Looks like no one added any tags here yet for you.
Bipolar disorder
mental illness with cyclic fluctuations in mood (mania, hypomania, depression)
2 types
1 min 1 manic ± major depressive episode or hypomania
2 min 1 depressive episode + min 1 episode of hypomania + no hx of manic episode
Risk factors of Bipolar
substance abuse
family hx
psychosocial
head trauma
perinatal insult
Most common in
adolescents 15-30 yo (mean age 21y/o)
Mania
no sleep
more self-esteem
mood disturbance has effect on social or occupational functioning
symptoms present >= 1 week and present nearly every day or other condition
faster speech
racing thoughts, easily distracted
goal directed activity or agitation
not attributed to substance
Mania - DIG FAST
distractibility
impulsivity
grandiosity
flight of idea
activity increase
sleep deficit
talkative
hypomanic episode
not severe enough for impairment in social/occupation function (no hospitalization)
at least 4 consecutive days and most of day
Medical causes of Manic symptoms
CNS
Infection
Electrolyte or metabolic abnormality
Endocrine or hormonal dysregulation
Non-pharm for bipolar
MANIA - d/c antidepressants, stimulants, nicotine, caffeine (at the start of diagnosis)
DEPRESSION - d/c BZD (at the start of diagnosis)
ECT (last resort)
CBT
Psychoeducation programs
mood stabilizers in bipolar disorder take how long for effect
2-4 weeks
Lithium
1st line for acute mania, maintenance, mild depression
Monitor Li 12hr after dose every 2 months
acute
maintenance
elderly
acute mania Li level
0.8-1.2
maintenance Li level
0.6-1.0
Li toxicity is seen at
1.5
What increases lithium levels?
dehydration
large change in Na
NSAIDs
ACEI
What should be monitored with Li treatment?
Renal
thyroid function (can cause hyperparathyroidism→Hypercalcemia, hypothyroidism>hyperthyroidism)
AE of Li
ataxia
impaired neurocognition
thyroid abnormality
Tremors on Li therapy - try these:
decrease/eliminate caffeine
Li dose reduction
addition of beta blocker
avoid in lactation
Valproic acid/DVPX
Valproic level monitored during initation and titration
teratogenic
Lamotrigine aspects
all pt that develop a rash must stop lamotrigine and see ER asap → can turn into SJS or TENS
wt neutral
NAUSEA
Carbamazepine
good for mixed states
titrated slowly to avoid SJS and TENS
most monitor to avoid toxicity (no correlation btwn serum level and efficacy)
First line monotherapy acute mania regimen in order (unless pt factors specify otherwise
Li
quetiapine
Vlproic Acid
Asenapine
Aripiprazole
Paliperidone
risperdone
cariprazine
1st line combination therapy acute mania
Quetiapine + Li/DVP
Aripiprazole + Li/DVP
Risperidone + Li/DVP
Asenapine Li/DVP
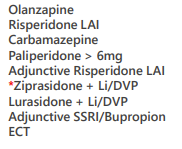
2nd line tx for acute mania
olanzapine
carbamazepine
olanzapine +Li/DVP
Li +DVP
ziprasidone
haloperidol
ECT
1st line Acute depression bipolar (chose in order they are given)
quetiapine
lurasideone + Li/DVP
Lamotrigne
Lurasidone
Adjunctive Lamotrigne
2nd line Acute depression bipolar (chose in order they are given)
DVP
adjunctive SSRI/Bupropion
ECT
Cariprazine
olanzapine + fluoxetine
Maintenance of bipolar prevention of mood episode 1st line
lithium
quetiapine
DVP
lamotrigne
asenapine
Maintenance of bipolar prevention of mood episode 1st line - PREVENTION OF DEPRESSION ONLY
Aripiprazole + Li/DVP
Aripiprazole PO
Aripiprazole LAI
2nd line maintenance of mood episode
monitoring parameters
2-4 weeks - improved mood, thoughts, behaviour, sleep - use MDQ
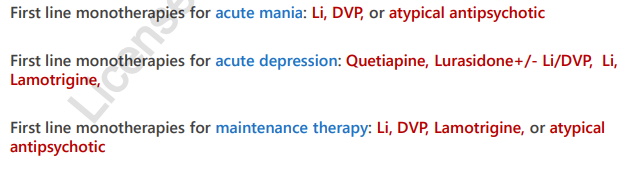
1st line monotx for acute mania
1st line monotx for acute depression
1st monotx for maintenance tx
why are AP difficult in conception?
conventional antipsychotics and risperidone increase prolactin which interferres with ovulation and decrease fertility (may need d/c)
taper prior to conception - must be stable for 4-6 months and low risk of relapse