Pupil assessment (9)
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
what is the pupil
an aperture in the iris
regulates retinal illumination
very small (miotic) in brightly lit conditions and large (mydriatic) in dim illumination
covered by a membrane up to the 8th month gestation
what 2 muscles does the iris contain
sphincter pupillae
dilator pupillae
both innervated by thr autonomic nervous system : controlled by the central neural pathways that are influenced by retinal illumination , viewing distance, attention and alertness
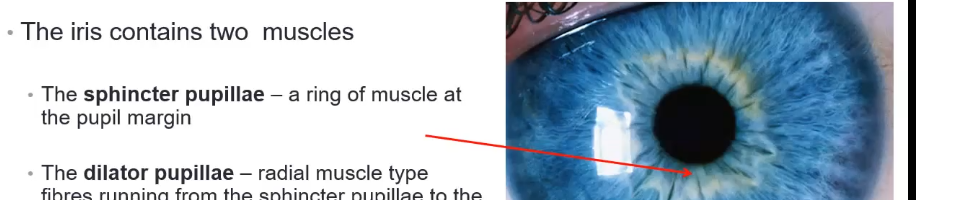
what is the sphincter pupillae
a ring of muscle at pupil margin

what is the dilator pupillae
a radial muscle type fibres running from the sphincter pupillae to the iris root
sphincter muscle
circular muscle
anchored to adjacent stroma and retains its function even if severed
contraction of the sphincter causes pupil to constrict in miosis.
muscle is innervated by the parasympathetic system
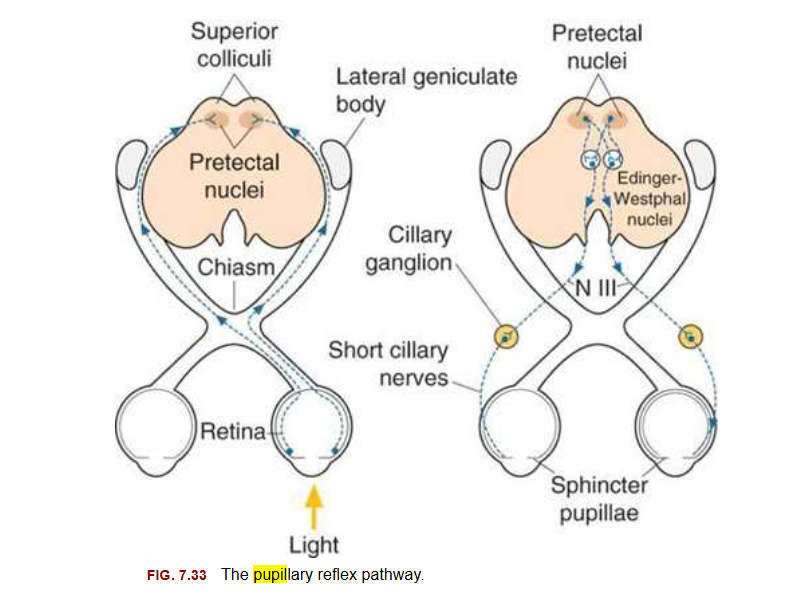
Afferent: to the brain - optic nerve → chiasm → optic tract → pretectal nucleus
Efferent: from the brain - ciliary gaglion → 3rd nerve → sphincter pupillae
section of iris: shows sphincter
dilator: myoepithelium which is muscle and epithelial properies

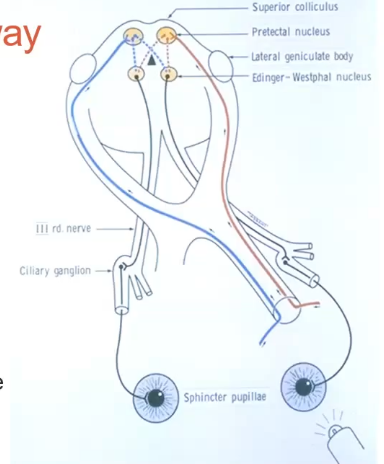
Afferent pathway
going from retina down the optic nerve, half goes into the brain on one side, other goes to the brain on the opposite side
fibres of sphincter muscle doesnt go too far into the brain . hits pre tectal nucleus
crosses over- so any light shon on one eye should affect both
efferent pathway
ciliary ganglion from the brain, passes the 3rd nerve then to the sphincter pupillae
dilator - innervation pathway
dilator pupillae
innervated by sympathetic system
arises from the superior cervical ganglion
lack of stimulation of sphincter causes pupils to get bigger
starts from the central nervous system in the neck ( cervical ganglion)
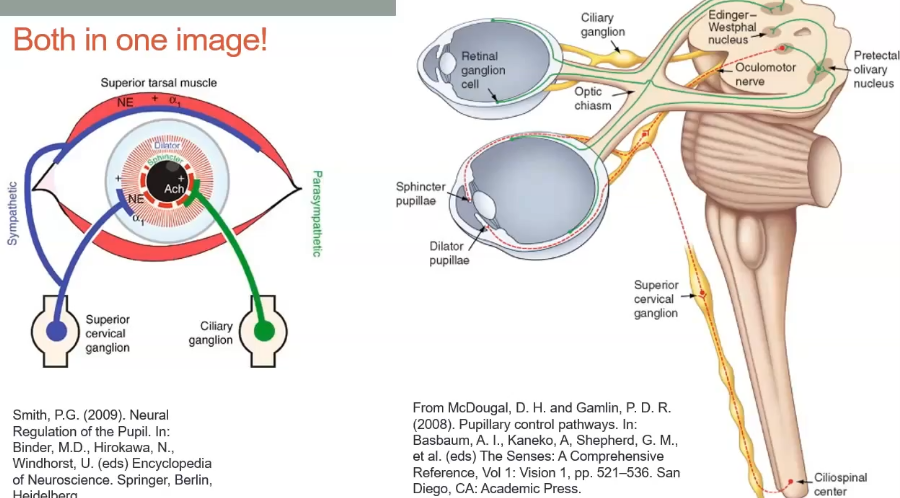
both pathways in the eye
pupillary reflec pathway
pupil responses
pupil response- dilation
this is when pupil gets larger
called dilation/mydriasis
stimulated by sympathetic nervous system or lack of stim from sphincter
associated with low light
associated with mydriatic drugs eg tropicamide or phenylphrine , or amy sympathetic NS stimulant
associated with excitement or fear
pupipl response- constriction
pupil gets smaller
miosis
induced by the parasympatheic action on the sphincter muscle
associated with bright light
miotic drugs
what are the 2 types of pupil responses
direct- seen when the light enters the eye
consensual- seen when light falls in the fellow eye
pupils should react as a pair
if shine light in one eye and that pupil constricts its called direct
when shine light in one pupil and look at the other eye, thats consensual
the pupil- the near triad
accomodation - pupil constriction change when looking at distance vs near
convergence
pupil constriction
pupil size
it is governed by a balance between the sypathetic and parasympathetic input
methods of assessment of the pupil
done in normal room illumination
px remove glasses
look at a letter on the chart
use a spotlight if they have a vision of less than 6/18 or theyre hyperopic , to avoid stimulating accom
sit in front of the patient, dont block their view
check for size shape and location
checkng pupil size
both pupils should be equal in size
bright light: 3-6 mm in da=iameter
dim light: 4-8mm in diameter
the pupil size will show normal fluctuations known as hippus
pupil size nomally decreases with age
pupil shape
both pupils should be round or even slightly oval
location of pupils
both pupils should be central in the iris
measuring pupil size
can use a ruler or pupil gauge
have ruler on forehead and as close to thr px eye as possible
reduce the room illumination but keep emough light to se the pupil margin
use a UV burton lamp if eyes are dark
do in bright and dark
repeat the pupil measurements

duchek pupil gauge
peoce or plastic, cardboard with holes in it
distance between holes get larger
start from bottom
hold the gauge as close to the eye as possible
look through the bottom pair of holes
the holes appear to overlap through which you can see the distance target
move the card down. As you lool through the holes that are further apart the images will overlap less
at some point the images will only just touch ( no black in between them) ,and youll only be able to see the distance target . this is the pupil size
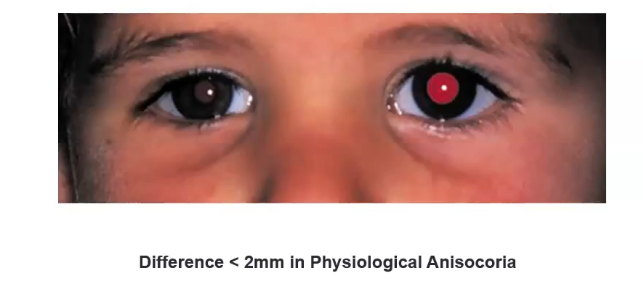
anisocoria
unequal pupil size in normal room illumination
down to physiology
direct and consensual reflexes
px fixates ahead at the chart or spot of light
shine a pen torch into the right eye (5-10cm)
position the light at the inferior temporal side
watch the right eye for constriction
note down speed and degree of response
this is direct response
do the same but watch the left pupil for constriction : consensual response
may need a burton lamp
repeat with light entering the left eye
observing the direct and consensual dilation
shine the light in the right eye as before
observe the pupil response in both eyes when the light is removed
it should be equal
now repeat shining the light in the left eye
observe the diation when the light is removed
should be equal and smooth
swinging flashlight test- RAPD
checks the afferent pathway to the brian
the patient fixates in the distance
holds the pentorch below the right eye (5-10 cm) for 2-3 secs
quickly move the light over to the same position but below left eye
keep the position below the eye
pause for 2-3 seconds
repeat several times
observe the pupil size as the light is swung backwards and forwards
swinging flashlight test results
normal
pupil constricts as light enters the eye
briefly dilates as torch swings to other eye
re constricts as conselsual reflex occurs
abnormal
the pupil of the effected eye will appear to dilate when the light falls on it
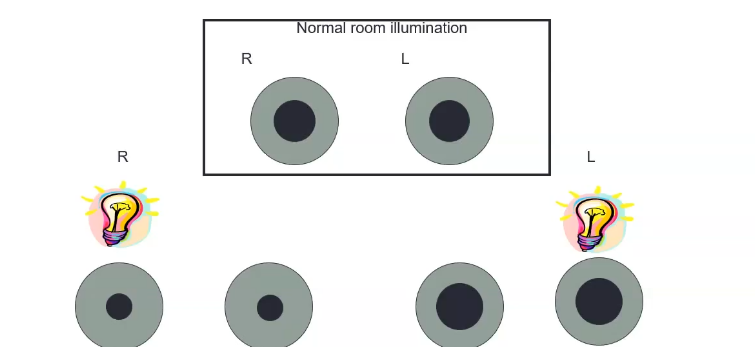
afferent pupil defects: absolute
with light in one eye, both eyes constrict
swap over to other eye- pupil gets bigger in both eyes
left absolute defect- dilating back to what it was in normal room illumination , no stimulus is affecting the eye
when light is shon into the affected eye, both pupils dilate slightly because less afferent signal is sent
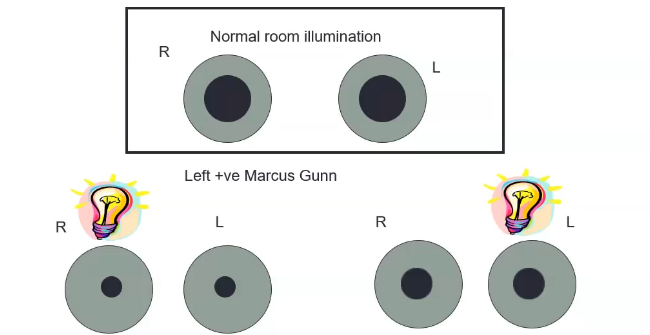
afferet pupil defect- relative
when illuminating one eye, both eye constricts
when illuminating other eye, dilates slightly but doesnt go back to the normal room illumination
less signal is sent ot the brain
positive RAPD
relative to the response in the right eye- left
how to dteermine the affected eye for RAPD
shine light in one eye for 2-3 seconds
observe both pupils
normally, both pupils constrict
swing the light to the other eye and observe
if the pupils dilate when light is shining into the left eye fo rexample, then the left eye is affected
the near reflex ( reading response)
often tested if a problem is found with the light responses
px fixates into the distance
ask the px to fixate a near target 15cm away
dont use pentorch as target
observe the pupil constriction as the px look sat the near target
observe the dilation as the px returns their gaze to the distance
pupil defects
what are the 2 types of pupil defects
afferent- signal impaired going to the brain
efferent- signal impaired coming from the brain
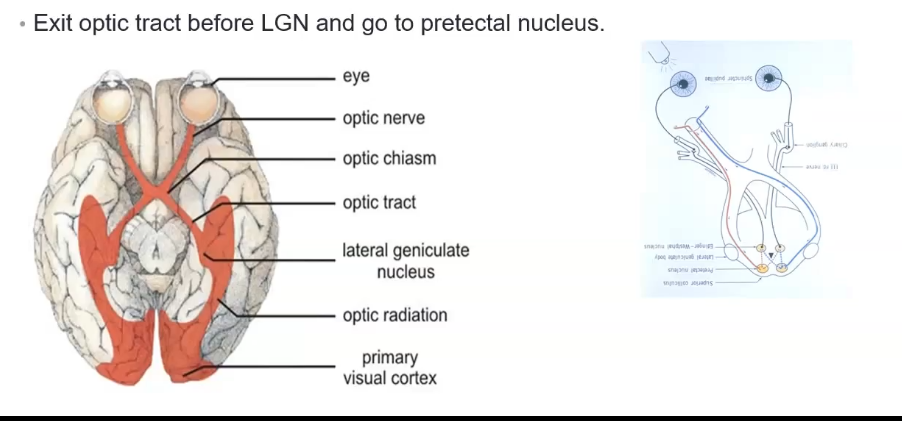
afferent pupil fibres
starts at the retina. photoreceptors detect the light and signals travel through bipolar cells → ganglion cells
travels to optic nerve which caries all visual and pupillary light reflex signals from one eye
goes to optic chiams, where around 505 of fibres from nasal retina cross to the opposite side
optic tract- contains fibres from both eyes, each optic tract carries info from contralateral visual field . pupillary fibres remain in the tract bt peel off begore reaching the LGN ( lateral geniculate body)
goes to the pretectal nuclues- midbrain: this is where the afferent signal for pupil reflec synapses
creates a direct and consensual response
afferent pupil defects
the pupils are equal size in normal room illumination
recording:
RAPD present / RAPD not present
or positive RAPD / negative RAPD
efferent pupil fibres
motor pathway that carries signals from the brain to the eye making the pupil constrict
edinger westphal nuclues located in midbrain, recieves input from both pretectal nucleus and sends paasympathetic fibres to control pupil constriction
the parasympathetic fibres travel superficially on outside of oculomotor nerve,
oculomotor nerve synapse at the ciliary ganglion
post ganglionic fibres leave ciliary ganglion and travel via short ciliary nerves to the eye
reaches the iris sphincter muscle and the parasym activates causing pupil to constrict
iris dilator is via long ciliary nerves
fixed miotic pupil defects
horners
iritis
argyll robertson
long standing adie
pharmacological
fixed mydriasis pupil defects
trauma
adie
acute ACG
third nerve palsy
pharmacologcal
efferent pupil defects
adie or tonic pupil- large pupil
loss of input from ciliary gangliato sphincter - where the sphincter muscle gets its innervation
unopposed dilator action
adie pupil
80% unilateral
young adults typically affected usually female
other associations like temporal arteritis, diabetes

third nerve palsy
large pupil - sphincter pupillae innervated by the third nerve, so if anything affecting the third nerve causes the large pupil
thrd nerve also controls ocular muscles and levator muscle
so get droopy lids, eye goes down and out
refer to hospital
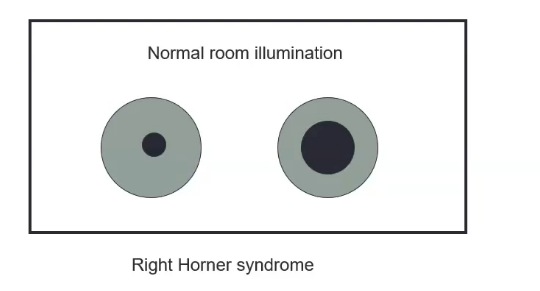
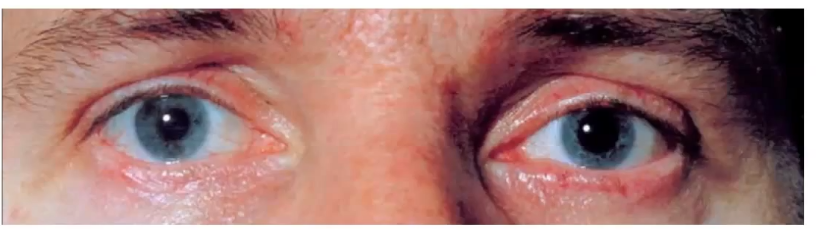
efferent pupil defects: horners
horners syndrome- loss of input from the sympathetic ganglia
unopposed sphincter action
smaller pupil
dilator muscle paralysed
any age
associated with poor dilation, ptosis and facial anhydrosis
check up routinely
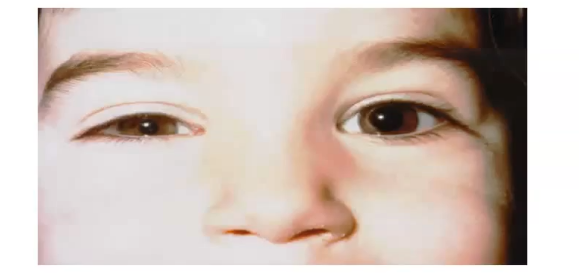
ptosis
drooping of the upper eyelid
if ptosis is on the same side as miotic pupil: horners
is ptosis is on same side as mydriatic pupi: third nerve palsy
miotic pupil conditions : argyl and iritis
argyl: pupils so not constrict to light but do when focusing on near objects
iritis : red eye , pain , constricted pupil , cells and flar in anterior chamber

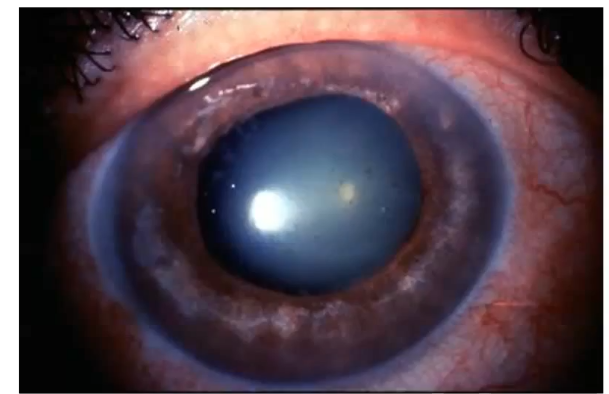
mydriatic pupil : acute angle close glaucoma
fixed diated pupil in acute angle closure glaucoma
linked to IOP and drainage of aq humour
the pupil resonse- recording
pupil size in mm
pupil shape
pupil reflexes- direct and consensual
speed of response may also be added on a scale of 0 ( no response) - 4 ( large brisk response)
check and note for RAPD , either ±
PERRLA: recording
P: pupils
E: equal
R: round
R: reactive
L: light
A: accom - only check ifresponse to light was not normal

both the pupils constrict, which eye is showing a consensual resonse
left

both pupils dilate, which eye is blind?
the right, as light is shining into it
what is unequal pupil size in normal lighting conditions called?
anisocoria
what causes a small pupil
horners
constriction of pupil sphincter muscle causes what
pupil constriction
miosis ( another word for pupil constriction)
stimulation of the sympathetic nervous system causes what?
both pupils to dilate
parasyn: causes both pupils to constrict