Drugs & Pregnancy, Contraception
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
GPA is the abbreviation for a woman’s obstetric history
G / gravida =
P / para =
A or Ab / abortus =
Ex: If patient has had 4 pregnancies, 3 births, and 1 miscarriage =
# of pregnancies
# of births of viable offspring
abortions
G4, P3, A1
TRIMESTERS
+development
1st trimester =
2nd trimester =
3rd trimester =
w1-12 → heart, eye, ear, teeth, genitalia, brain
w13-27 → brain, CNS
w28 to end → full term
What is the daily recommendation of folic acid?
0.6 mg
DRUG PASSAGE ACROSS PLACENTA
What makes it MORE LIKELY to cross?
Lipid solubility →
Molecular weight →
Protein binding →
Degree of ionization →
lipophilic
smaller
lower binding
unionized
Drug A can cause eustachian tube defects, but the patient has failed all therapeutic alternatives. When is it safe to give?
A. First trimester
B. Second trimester
C. Third trimester
D. Not worth the risk at any time
C
(eustachian tube in the ear)
OLD FDA PREGNANCY CATEGORIES
A
B
C
D
X
MOST DRUGS ARE CATEGORY ___
human studies, NO RISK
animal studies no risk/no human studies OR animal studies risk/human studies no risk
animal studies risk/no human studies OR no human/animal studies
benefit > risk
risk > benefit
C
NEW PREGNANCY CLASSIFICATION
as of June 30, 2015 → narrative format with 3 sections
risk summary
clinical considerations
data (animal vs human)
COMMON OTC TREATED CONDITIONS
CONSTIPATION → order of rec
-
-
-
-
-
**AVOID … can induce early contractions
dietary fiber + water
bulk forming (psyllium, methylcellulose)
stool softener
osmotic
stimulant
mineral/castor oil
COMMON OTC TREATED CONDITIONS
HEARTBURN → order of rec
-
-
-
-
**AVOID ..
small, freq meals
antacids, sucralfate
H2RA (famotidine)
PPI
sodium bicarb, mag trisilicate
COMMON OTC TREATED CONDITIONS
NAUSEA & VOMITING → order of rec
-
-
-
-
small, freq meals
pyridoxine (vit B6) ± doxylamine
metoclopramide or promethazine
ondansetron
AVOID NSAIDS ______
>/= 20w
________ vaccines are contraindicated in pregnancy →
live → MMR, varicella
Vaccinations to be recommended during pregnancy →
Tdap in 3rd tri, inactivated influenza
GESTATIONAL DIABETES DIAGNOSIS
_____________ is gold standard, performed at 24-28w
A1c less reliable during pregnancy due to increased RBC turnover
Can ONLY be diagnosed in ____ or ____ trimester
If meet criteria in ___ trimester, is T2DM
oral glucose tolerance test OGTT
2nd, 3rd
1st
GESTATIONAL DIABETES TREATMENT
Non-pharm →
T2DM BG GOALS →
GDM BG GOALS →
1ST LINE MEDICATION
2ND LINE MEDICATION
Non-preferred/3rd →
plate method, 150m/wk exercise
80-130 fasting, <180 2h PP
<90 fasting, <120 2h PP
insulin
metformin
glyburide
HYPERTENSION
Treat when BP ______
Medications to use →
AVOID …
>140/90
methyldopa > labetalol > nifedipine > thiazides 2nd line
ACEi/ARB/renin inhibitors
ECLAMPSIA = preeclampsia + seizures
Treatment = _______ during and after delivery
IV MgSO4
DYSLIPIDEMIA
B/C category
C category
TAKE HOME: RISK/BENEFIT ASSESSMENT
only highest risk patients should continue therapy
BAS
omega-3 FAs
LACTATION: Relative infant dose (RID) _____ is considered CONTRAINDICATED
(dose received via breast milk relative to mother’s dose)
>/= 10%
BREASTFEEDING OLD CLASSIFICATION SYSTEM
Compatible but monitor infant for side effects →
Avoid if possible, monitor infant for side effects →
Avoid if possible, may inhibit lactation →
AVOID →
anticonvulsants, opioids
doxycycline, chloramphenicol
diuretics, estrogens
antineoplastics
LACTATION: STRATEGIES TO MINIMIZE EFFECTS
Use ______/_______ absorption
_____ half-life
Check ______ in infants
Dose daily meds ____________
Other meds ________
topical/poor oral
shortest
safety
before longest sleep interval
right after feeding
PROGESTINS
______ cervical mucus
Delay ovum, _________
Induce __________
Block ______ → inhibit ovulation
thicken
sperm transport
endometrial atrophy
LH surge
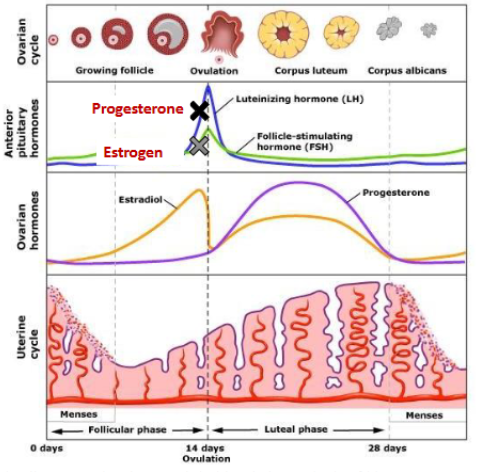
ESTROGENS
Suppress ____ release
Inhibit _______
________________ (cycle control)
FSH
ovulation
stabilize endometrial lining
PROGESTINS
Drugs + side effect profile
1st generation
2nd generation
3rd generation
4th generation
ethynodiol → norethindrone; high androgenic, slight estrogenic
norgestrel, levonorgestrel; mod-high androgenic, minimal estrogenic
desogestrel → etonogestrel, norgestimate → norelgestromin; little-mod androgenic, no estrogenic
dienogest, drospirenone; no est, and, gluco, or mineralocorticoid
Androgen effects →
Corticoid effects →
acne, +weight
fluid retention
HORMONAL CONTRACEPTIVES
**Takes _________ to adjust to changes in hormonal levels
2-3m
ESTROGEN ADEs → excess (3)
breast tenderness, +weight, irritability, depression, menorrhagia
nausea
headaches
fluid retention
ESTROGEN ADEs → deficiency (6)
breakthrough bleeding early cycle
amenorrhea
vasomotor sx
nervousness
-libido
vaginal dryness
PROGESTIN ADEs → excess (6)
breast tenderness, +weight, depression
+appetite
fatigue
+libido
alopecia
acne/oily skin
hirsutism
PROGESTIN ADEs → deficiency (3)
dysmenorrhea
breakthrough bleeding late cycle
-weight
B
COMBINED ESTROGEN+PROGESTIN (CHC) → 3
Progestin ONLY → 4
COC, patch, ring
IUD, inj, implant, POP
COMBINED HORMONAL CONTRACEPTION (CHC)
combined estrogen + progestin
*CONTRAINDICATIONS
_______ cancer
_____ days postpartum
_______ disease
____________
________ related (VTE, smoker, DM + vascular complications, etc)
____________
breast
<21
liver
migraine WITH aura
vascular
dialysis
CHC COUNSELING POINTS
_______
__________ management
No protection against ________
_______
Warnings for sx of stroke or clot (estrogen) →
adherence
missed dose
STI/STDs
ADEs
ACHES → abd pain, chest pain, headache, eye/speech problems, sev leg pain
Combined ORAL Contraceptives (COCs)
Monophasic → _____ amounts of hormones →
Multiphasic → _____ amounts of hormones →
Multiphasic less _________ and _______
consistent → 21 active + 7 placebo (usually)
varying → biphasic more breakthrough bleeding, triphasic fewer metabolic effects
premenstrual sx, dysmenorrhea
TRANSDERMAL PATCH
Xulane, Zafemy, Twirla
New patched applied _____ to abdomen, buttocks, upper torso, or upper arm
______ is patch free
If off >24h, use back up _____
NOT RECOMMENDED _____
Return to fertility →
weekly
week 4
x 7d
>90kg → Twirla BMI >30
3m
VAGINAL RING
EluRyng, NuvaRing, EnilloRing, Haloette, Annovera
______ continuous use followed by _____ ring-free
Effective anywhere in vagina, can be used w vaginal creams, no need to remove during sex, SHOULD NOT BE REMOVED ______
Return to fertility →
3w, 1w
>2-3h
3m
IUDS ARE CONTRAINDICATED IN … (2)
pelvic inflam disease
uterine abnormalities
DEPO-PROVERA INJECTABLE
medroxyprogesterone acetate
Available ___ or ___
Lasts ______
May be given up to _____ late
BBW →
AEs → 3
Return of ovulation →
IM, SQ
3m
2w
-BMD
irregular bleeding, menorrhea, +weight
10m
NEXPLANON IMPLANT
etonogestrel
Lasts ____
AEs → 2
RECOMMENDS AGAINST USE AT ______
Return to fertility
3y
irregular bleeding, headache
>/= 130% IBW
1m
PROGESTIN-ONLY PILL (POP) ADHERENCE
_________ → cannot be taken more than ____ late
_________ → cannot be taken more than ____ late
If any are taken late, recommended to use back-up contraception for ____
norethindrone, norgestrel → 3h
drospirenone → 24h
48h
DRUG INTERACTIONS CONTRACEPTIVES
_________
_________ decrease efficacy
_________ induce OC metabolism and decrease efficacy
MANAGEMENT →
antibiotics
antiretrovirals
anticonvulsants
-hormone dose, greatest risk w oral (COC/POP)
INITIATING CONTRACEPTION
Can start anything within ____ start of menses
Use barrier method of abstinence until contraceptive is effective (typically ___)
5d
7d
EMERGENCY CONTRACEPTION
ADEs: _______, bloating, menstrual cramps, headache
Use within … → Yuzpe (>100 mcg EE, 500 mcg levonorgestrel)
→ Levonorgestrel (Plan B One-Step, etc)
→ Ulipristal (Ella)
→ Paragard (copper) IUD
nausea
72h
72h
120h
5d
AR PHARMACIST CONTRACEPTIVE PROTOCOL
Must be age ____
Can only dispense ____ form
Cannot dispense more than a ____ supply until the patient has seen a provider
If patient has not been seen by a provider in the last ______, the pharmacist must provide a referral to local provider
Must provide patient with an informed ________ and standardized _______
18+
oral
6m
6m
consent form, fact sheet (Appendix E)