NURS 245 Ch. 41 part one: Disorders of Endocrine Control of Growth and Metabolism
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
62 Terms
hypofunction
underproduction of a hormone
what causes hypofunction
congenital defects; disruption in blood flow, infection, inflammation, autoimmune, neoplastic growth; decline in function; atrophy from drug therapy; receptor defects
hyperfunction
excessive hormone production
what causes hyperfunction?
excessive stimulation and hyperplasia of the endocrine gland, hormone-producing tumor on a gland
primary endocrine disorders
originate in the target gland that is responsible for producing the hormone
secondary endocrine disorders
target gland is normal, but its function is altered by defective levels of stimulating hormones or releasing factors from the pituitary system
tertiary endocrine disorders
result from hypothalamic dysfunction and both the pituitary and target organ are understimulated
releasing hormones
tell the pituitary what to release into the blood
trophic hormones
from pituitary; tell specific peripheral glands to grow and produce their hormones
adenomas are the most common cause of
pituitary disorders
adenomas effect of mass and on hormone secretion
the mass can cause pressure in the skull that causes headaches, seizures drowsiness, visual deficits. the effect on hormone secretion depends on the cells and location involved that can alter the release of hormones
direct and indirect control of hormones
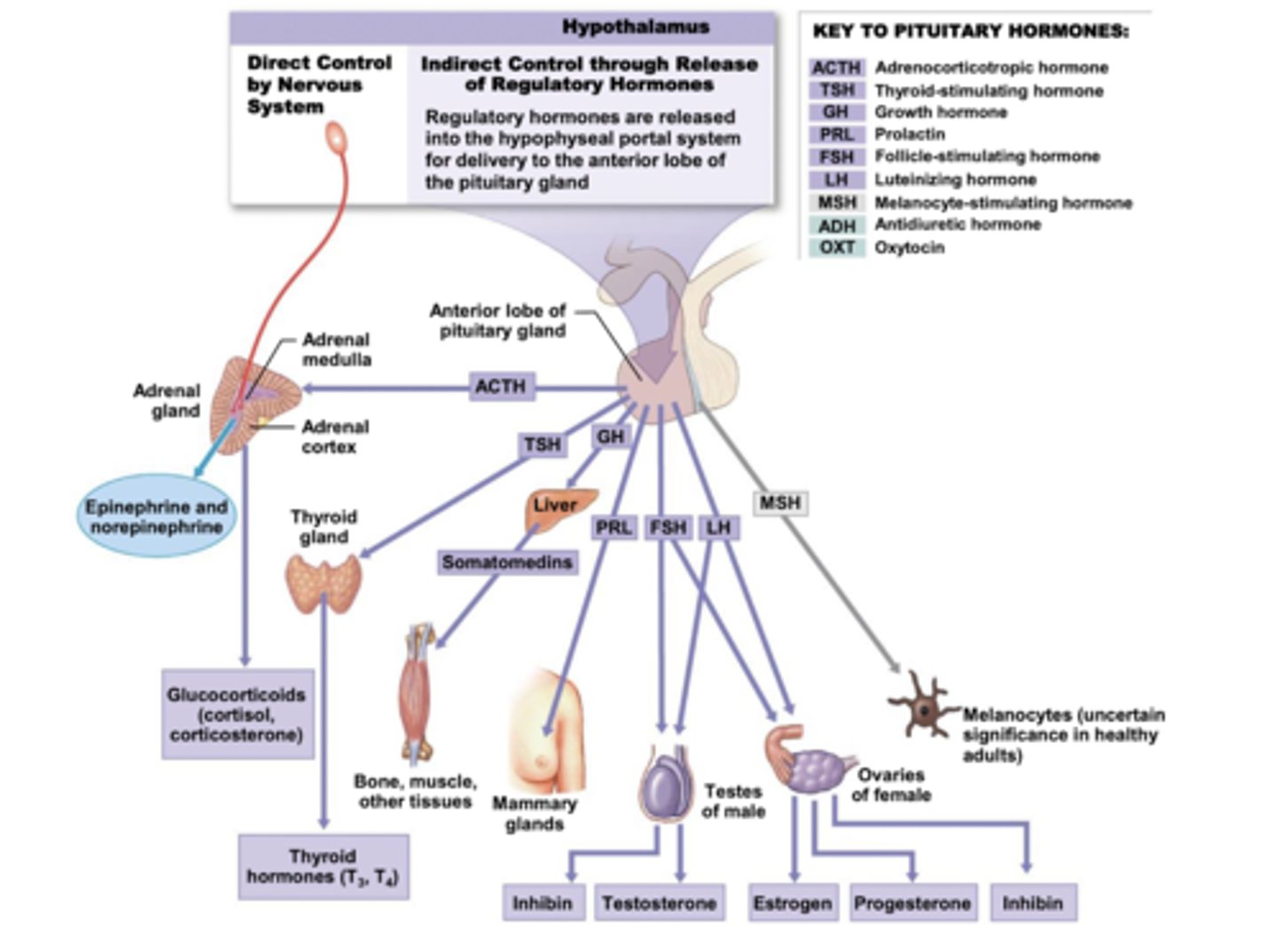
the hypothalamus' control of growth hormone release
GHRH stimulates the anterior pituitary to release growth hormone, somatostatin inhibits the release
GH secretion is stimulated by
hypoglycemia, fasting, starvation, stress
GH secretion is inhibited by
increased glucose levels, free fatty acid release, obesity, cortisol
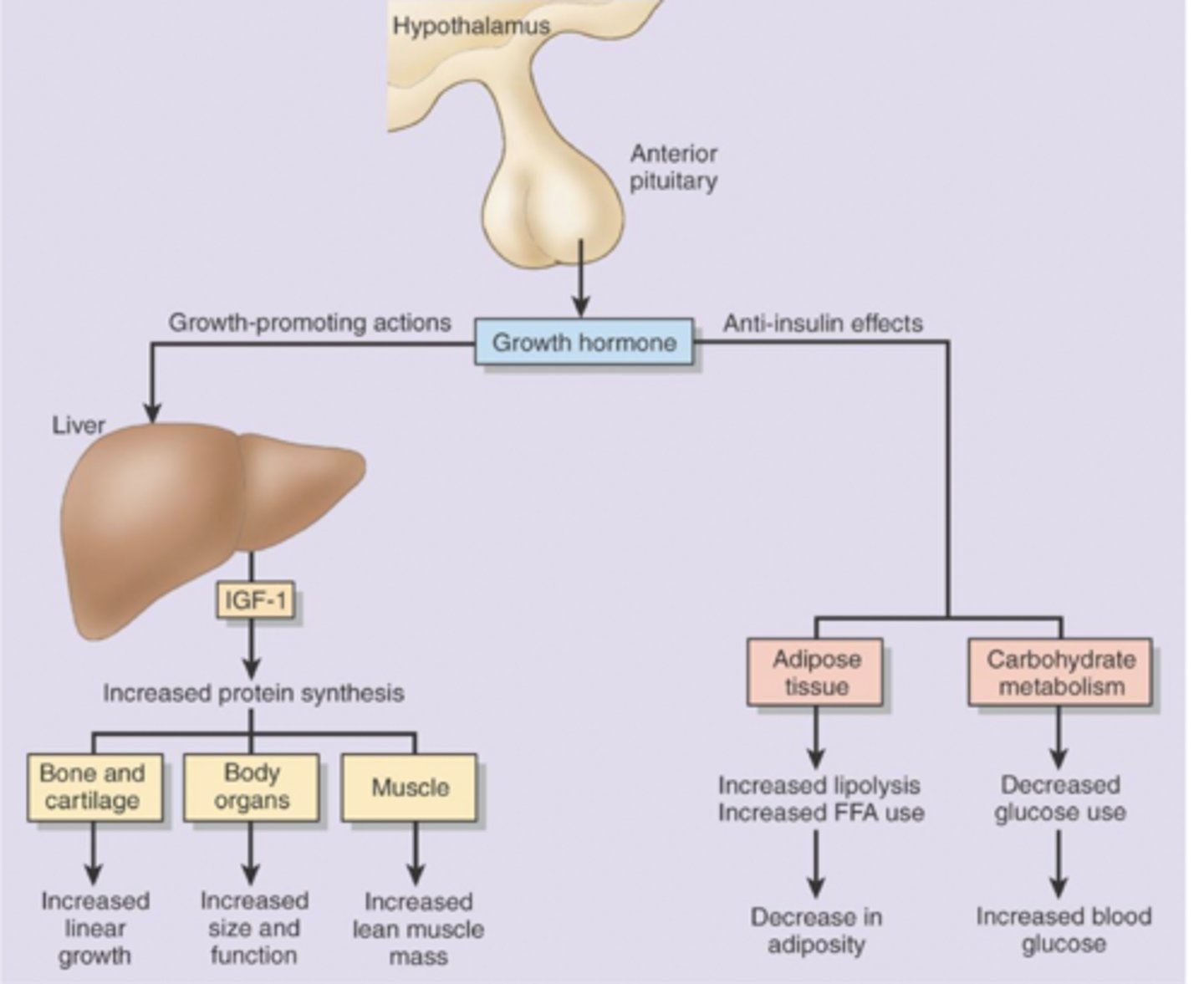
functions of the growth hormone
promotes growth through increased bone and cartilage, size and function of organs, and lean muscle mass via IGF-1 release in the liver.
promotes anti-insulin effects in adipose tissue with increased lipolysis and decreased adiposity and through carbohydrate metabolism decreases glucose use and increases blood glucose
dwarfism
deficit in growth hormone production and release. idiopathic GH deficiency (lack in hypothalamus), pituitary tumors and agenesis of pituitary (cannot product GH)
Laron-type dwarfism
hereditary defect in IGF production
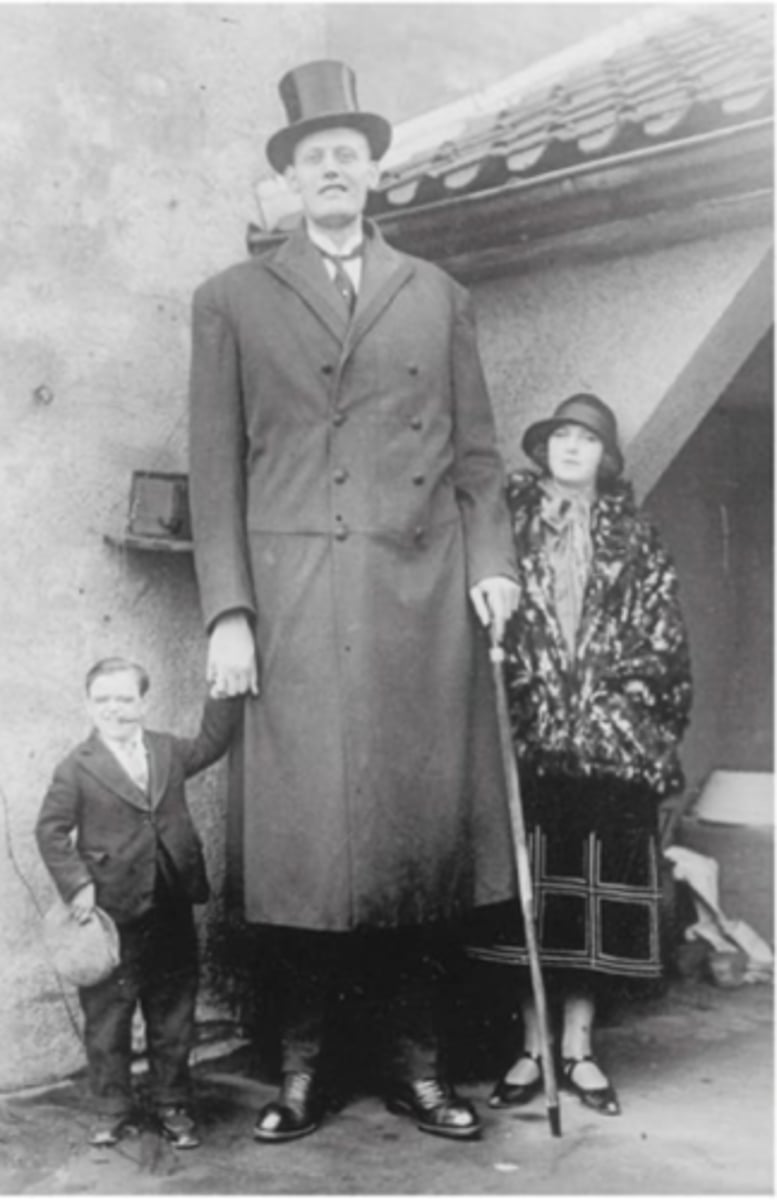
gigantism
excess in GH prior to puberty and fusion of epiphysis
acromegaly
excess GH secretion in adults that is often associated with an adenoma. bones will become broader and heavier, soft tissue will grow causing enlarged hands and feet, along with changes in facial features.
what happens when there is an excess in GH in adults?
overgrowth of cartilaginous parts of the skeleton, enlargement of organs including the heart, metabolic disturbances that alter fat metabolism and impairs glucose tolerance
causes of acromegaly
most of the time, somatotrope adenoma. other causes include excess secretion of GHRH by hypothalamic tumors, ectopic GHRH secretion by nonendocrine tumors like carcinoid tumors, ectopic secretion of GH by nonendocrine tumors.
treatment for acromegaly
normalize GH response to oral glucose load, normalize IGF-1 levels to age and sex match, remove tumor or mass, relieve central pressure effects, improve adverse clinical features
thyroid hormones
T3 and T4 - released in response to TSH. disorders can result from pituitary or thyroid gland dysfunction causing goiter, hyperthyroidism, hypothyroidism
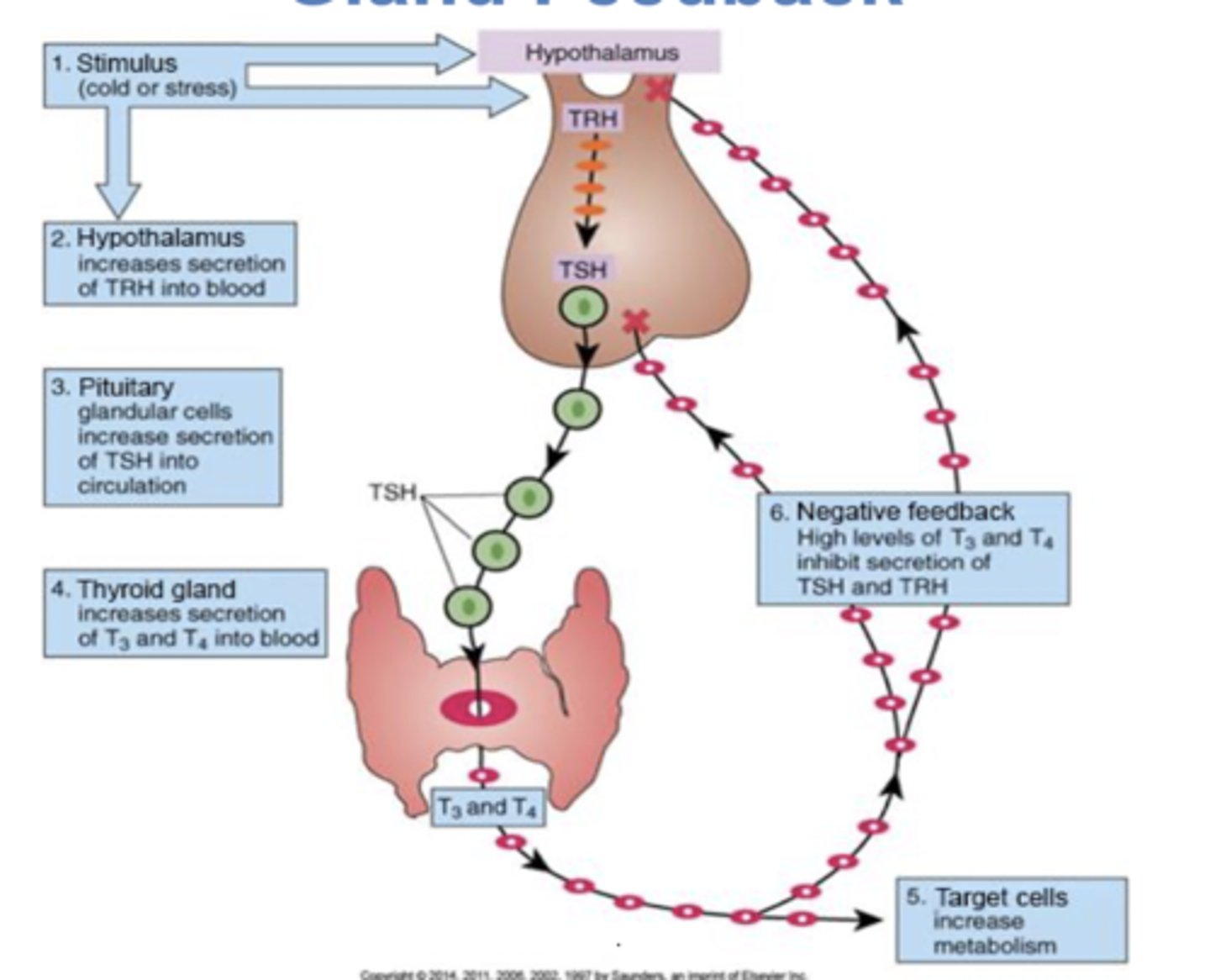
negative feedback loop in hypothalamus-pituitary-thyroid gland
a stimulus such as cold or stress will cause the hypothalamus to increase secretion of TRH in to the blood. pituitary glandular cells will increase secretion of TSH into circulation, causing the thyroid gland to increase T3 and T4 into the blood. target cells will see this and increase metabolism. the negative feedback loops occurs in response to high levels of T3 and T4, inhibiting secretion of TSH and TRH.
how do thyroid hormones effect peripheral tissues?
elevates rates of oxygen consumption and energy, increases heart rate and contraction (BP), increases sympathetic sensitivity, maintains sensitivity of respiratory centers, stimulates erythrocytosis, stimulates endocrine activity in tissues, accelerates turnover of minerals in bone
hypothyroidism
decreased metabolic rate, accumulation of hydrophilic mucopolysaccharide substance (myxedema) in connective tissues, elevates serum cholesterol
hyperthyroidism
increased metabolic rate and oxygen consumption, increased use of metabolic fuels, increased sympathetic nervous system responsiveness
manifestations of hyperthyroidism
thyroid storm, restlessness and irritability, wakefulness, increased CO, tachy and palpitations, diarrhea and increased appetite, dyspnea, heat intolerance, diaphoresis, thin and silky skin and hair, weight loss
thyroid storm
very high fever, extreme cardio (tachy, congestive failure, angina), CNS effects (agitation, restlessness, delirium) high mortality rate.
manifestations of hypothyroidism
mental and physical sluggishness, somnolence, decreased CO and brady, constipation, decreased appetite, hypovent, cold intolerance, coarse dry skin and hair, weight gain, myxedema in severe cases (nonpitting in face)
somnolence
sleepiness
myxedema coma
severe hypothyroidism; acute hypotension, hypoglycemia, hypothermia that can cause loss of consciousness
endemic goiter
hypothyroid condition in regions with low iodine levels in soil and food
goitrogens
food that contains elements to block synthesis of triiodothyroinine (T3) and thyroxine (T4)
toxic goiter
results from hyperactivity of thyroid gland
hyperthyroidism
grave's disease (autoimmune), thyroid tumors that cause hypermetabolism, toxic goiter, exophthalamos
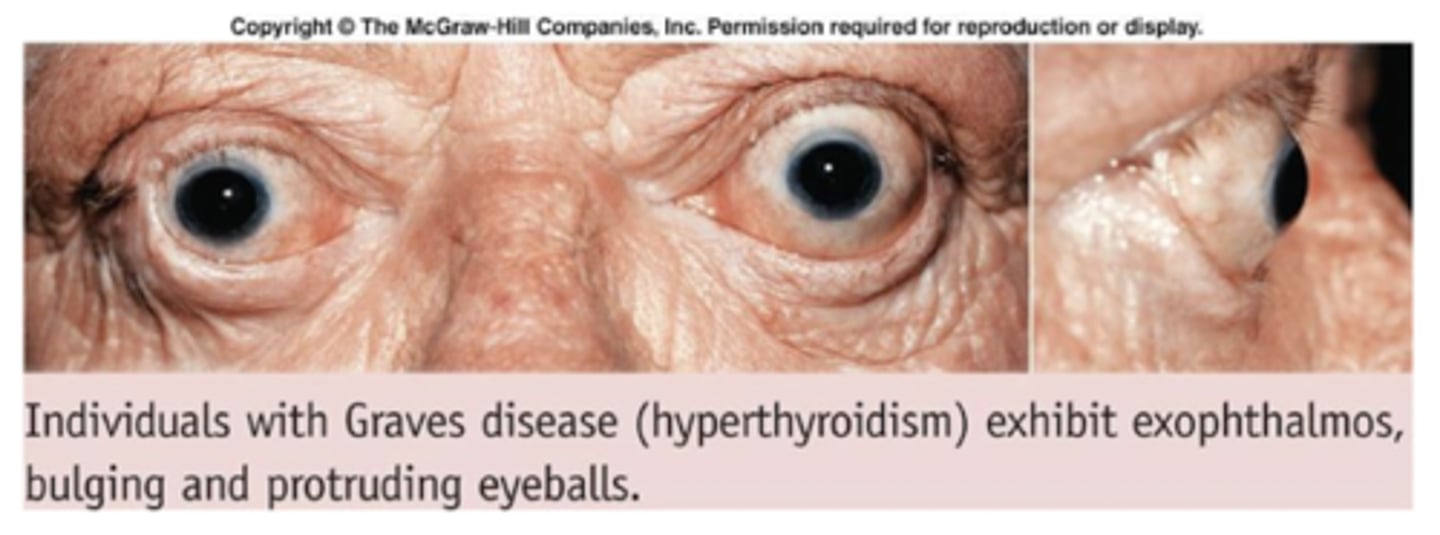
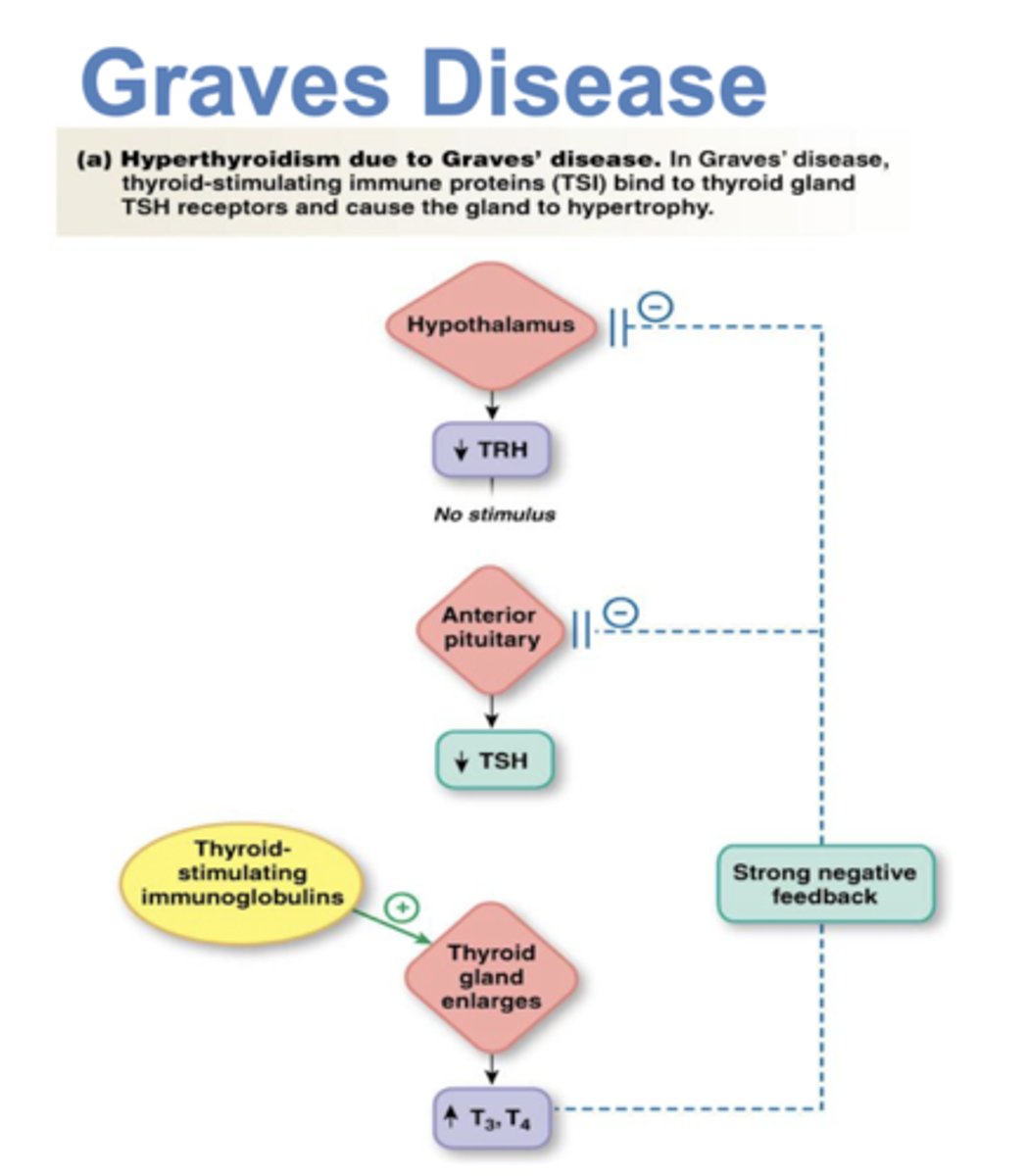
grave's disease
autoimmune disorder in which the body makes abnormal antibodies directed against thyroid follicular cells. they mimic TSH which stimulates TH release. metabolic rate is increased, sweating, rapid and irregular heartbeats, nervousness, weight loss x
hypothyroidism
iodine deficit (endemic goiter), hashimoto thyroiditis, tumor, cretinism
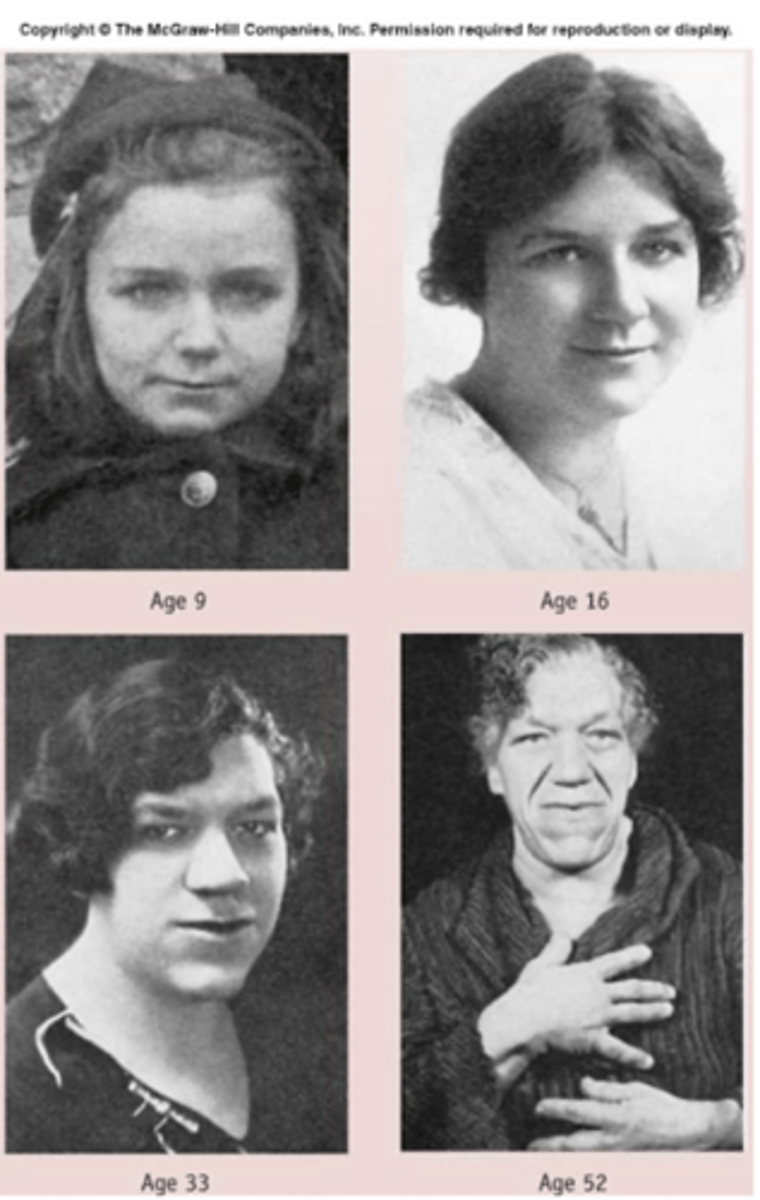
congenital hypothyroidism
thyroid hormone is essential for normal growth and development. untreated cases cause mental retardation and impairment of physical growth - manifestations here are referred to as cretinism.
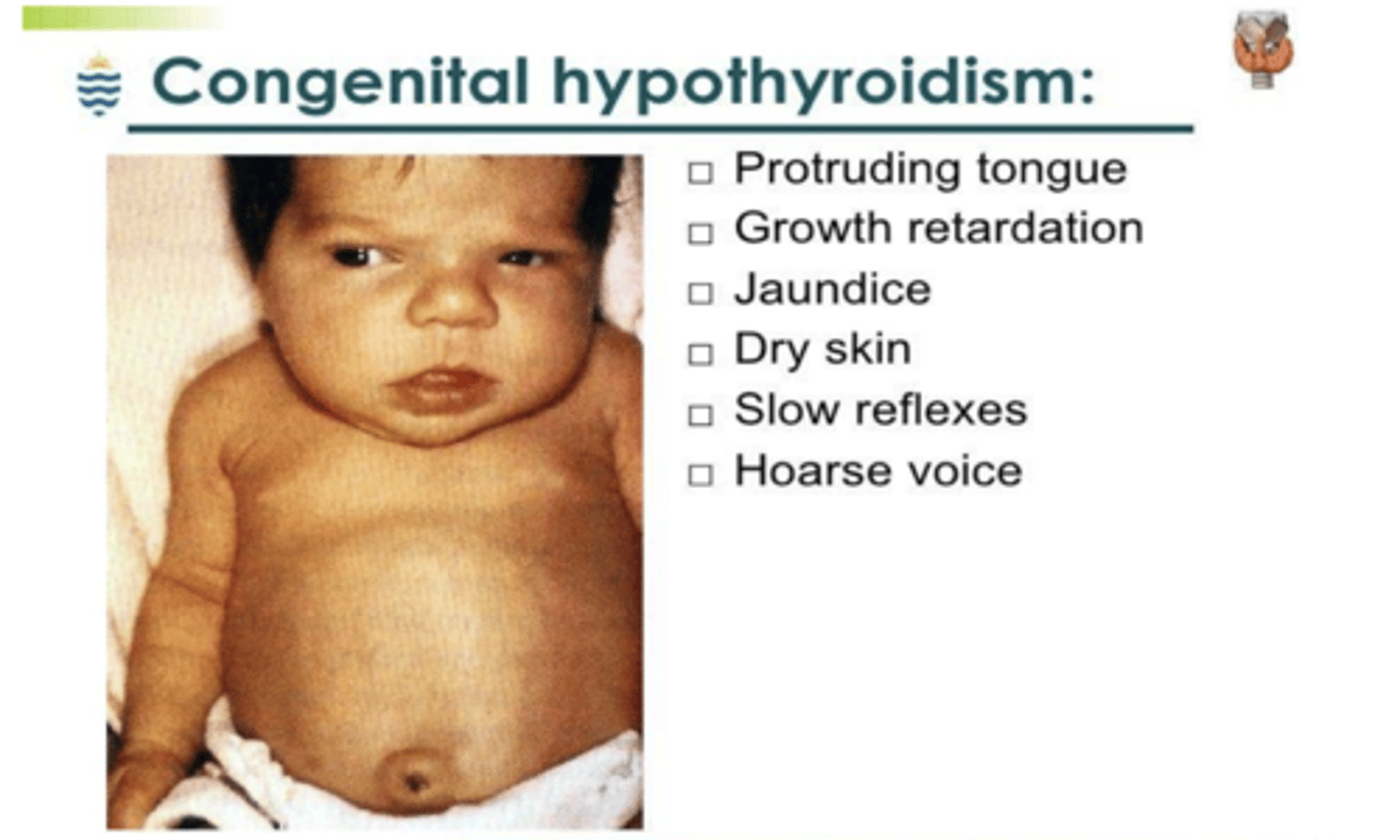
cretinism
results in short stature and cognitive defects that can be related to iodine deficit during pregnancy or untreated congenital hypothyroidism.
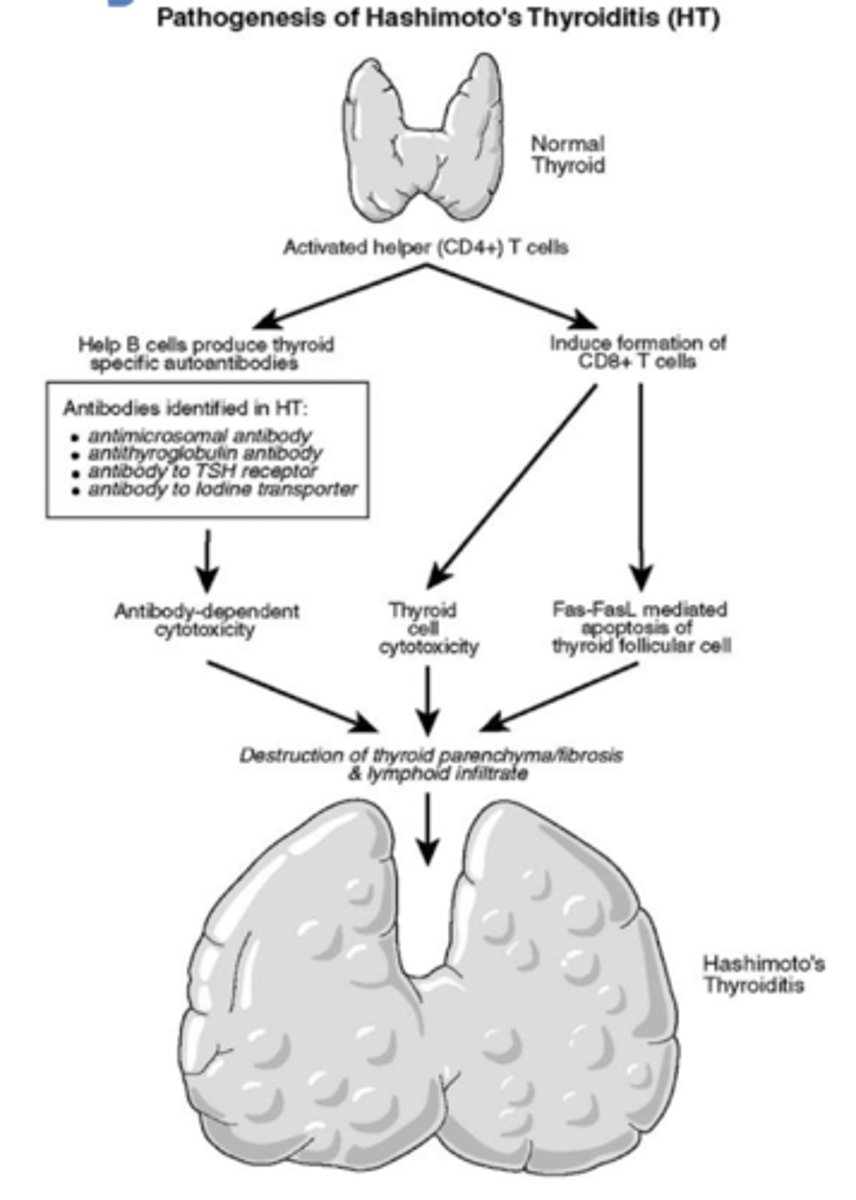
hashimoto thyroiditis
autoimmune disorder in women that destroys the thyroid, causing hypothyroidism
how are thyroid disorders measured?
measures of T3, T4, TSH; resin uptake, thyroid autoantibodies, radioiodine uptake test, thyroid scans, ultrasonography, CT and MRI scans, fine-needle aspiration biopsy of nodule
mineralocorticoids (aldosterone)
function in sodium, potassium, and water balance
glucocorticoids (cortisol)
aid in regulating metabolic functions of body and controlling inflammation. essential for survival in stressful situations
adrenal sex hormones (androgens)
serve mainly as a source of androgens for women
what are the actions of cortisol?
plasma proteins increase and immune systems are suppressed. catabolism increases, which causes muscle breakdown, free fatty acid increase, blood sugar increase, and SNS response increase
adrenal cortical insufficiency
inability to make all 3 hormones: primary adrenal being Addison disease, secondary adrenal cortical insufficiency, acute adrenal crisis
excessive adrenal secretion
glucocorticoid hormone excess (Cushing syndrome), hyperaldosteronism
congenital adrenal hyperplasia
decreased cortisol synthesis - other hormones may be increased or decreased
primary adrenal cortical insufficiency (Addison Disease)
aldosterone and cortisol levels are decreased, ACTH levels are elevated because of a lack of feedback inhibition
ACTH
adrenocorticotropic hormone
secondary adrenal cortical insufficiency
occurs as a result of hypopituitarism or because the gland has been removed. lack of ACTH.
acute adrenal crisis
bilateral adrenal hemorrhage, life-threatening situations of dehydration, acute hypotension, vascular collapse, muscle weakness
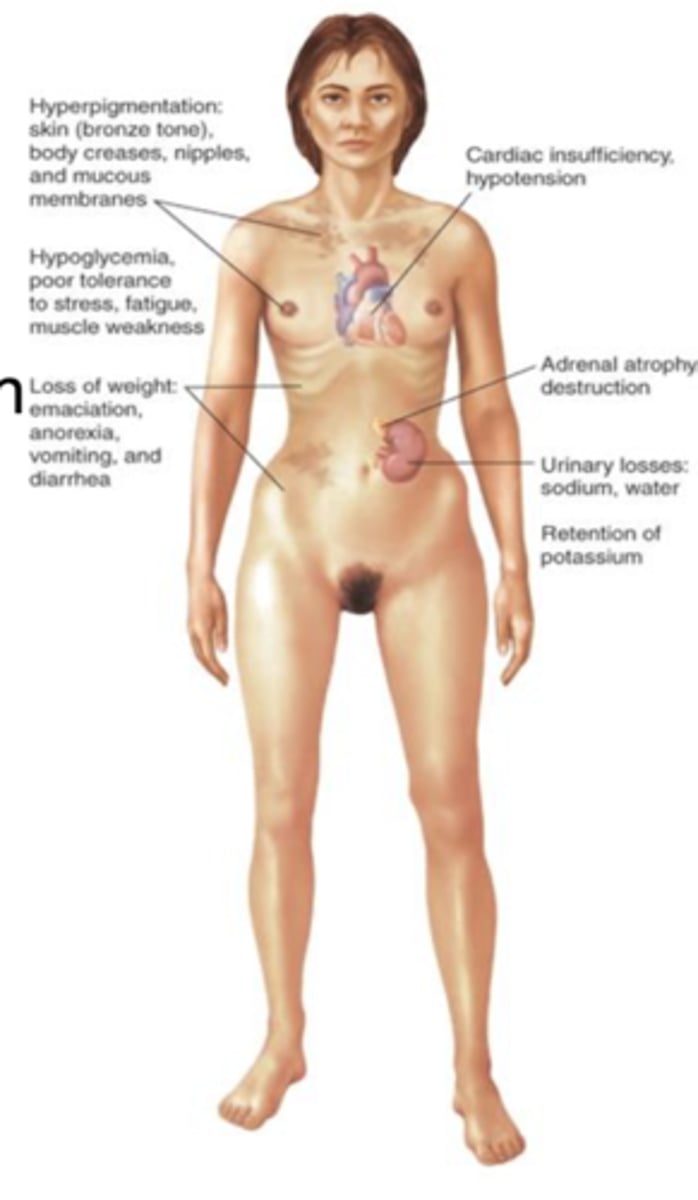
Addison disease
deficiency of adrenocorticoid secretions caused by an autoimmune reaction. the adrenal gland may be destroyed by hemorrhage or infection.
what causes addison disease?
destruction of the adrenal gland and glucocorticoid insufficiency.
clinical findings of Addison disease
anorexia and weight loss, fatigue and weakness, GI symptoms, myalgia and arthralgia, orthostatic hypotension, hyponatremia, hyperkalemia, hyper pigmentation, decreased blood volume
hypercortisolism (cushing syndrome)
pituitary form: excessive production of ACTH by a tumor of the pituitary gland
adrenal form: benign or malignant adrenal tumor
ectopic form: nonpituitary ACTH-secreting tumor
latrogenic: long-term glucocorticoid treatment
manifestations of hypercortisolism
altered fat metabolism, muscle weakness and wasting, purple striae, osteoporosis, derangements in glucose metabolism, hypokalemia, gastric acid secretion, hirsutism, acne, menstrual irregularities
Cushing syndrome appearance changes
round and ruddy face, truncal obesity with fat pad between scapulae, thin limbs and hair, fragile skin and striae
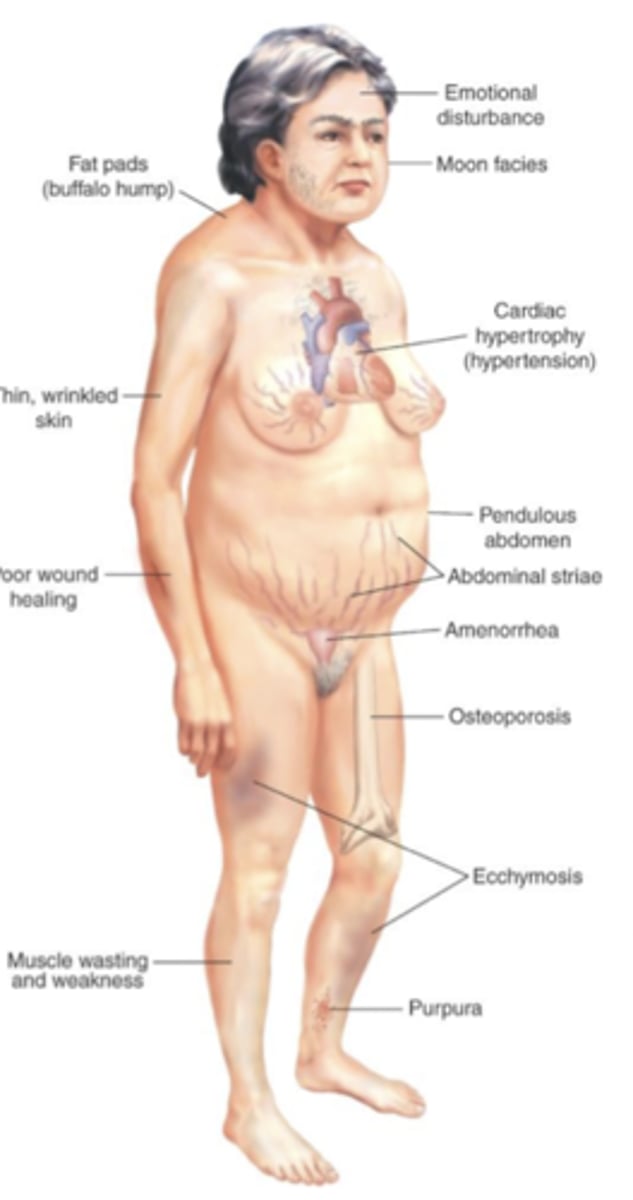
cushing syndrome
retention of sodium and water, suppression of immune response and stimulation of erythrocyte production. emotional lability and euphoria, increased catabolism of bone and proteins, delayed healing, increased insulin resistance and glucose intolerance
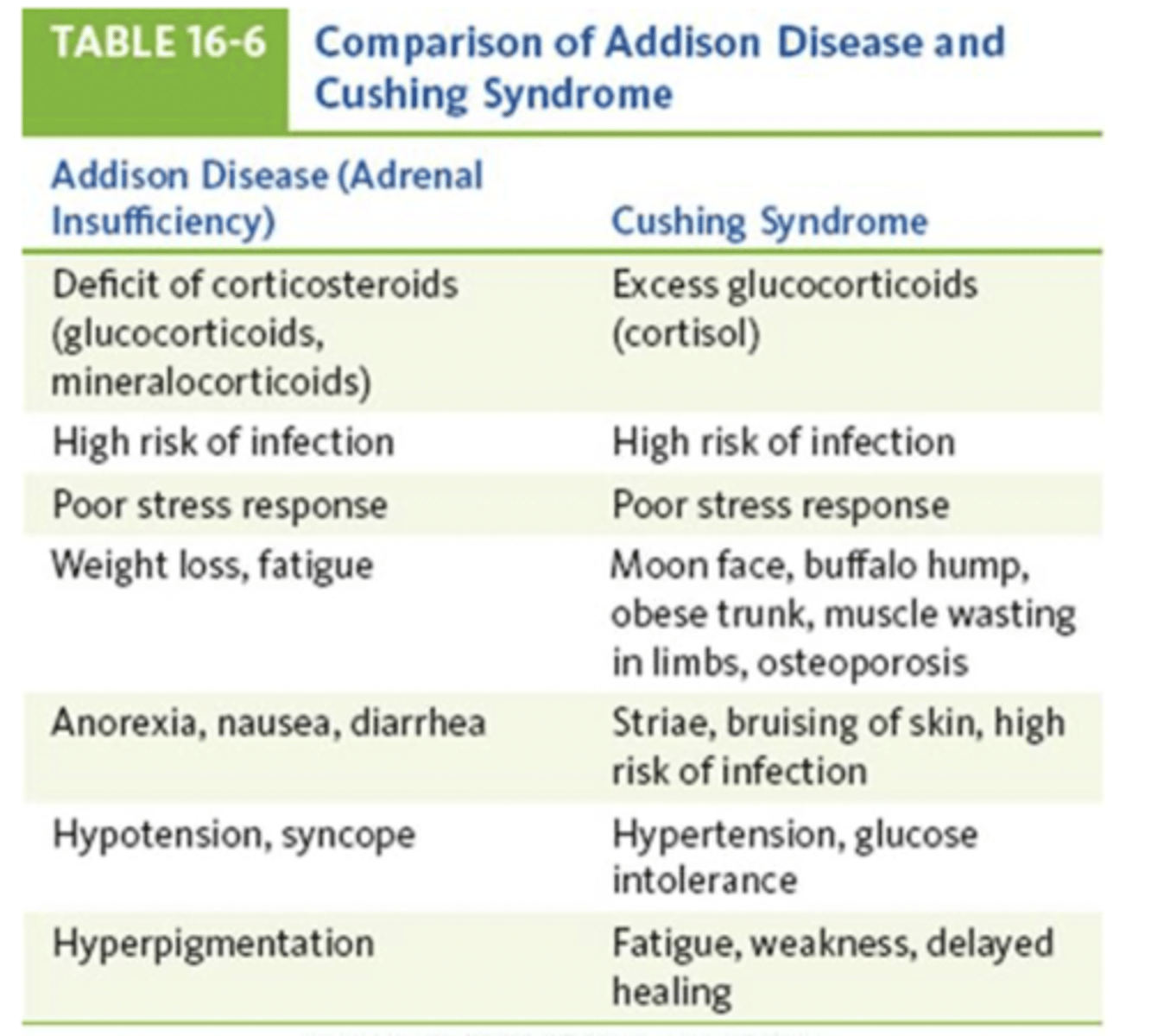
compare and contrast of addison disease and cushing syndrome
both have high risk of infection and poor stress response.