cellular adaptations and cell death
1/38
Earn XP
Description and Tags
week 2 ctb
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
homeostasis
cells must survive with a tight set of parameters
pH
temperature
oxygenation
changes to these parameters can lead ot loss of homeostasis
cells may adapt
cells may die
if capacity to adapt is exceeded, injury occurs
reversible to a point
irreversible injury leads to cell death
proliferative capacity of cells
permanent cells
non proliferative
terminally differentiated
stable cells
usually non proliferative
capable of proliferating if required
labile cells
proliferative
continuously dividing
adaptive changes
hypertrophy
hyperplasia
atrophy
metaplasia
hypertrophy
increases in individual cell size
gain of cellular substance
as a result of increased functional demand
as a result of specific endocrine stimulation
hypertrophy-pathological
pathological hypertrophy of heart
in response to increased haemodynamic loads
heart muscle enlarged
compromised myocardial blood supply can lead to:
reversible injury
irreversible injury + cell death
hyperplasia
increase in cell number
physiological- uterine endometrum
pathological: BPH
physiological hyperplasia
hormonal hyperplasia
glandular epithelium of breast in puberty/pregnancy
compensatory hyperplasia
residual tissue grows after removal/loss of part of an organ
atrophy
decrease in cell size
loss of cellular substance
atrophy in sufficient cell number- organ atrophy
causes:
decreased workload
diminished blood supply
loss of endocrine stimulation
ageing
metaplasia
change in cell type
one adult cell type replaced by another cell type
an adaptive response
normal protective mechanisms may be lost
cell function often compromised
dysplasia
abnormal development of cells within a tissue or organ
failure of normal development
features include:
nuclear enlargement
loss of nuclear polarity
increased cell division
neoplasia
a mass formed by autonomous proliferation of cells that persists after cessation of the stimulus that provoked the change
compared with normal cells, neoplastic cells have disordered phenotype, function and behavious
benign neoplasms show least cytological variation from parent tissue and do not invade surrounding structures
malignant neoplasms show substantial cytological changes- invade surrounding tissues and are harmful
causes of cell injury
hypoxia/ischaemia (oxygen deficiency, redued blood supply)
genetic defects (mutations causes LOF of GOF or faulty proteins)
physical agents (trauma, extremes of temperature, radiation)
toxins (pollutants, insecticides, CO)
infection (viruses, bacteria, fungi)
nutritional imbalances (specific vitamine deficiencies)
immunologic reactions (autoimmune reactions, chronic inflammation)
mechanisms of cellular injury
membrane destruction
protein denaturation
disrupt metabolic processes
DNA damage
hypoxia/ischaemia
reduction in level of oxygen available/inadequate blood supply
lack of oxygen limits aerobic respiration
inadequate ATP leads to reduction in cellular function
due to inadequate oxygen supply or inadequate oxygen delivery
ischaemia leads to loss of nutrient delivery and build up of toxins
due to embolism or systemic cardiac failure
chemicals and drugs
simple chemicals
glucose
salt
damage electrolyte and fluid balance
poisons
arsenic
cyanide
mercury
frequent exposure to:
CO
pollutants
alcohol
therapeutics
infectious agents
bacteria
viruses
parasites
particularly significant in cases of:
immunocompromisation
malnutrition
physical
divided into:
mechanical trauma
shape of colliding object
force of collision
site of injury
thermal injury
burns
hyper/hypothermia
electrical injury
low/high voltage current
injury produced by ionising radiation
x rays
sustainable healthcare
climate change: global cause of environmental disease
WHO estimates 250000 deaths between 2030 and 2050 due to climate change
CV, cerebrovascular diseases
food/water borne infectious diseases
vector-borne infectious diseases including malaria and dengue
malnutrition
nutritional
dietary insufficiency- injury at cellular level due to interference in normal metabolic pathways
dietary excess- abnormal conc of molecules that may affect metabolic pathways
scurvy
vit C deficiency
ascorbic acid is involved in a number of biochemical reactions
involved in collagen synthesis
deficiency results in impaired wound healing, defective tooth formation, impaired osteoblast function
cellular response to stress and injury
response to injury commonly results in activation of response pathways
integrated stress response
unfolded protein response
autophagy
can trigger cell death
integrated stress response
intracellular signalling pathways
modulate gene expression and protein synthesis
adaptation to cell injury
activated by stress sensing kinases
results in cell survival, recovery, restoration of homeostasis or cell death
unfolded protein response
accumulation of misfolded proteins in the ER
results in:
increased production of chaperones
enchance degradation of abnormal proteins
slows protein translation
ageing
viral infections
neurodegenerative disorders
autophagy
cell eats its own contents
cytoplasmic materials delivered to lysosome for degradation
survival mechanism for nutrient deprivation
cell death: apoptosis
programmed cell death
activation of specific genes
pathologic or physiologic
no inflammatory response
usually single cells
membrane integrity retained
cell shrinkage and formation of apoptotic bodies
cell death: necrosis
pathologic
cell disintegrates
inflammatory response
groups of cells
membrane integrity lost
cell swelling and lysis
necrosis
accidental cell death
severe injury to many cellular components
severe mitochondrial damage
rupture of lysosomal and plasma membranes
local inflammatory response
main causes: ischaemia, microbial toxins, burns, chemical and physical injury
types of necrosis
coagulative necrosis
liquefactive
caseous
fat
fibrinoid
coagulative necrosis
architecture of dead tissue preserved for some days
firm texture
injury denatures structural proteins and enzymes
proteolysis blocked
necrotic cells eventually broken down by lysosomal enzymes from infiltrating leukocytes
liquefactive necrosis
digestion of dead cells
transformation of tissue to viscous liquid
bacterial or fungal infections
pus
caseous necrosis
tuberculosis
cheese-like appearance
fragmented or lysed cells
granular debris enclosed within a collection of macrophages
fat necrosis
focal areas of fat destruction
release of activated pancreatic lipases
acute pancreatitis
fibrinoid necrosis
vascular damage
antigens and ABs deposited in artery walls
apoptosis
precise set of molecular pathways
defined genes and biochemical pathways
once initiated, it’s irreversible
serves to eliminate cells with intrinsic abnormalities
promotes clearance of cell fragments without inflammatory reaction
physiological apoptosis
removal of cells during development
involution of hormone dependent tissues
cell turnover in proliferating populations
death of cells that have ‘served their purpose’
pathologic apoptosis
DNA damage
misfolded protein accumulation
infections
atrophy due to obstruction
morphologic changes during apoptosis
cell shrinkage
chromatin condensation
cytoplasmic blebs and apoptotic bodies
phagocytosis
mechanism of apoptosis
results from activation of enzymes called caspases
pro-enzymes
activated by
mitchondrial (intrinsic pathway)
death receptor (extrinsic pathway)
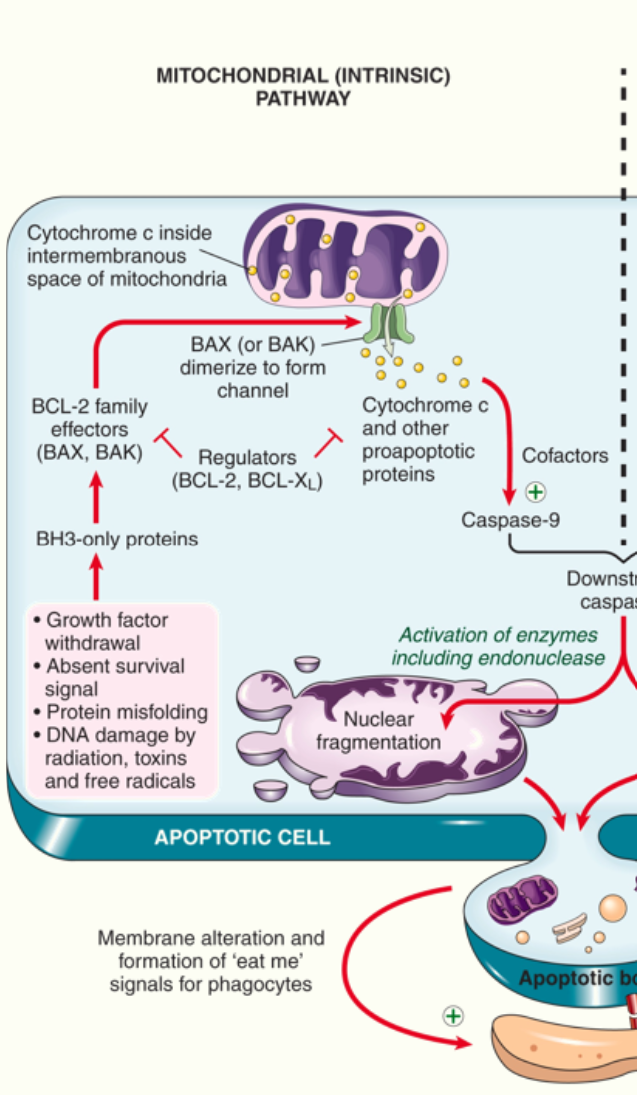
intrinsic pathway: mechanism of apoptosis
mitcohondria contain proteins that can induce apoptosis: cytochrome C
anti-apoptotic proteins maintain mitochondrial membrane integrity
deprivation of survival signals leads to dimerisation of pro-apoptotic factors BAK and BAX
BAK and BAX dimerise and insert into mitochondrial membrane, forming channels
permeabilisation of mitochondrial membrane releases cytochrome C
caspase activation is triggered, leading to apoptosis
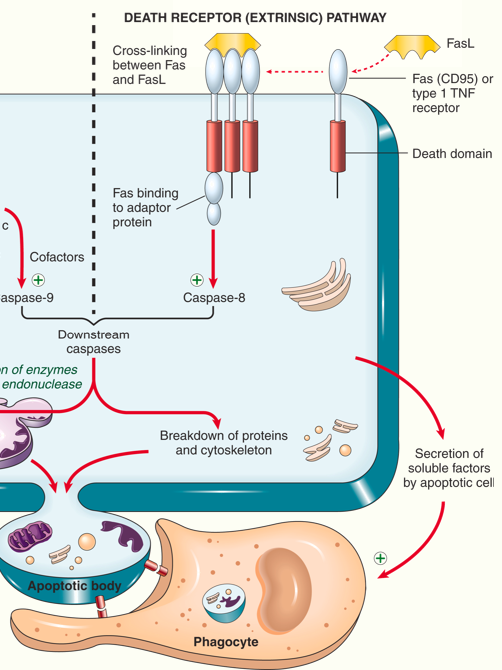
extrinsic pathway: mechanism of apoptosis
death receptors on cell surface are capable of triggering apoptosis
members of the tumour necrosis family containing death domains
Fas is a prototypic death receptor
Fas ligand (FasL) is expressed on activated T lymphocytes
recognition of Fas-expressing cells leads to crosslinking of Fas and binding of adaptor proteins
caspase activation