CHAPTER 2: DEFINITION OF TERMS / PATIENT INTERVIEW
1/56
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
57 Terms
patient interview
the first and often the most important step in effective di- agnosis and treatment planning.
demographic informa- tion should be obtained and recorded
Patient’s full name, and how he or she pre- fers to be addressed, for example, Mrs, Ms, first name, etc. If the name is unusual, a phonetic spelling to assist in correct pro- nunciation at the initial interview can be very helpful.
Address and telephone number(s).
Age, sex, and race. Although this informa- tion is routinely included in patient ques- tionnaires, it may be more prudent to house it in the medical history instead of the de- mographic form, emphasizing its need for legitimate patient care purposes.
Occupation.
Marital status.
Party to contact in case of emergency.
Third party involvement, if any, such as private insurance, Government benefit programs, and the like.
Responsible party: when dealing with a minor child, or legally disabled adult, it is critical to ascertain who can give consent for treatment, and who will be responsible for payment of fees. Divorce, remarriage, and all the complications of modern fam- ily life can make this question at once both difficult and absolutely essential to answer before proceeding very far
Corah Dental Anxiety Scale
A standardized instrument used during the course of the initial interview
one tool to measure and confront patient’s fears.
Using the scale: the questionnaire is scored by adding the total score for the four items, responses ‘a’ to ‘e’ valued 1 to 5 respectively.
A score of 20 indicates very high anxiety, whereas a score of 4 would indicate no anxiety.
If the patient scores 12 or less and doesn’t mark ‘e’ on any item, no follow- up is recommended; however, any ‘e’ response even if the total is 12 or less should be noted and followed up verbally, to identify and deal with that concern.
If the patient scores 13 or 14, suggesting an anxious patient, they should be asked about their dental experiences with an emphasis on what you can do to make them most comfortable.
Again, any ‘e’ response should be noted and followed up verbally, to identify and deal with that concern.
A score of 15 or higher suggests a highly anxious patient.
A digression from the interview is indicated to explore the source of the anxiety, encouraging the patient to recount and confront old experiences, to admit fears, and to suggest ways to relieve anxiety about future care.
medical issues that must be addressed in the dental environ- ment
PATIENTíS GENERAL HEALTH
ALLERGIES AND SENSITIVITIES
SYSTEMIC DISEASES
ISSUE OF PAST DISEASES, CONDITIONS, AND TREATMENT
issues may have significant den- tal implications
Malignant and/or non-malignant tumors.
Radiation therapy.
Artificial or prosthetic joints.
Use/abuse of tobacco, alcohol, narcotics,
or other illicit drugs.
Other past medical conditions, especially
those requiring hospitalization and/or sur-
gery.
Pregnancy issues
conditions under endocrine systemic disease
arthritis, diabetes, thyroid problems
conditions under Respiratory systemic disease
asthma, tuberculosis, shortness of breat
conditions under Cardiac systemic disease
heart disease, rheumatic fever, heart murmur, heart valve problems, pacemaker, high blood pressure, chest pains, swollen ankles
conditions under Blood: systemic disease
abnormal bleeding, anemia, transfusions, fatiguability
conditions under Gastrointestinal/genitourinary: systemic disease
jaundice, hepatitis, liver disease, contact with HIV or AIDS virus, sexually transmitted disease, kidney dis- ease
conditions under Central nervous system: systemic disease
epilepsy, fainting spells, nervous disorder/psychiatric care
ROUTINE SYSTEMIC APPROACH
Doing examination and diagnosis the same way every time (routine) and in a logical order (systematic) saves a great deal of time while avoiding serious omissions and mistakes in the process
DATA GATHERING
Refers to the comprehensive collection of bits of information about the patient through interview, history, examination, and other aids.
PATIENT HISTORY
Consists of all information given to us by the patient
EXAMINATION
includes all additional methods used by the dentist beyond the interview and history, such as radiographs, clinical examination, and other diagnostic aids and modalities
TYPES OF EXAMINATION
EMERGENCY EXAMINATION
SCREENING EXAMINATION
COMPREHENSIVE EXAM
TRIAGE
EMERGENCY EXAMINATION
include basic patient information, a good health history, and only the dental history necessary to assess the chief complaint being addressed as an emergency
ex: those that have wound near the head/brain
SCREENING EXAMINATION
When large numbers of people are to be treated in, for example, an institutional setting, screening examinations are often employed as a means of triage to allocate time and resources efficiently
ex: during dental/medical missions
COMPREHENSIVE EXAMINATION
Given the appropriate setting and adequate time, the comprehensive examination is employed to gather ALL the relevant data about a dental patient.
triage
This is a concept developed by the military for dealing with multiple casualties most effectively
used in ER to identify who needs immediate care and who can wait
triage categories: emergency
those with emergency signs require immediate emergency treatment
a life-threatening medical condition
expect to receive immediate attention
triage categories: priority / very urgent
those with priority signs should be given priority in queue for rapid assessment
a serious medical condition
expect attention after red patients have been stabilized
triage categories: urgent
expect attention after red and orange patients have been stabilized
triage categories: non-urgent / routine
those who have no emergency or priority signs are non-urgent cases and can wait their turn for assessment and treatment
can function without immediate care and will be attended to as soon as possible
category 1
resuscitation
ex: heart attack, major car accident
immediate (seconds)
category 2
emergency
ex: severe blood loss, overdose
within 10 mins
category 3
urgent
ex: head injury (conscious), breathing difficulties, infection
within 30 mins
category 4
semi-urgent
ex: sprained ankle with possible fracture, eye inflammation
within 1 hr
category 5
non-urgent
ex: cut not requiring stitches, common cold
within 2 hrs
techniques of examination
inspection
palpation
percussion — blunt end of mouth mirror, tap
auscultation —stethoscope; checks crepitus
olfaction — often overlooked; sense of smell
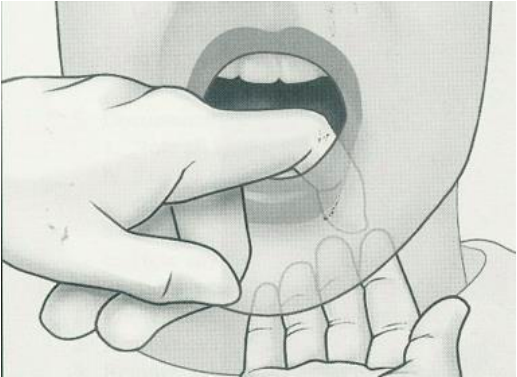
types of palpation
bi-manual palpation
bi-digital palpation
bilateral palpation
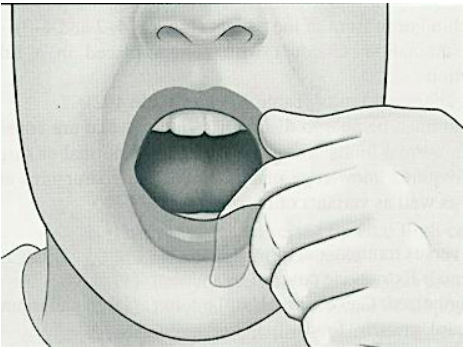
digital palpation
bi-manual palpation
Uses both hands on the same structure (one inside, one outside)
checks the floor of the mouth
Digital palpation
Uses index finger (detect presence of exostosis on the mandible)
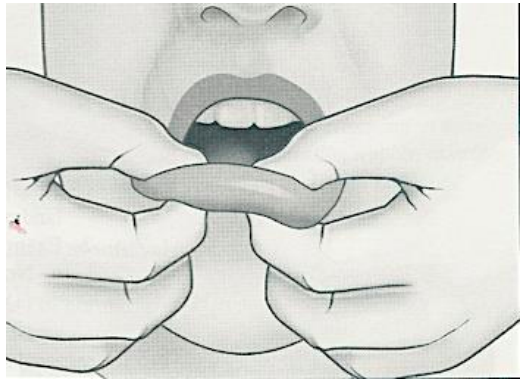
bi-digital palpation
Uses finger and thumb of same hand
use of two fingers either of the same hand or 1 finger from each hand
(palpate the lips)
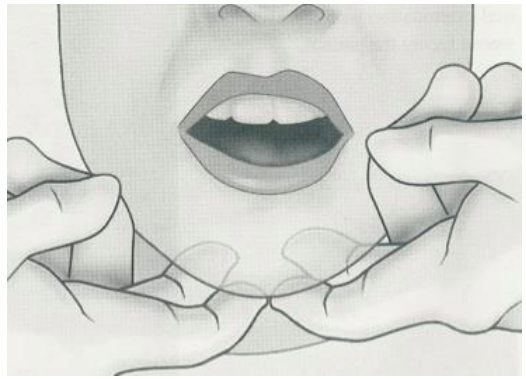
bilateral palpation
Use both hands at same time to examine structures on opposite sides (examine submental nodes)
palpates the left and right side of a patient’s body
checks clicking
FINDINGS
All bits of information obtained in the history and examination process
may be normal or abnormal, healthy, or pathologic
CHIEF COMPLAINT
It is the reason, usually a symptom or cluster of symptoms, why the patient seeks treatment.
It can be urgent, such as acute pain or gross swelling, or minor, such as a small chip on a tooth, which has been present for some time.
complain — the action
complaints — ang unod sa complain; gist
symptoms
subjective, elicited by history and interview, as described by the patient
ex: pain, sensitivity to hot/cold, altered taste, inability to chew or to speak clearly, esthetic complaints
signs
objective, often measurable, discovered by examination)
Obviously, some overlap is possible
ex: redness, swelling, measurable, fever, tenderness to palpation, crepitus, bad breath, molar crossbite
SOAP
subjective
objective
assessment
plan
NORMAL
Refers to the most typical or ideal value/condition.
Often a single expected value or description.
Represents what is commonly observed in healthy individuals.
—what might be normal to one, might not be normal to the other one!!
RANGE OF NORMAL
Refers to the acceptable limits around the normal value.
Accounts for physiologic differences among individuals.
Values within this range are still considered healthy.
variation of normal
usually structural, anatomical, developmental differences.
refers to individual differences that deviate from the ideal normal
but do not indicate disease or pathology.
ex: Peg-shaped lateral incisors, Diastema in mixed dentition
Pain or discomfort
the most common chief complaint and should always be given weight in the diagnosis.
different types of DIAGNOSIS
snap
TENTATIVE OR WORKING
DIFFERENTIAL
MULTIFACTORIAL
DEFINITIVE OR FINAL
SNAP diagnosis
Made quickly and on the spot, it can be a perfectly good diagnosis
ex: A patient returns 3 days after removal of a lower third molar complaining of pain and a bad taste and exhibiting inflammation and odorous discharge at the extraction site.
TENTATIVE OR WORKING diagnosis
A little more precise than the ‘snap’ diagnosis, this type of assessment assumes that the clinical picture ‘fits’ a given disease state, so that preliminary treatment may proceed, or other diagnostic tests may be selected.
ex: An ulceration under a partial denture flange of which the patient has been unaware may simply be an inflammatory response to irritation.
DIFFERENTIAL diagnosis
This refers to the process which, given a set of findings (signs and symptoms), the clinician categorizes that information into data relevant to making a diagnosis, and develops a list of the most likely diseases or disorders consistent with the findings
MULTIFACTORIAL diagnosis
Aka: Problem List
isuwat tanan problema
This is aimed at addressing the problems so as to provide maximum comfort, function, and esthetics, with the goal of long-term retention of the natural dentition.
DEFINITIVE OR FINAL diagnosis
Using the differential process just described, the definitive or final diagnosis is derived, and appropriate treatment rendered. If the disease fails to respond, it may be necessary to backtrack on the differential diagnosis and try again.
In the case of soft tissue diseases, microscopic examination of tissue samples at the cellular level often determines the final diagnosis. Blood dyscrasias or diseases provoking an immune response may be proved serologically. Not all problems can be solved so neatly, however, because the range of abnormal is as wide as that of normal.
different types of treatment plan
emergency
prevention-oriented
patient-oriented
comprehensive
emergency treatment plan
Immediate treatment plan
This addresses the definitive diagnosis directly, and must generally be instituted at once.
prevention-oriented treatment plan
If in our diagnosis we have successfully identified etiologic factors, then they can be addressed in the treatment plan.
no concept of the disease yet, just prevention: oral prophylaxis, pit/fissure sealtant
patient-oriented treatment plan
aka: humanistic or holistic approach
means working from our patients’ frame of reference and involving them in the entire process
comprehensive treatment plan
This derives from a problem list diagnosis, and may be safely postponed if necessary, or carried out in stages over time.
PROGNOSIS
forecast
prediction as to the future outcome of a disease made with or without therapy
REFERRAL
refers to sending a patient to another health professional for further consultation, treatment, or co-management