atopic triad (atopic dermatitis or allergic rhinitis)
Classic triggers include; pets, dust & pollen
(2) Non-atopic (intrinsic) - No identifiable allergen. Usually follows viral infection, stress or exercise
(3) Status asthmaticus: Acute severe asthma --> unremitting & possibly fatal
(4) NSAID-Induced Asthma: Occurs in adults; NSAIDs block COX pathway, thus increase production of leukotriene through LOX pathway. Associated with nasal polyps (in adults - unlike CF where it is in children) and chronic rhinosinusitis"
What leads to bronchoconstriction/ bronchodilation?
"
"
2 Phases
What is involved?
"Phase 1: Sensitization
(1) Initial exposure to allergen --> Th2 cells presented with antigen by antigen present cell (APC)
(2) Th2 --> does 2 things
First, IL-5 for eosinophil recruitment
Second, IL-4 and IL-13 which leads to plasma cell producing IgE antibodies against allergen
(3) End result: Mast cell primed with IgE antibodies
Phase 2: Reaction (repeat exposure)
(1) Antigen binds to IgE on mast cell and mast cell degranulates releasing histamine & leukotrienes
(2) Early phase: Histamine & leukotriene cause bronchoconstriction
(3) Late phase: Histamine & leukotriene lead to vasodilation and eosinophil recruitment
Eosinophil releases major basic protein --> inflammation and mucus production
"
Class? Mechanism?
Use?
Zileuton
"Anti-lipoxgenase (LOX)
Zileuton --> leukotrienes
"
Spirometry: FEV1/FVC? RV, FRC & TLC?
How do ppl with CB breathe?
Cause & pathophysiology?
What is the Reid index?
Presentation?
Classic lab values? (PAO2, PaCO2, pH & bicarb)
Will oxygen therapy help?
Treatment? (Acute exacerbation & everday)
Aortic Stenosis
Murmur & increase of intensity
HF?
Cause
Unique fr
"Murmur: Holosystolic crescendo-decrescendo @ 2nd ICS
S4 - from hitting a thick wall
Increase murmur: increase preload and decrease afterload & expiration
Cause:
(1) Dystrophic calcification (older pt)
(2) Bicuspid aortic valve (younger pt)
HF: Diastolic HF —> LV concentric hypertrophic
Presentation:
- Triad (1) Exertional dyspnea (2) Angina (3) Syncope
(4) Pulsus Parvus & tarsus
(5) Single/SoftS2 (bc it takes longer for aortic valve to close, so it closes ~ time as pulmonic)
"
"Cystic Fibrosis
Genetics
Pathophysiology in different organs
Consequences (Ex. Infections from what organisms for child vs. adults)
Diagnosis
Treatment
Genetics: Autosomal recessive mutation in CFTR gene on ch7 → Phe508del
Pathophysiology:
CFTR gene encodes an ATP-gated Cl- channel → Mutated protein is misfolded and improperly trafficked to cell membrane
GI tract and Lungs/Respiratory:
Cl- trapped within cells → ↑Na+ and H2O reabsorption into cells
↑ Na+ reabsorption → ↑Negative transepithelial potential difference (NA+ is attracted to (-) charge)
↑ H2O reabsorption → Thick and dehydrated mucus in lumen → Obstruction and distension
Sweat glands:
Mutated channel → ↑ Cl- in sweat (diagnostic) → ↑ Na+ and H2O loss in sweat (Dehydration)
Consequences/Presentation in each organ:
Lung *Note: lung is more common cause of death, ↓ lifespan (35-45)
Thick mucus in lungs → Recurrent pulmonary infections and mucus plugging → Hyperinflated lungs with productive cough
Infxn in child: S. aureus
Infxn in adults: Burkholderia Cepacia & P. aeruginosa (bc thick mucus allows for biofilms)
Bronchiectasis, ABPA, Nasal Polyps (child), Digital clubbing
Thick mucus in pancreatic and bile ducts → ↓ Pancreatic and biliary secretions → ↓ Fat / Fat-soluble vitamin (ADEK) absorption
Chronic pancreatitis, Steatorrhea (fatty stools), CF-related diabetes
Thick mucus in stool → Thick/sticky meconium (1st poop) → Inspissated mass gets stuck in ileum → Meconium ileus in newborns (small bowel obstruction)
Pancreatic enzyme replacement
Lumacaftor (improves protein misfolding and trafficking) + Ivacaftor (enhances Cl- flux through channel)
"Pneumoconiosis
Basics?
4 types (occupations, imaging/histology & consequences)? ABCs"
"Basics:
Occupationally acquired through inhaling dusts → Presents many years after inhalation
Dust particles inhaled into alveoli → Alveolar macrophage phagocytosis → Cytokine release → Inflammation and fibrosis
Subtypes:
Asbestosis
Occupation: Hx of roofing, shipbuilding, house insulation, plumbing
Inhalation of asbestos fibers → Affects lung + pleura
Lung → Lower lung lobe fibrosis, bronchogenic carcinoma
Pleura → Calcified pleural plaques, pleural effusions, mesothelioma (less common than bronchogenic carcinoma)
Ferruginous bodies: Golden fusiform iron-coated fibers found in asbestos lesions
Hypersenstivity Pneumonitis
Cause & course?
Comparison to other disorders?
Classic case?
Diagnosis?
Treatment?
"Hypersensitivity (mixed III/IV) reaction to environmental antigens (mold, bacteria, agricultural particles)
Chronic: Non-caseating granuloma formation and fibrosis
Classic case: Farmers (moldy hay) or bird-fancier (Avian proteins)
Acute: Inflammation causes dyspnea, cough, fever
Differentiating from other disorders:
Idiopathic Pulm Fibrosis
Both slowly develop firbosis but in hypersensitivity pnueomonitis we see BOTH fibrosis AND non-caseating granualoma
Pneumoconiosos
Hx: Farmer or bird fan VS coal miner, aeorspace worker, beryllium miner, roofing & sandblasting
Timeline: Inflammation occurs acutely in hypersensitivity vs pneumoconiosis inflammation will not show up until many years after inhalation
Diagnosis: Bronchoalveolar lavage (BAL) - Saline in airways & alveoli --> recollect fluids & analyze --> + if reveals leukocytes
Treatment: Avoid exposure to antigen"
Aortic Regurgitation
Acute & Chronic
Heart failure
Murmur & location? Murmur intensity (preload, afterload & inspiration/expriation)
Presentation
Causes (3)
"Acute: Poor compensation due to rapid physiologic changes (Ex. Cause: Aortic dissection)
Chronic: Allows for heart remodeling --> regurgitant blood into LV --> Increased LVEDV --> eccentric hypertrophy (to be able to hold increased volume) --> systolic heart failure --> S3 heart sound
Murmur: Early decrescendo diastolic murmur @ Erb's point (L 3& 4th intercostal space) + Loud S3 (from blood rushing)
Intensity: Increases w/ preload & increases w/ afterload and expiration
Presentation: (1) Increase pulse pressure (bc LV needs to shoot out way more blood to compensate for all the blood that comes back so increased SBP but only some blood reaches the arteriole so DBP stays ~ the same
(2) ""Water hammer"" pulse bc rapid upstroke & head bobbing (3) Exertional dyspnea & pulmonary edema
Causes: (1) Age related aortic valve sclerosis most common cause (2) Bicuspid aortic valve - fusion of two aortic leaflets in younger patients; increased risk of dystrophic calcification to valve (3) Aortic dilation secondary to aortic dissection, aortic aneurysm, connective tissue disease and/or teriary syphillis "
Potential Locations
Origina/Derivative
Associations
Presentations (w/ & w/o PDA)
Imaging
Management
Aortic Stenosis
Murmur, location & what increases intensity?
Unique Ft
Cause
HF
"Murmur: Holosystolic harsh crescendo-decrescendo @ 2nd R ICS (aka where you hear aortic) + S4 (from blood hitting thick wall) radiates to carotids
Increased by: Increased preload, decreased afterload, & expiration
Causes:
(1) Dystrophic calcification (in older pts)
(2) Bicuspid Aortic valve (younger pts)
Heart Failure: Diastolic HF --> LV cocentric hypertrophy (bc have to use increased preasure
Presentation:
(1) Triad
- Exertional dyspnea
- Angina
- Syncope
Weak bc lil blood is going to the aorta & late bc it takes longer for LVP to get higher than aortic pressure
(3) Single, soft S2
"
Mitral Stenosis
Murmur: Location & how to increase intensity
Presentation
Cause
Origin & cause?
Murmur?
Assocations?
Murmur: Harsh holosystolic murmur @ Left LSB
*Note: With increased severity, murmur decreases (bc bigger hole)
Assocations: (1) Down syndrome
Acute vs chronic?
Murmur & Increase in intensity?
Presentation?
Associations?
Murmur - location & increasing sound
Associations
Complications
Hypertrophic Obstructive Cardiomyopathy (HOCM)
Cause & Genetics
Murmur (Including location & what increases the intensity)
Histology
Management
"Presentation
Sudden cardiac death while relatively young
Cause
Genetic mutations in sacromeres (B myosin heavy chain & myosin binding protein G)
Autosomal dominant
Dynamic LV outflow tract obstruction bc cocentric hypertrophy @ septum (dynamic bc if we fill it w/ a lot of blood, this will ush on septum & move it over --> easier to eject blood)
Murmur: Systolic crescendo-decrescendo at LLSB
IF condition creates mitral regurgitation, holosystolic murmur @ apex & S4 sound
Incearsing murmur: Decreased preload (keeping volumes high helps with correcting) *functional mitral regurgitation
Histology:
(1) Myofibrillary disarray --> swirls & clusters
(2) Interstitial fibrosis --> the white spaces
Management:
(1) Avoid dehydration & strenuous exercise
(2) B blockers to decrease HR & contractility (decreased HR means more time for diastolic filling)
"
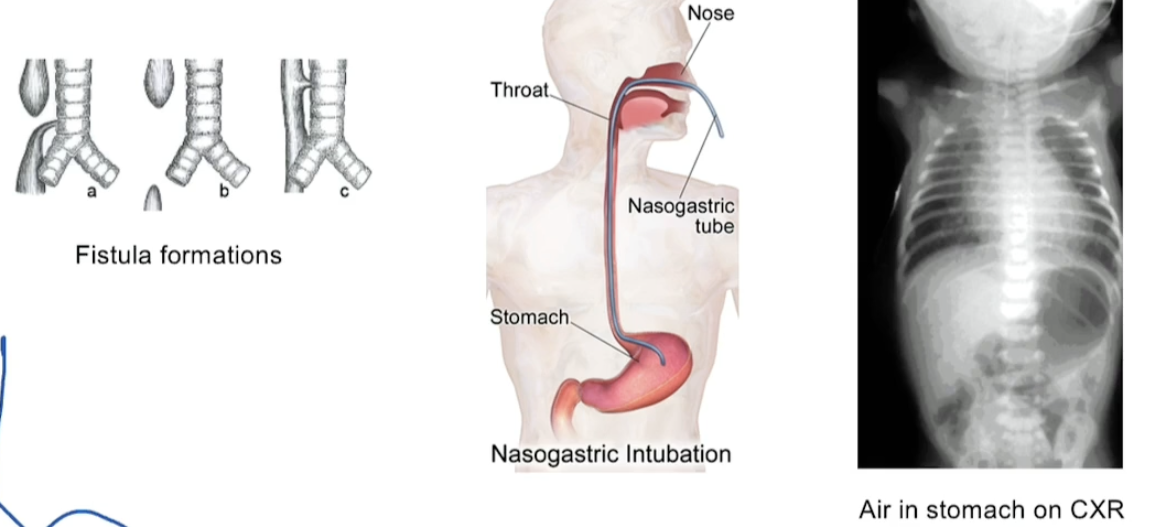
Murmur
Associations
CXR
Tracheoesophageal Fistula
"From embryonic stage (recall lung bud derives from foregut)
Sx
cant pass NG tube
polyhydraminos (bb cant swallow fluid so it builds up)
Drooling, vomitting, choking on 1st feed
Air in stomach on CXR
Perfusion vs Diffusion
"
"
Restrictive Lung Disease
What happens to RV, FRC & TLC?
FEV1/FVC
How do pts breathe?
Restrictive Lung Disease Classification
Dysfunctional breathing mechanisms
________
________
Interstitial Lung Disease
______
______
______
""
Idiopathic Pulomonary Fibrosis
Onset?
Sx?
Dx? How do CXR & CT look?
Pathogenesis?
Drugs & Radiation Induced Fibrosis
"
"
Lung Cancer Basics
What are the two classifications?
CXR?
Presentation
Associated Complications of Lung Cancer (think: What structures are around the lung?)
_______
_______
_______
_______
_______
_______
""
Adenocarcinoma
Most common in what population?
Location?
What type of tumor? What does it produce?
EM?
Mutations?
"A leg of A is short & blunted like microvilli on EM
Think: Since it's not smoking, must be something else like mutations"
What is a DVT?
- Associated triad?
- Presentation?
- Diagnosis (3 things, including a high yield PE test)
- Presentation?
- Diagnosis: What does this look like on CT? V/Q perfusion scan?
- EKG?
Pleural Effusion
What causes it?
Presentation? (tracheal shift? CXR? Sx?)
Etiologies (3)
1 procedure for diagnosis (how do we interpret results?)
""
Acute Respiratory Distress Syndrome (ARDS)
Presentation
Underlying etiology - damage to lung. How?
(1)
(2)
Pathogenesis
Diagnosis (what do we see on CXR?)
Management
Neonatal Respiratory Distress Syndrome (NRDS)
Presentation
Risk factors
Management
Internal Capsule
- Blood supply?
- What are its 3 parts?
Blood supply: Lenticulostriate Arteries (group of small arteries coming MCA)
The internal capsule is a collection of white matter (axons) divided into 3 parts:
Anterior Limb
Ascending sensory fibers: Thalamocortical tracts
Posterior Limb
Descending motor fibers: Corticospinal tract
Ascending sensory fibers (but seperate from motor therefore, you can have a pure motor stroke in posterior limb OR pure sensory stroke in either the anterior or posterior): Thalamocortical and somatosensory tracts
Genu
Descending motor fibers: Corticobublar Tract
Spinal Nerves & Cord
- How many spinal nerves are there? How are the spinal nerves separated/classified?
- How do the spinal roots exit in relation to the vertebra?
- Where does the spinal cord terminate in adults? What is the anatomical landmark for this?
There are 31 spinal nerves.
8 cervical
12 Thoracic
5 Lumbar
5 Sacral
1 coccygeal
C1-7 exit above & C8 and caudal exit below. They exit laterally through the intervetebral foramina.
Spinal coot terminates at L1/L2. We use the illiac crest to anatomically mark L4 which is where we would do a lumbar puncture
Tetanus
What is the organism? Gram + or -? Aerobic or anerobic?
What is the toxin relseased? And where does it travel? How?
What is the mechanism of action? What neurotransmitter is involved?
Typical presentation?
Tx?
"
Organism: Clostridium Tentii --> Gram + spore forming anerobic bacteria
Note: Spores are heat & chemical degredation resistant
Toxin: Tetanospasmin toxin travels retrograde to the CNS via Dysein
Mechanism of action:
Tetanospasmin travels --> Renshaw cells (which usually regulate motor neuron activity) in spinal cord
Toxin cleaves snares proteins on vesicles carrying glycine such that they cannot release glycine & GABA into synaptic cleft
a-motor neurons unregulated --> unregulated contractions
Presentation
Typical pt: Unvaccinated, person who had a lacteration recently OR baby delivered by midwives
Baby sx: foul smelling umbilical stump
Other sx:
Risus sardonicus (sneering grin)
Spastic paralysis --> can lead to respiratory
Trismus (lock jaw)
Opsithotonos (sponal muscle spasms --> causes the back to arch)
Treatment:
Wound debrivment --> remove tissue that may have spores or toxin
"
Rabies
Organism?
Mechanism of action? Incubation period? Where does it travel to? How?
Reservoir
Worldwide: ________
US: ___________
Clinical signs & symptoms (ONE super high yield)
Organsim: Rabies virus
Mechanism of action:
Virus binds to acetylcholine nictonic receptor & enters motor neurons
Retrograde travel to brain via dynein --> encephalitis
Reservoir
Worldwide: Dogs
US: Bats (but also racoons, skunks, etc.)
Clinical signs & symptoms
Very general sx; nonspecific
Hydrophobia (foaming at mouth at the sight, thought or sound of water can trigger painful spasms in the throat & larynx)
Flacid paralysis
CN V
Name & Name of Branches:
High yield facts
Where is the nucleus?
Function
Sensory to
Sensory to
Motor to
Where does it travel?
Reflexes
Afferent & efferent of
Affterent for ___ & ____
Etiology of Lesions
(1)
(2) Infxn
(3)
Presentation
What would a leision to each cause?
Compression leisions vs ischemic and/or demyelinating
"
Name & Name of Branches: Trigeminal Nerve
V1: Opthalmic Nerve
V2: Maxillary Nerve
V3: Mandibular Nerve
High yield facts
Nucelus at lateral pons
Function
Sensory to V1, V2, & V3 areas
Sensory to anterior 2/3 of the tongue
Motor to muscles of mastication
Where does it travel? (see below) ""Standing Room Only""
V1 --> superior orbital fissure
V2 --> Foramen rotundum
V3 --> Foramen Ovale
Reflexes
Afferent & efferent of jaw reflex
Affterent for corneal reflex & lacrimation reflex
Etiology of Lesions
(1) Trigeminal Neuralgia (tx with carabmazepine)
(2) Herpes zoster Ophtalamicus if V1
(3) Foraminal Leisons or TMJ dysfunction
Presentation
V1: Loss of sensation to V1 area/ afferent for corneal reflex & lacrimation reflex
V2: Loss of sensation to V2
V3: Loss of sensation to V3, anteriro 2/3 of tongue, loss of jaw reflex & ipsilateral paralysis in muscles of mastication
"
CN XII
Name:
High yield facts
Where is the nucleus?
Where does it pass through?
Function
(1)
Unique charcateristic: ONLY CN with
Etiology of Lesions
(1)
(2)
Presentation
(1) Supranuclear Injury:
(2) CN XII injury:
CN VIII
Name:
High yield facts
Where is the nucleus?
Function
(1)
Where does it traverse?
Etiology of Lesions
(1)
(2)
(3)
Presentation
(1)
(2)
(3)
(4)
Name: Vestibulocochlear Nerve
High yield facts
lateral pons & lateral medulla
Function
(1) Hearing & balance & equilibrium
Where does it traverse: Internal acoustic meatus
Etiology of Lesions
(1) Bilateral acoustic Neuromas aka vestibular schwanomas (neurofibromatosis type 2 on chromosome 22)
(2) Temporal Bone Trauma
(3) Basilar skull fracture
Presentation
(1) Loss of balance; vertigo
(2) Sensorineural hearing loss
(3) Basilar skull fracture --> Raccoon eyes (blood pooling behind ear)
(4) Horizontal nystagmus
Poliomyelitis
Organism?
Where is it most common?
What does it affect?
Presentation? (Ex. typical pt & sxs. UMN or LMN?)
Disease course
CSF?
Chicken Pox/ Shingles
Causative organism
Disease course
Presentation (Including typical pt)
Relevant Variants (2 that concern us)
Treatment
Neurosyphilis
Recall syphilis progression
Causative organism
Presentation
Typical pt
Typical sx
Eye findings
Werdnig-Hoffman Disease aka Spinal Muscular Atrophy Type I (SMA Type I)
Cause
Presentation (how does it differ from polio)
Genes/Inhertiance
Muscle biopsy
Cause: Apoptosis on ventral horn cells
Presentation:
Onset between 0-6 month of age, death by 2 yrs old
LMN like Polio. Presents in babies like
Weak cough, difficulty swallowing or missing milestones like note being able to hold their head up
Unlike flaccid paralysis in Polio, no ascending paralysis & symmetric --> goes to proximal muscles right away
Cranial nerves classically spared (ex. normal eye movements etc.)
Genes/Inheritance: AR; SMN1 gene, chromosome 5
Muscle biopsy: muscle unit atrophy
What are the steps?
What are two things you really need to get neurotransmitter in synaptic cleft & trigger an AP in the post synaptic cell
Pesticides & Sarin Gas
Category
Mechanism
Tx
- Classification: Organophosphates
- Mechanism: Irreversible inactivion of acetylcholinesterase --> Means Ach will remain in the synaptic cleft so while bind to:
- Cholingeric receptors (more parasympathetic; more secretions)
- D iarrhea/ Diaphoresis
- U rination
- M iosis
- B radycaria
- E mesis
- L acriation
- S alivation
- Muscarinic recptors
- Excessive stimulation leads to inactivation --> muscle weakness --> paralysis (including of diaphragm)
- Tx:
- 1st take off clothes (which may still be contaminated)
- 2nd give Atropine (but this will only prevent muscarinic sx) so add 2PAM aka Pralidoxime which helps regenerate Ach
Edrophonium
Pyridostigmine
Classification
Mechanism
Short acting vs long acting + purpose? (what diagnostic test is particularly relevant)
Side effects
- Classification: Acetylcholinesterase inhibitor
- Mechanism: Inhibits acetylcholinesterase temporarily
- Purpose
- Edrophonium: Short acting, used for diagnosis
- Pyridostigmine: Long acting, used therapeutically
- Side effects:
- D iarrhea
- U rination
- M iosis
- B radycardia
- E mesis
- L acrimation
- S alivation
Phenytoin
Classification
Mechanism
Carbamazepine
Classification
Mechanism
Common uses
Gabapentin
Classification
Mechanism
Levetriacetman (aka Keppra)
Classification
Mechanism
Pupillary Light Reflex
What is pathway?
What test is used to assess pupillary light reflex?