L10: Meniscal & Articular Cartilage Injuries
1/88
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
89 Terms
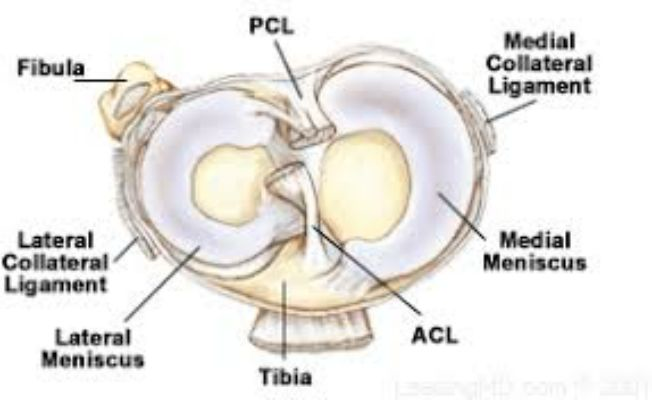
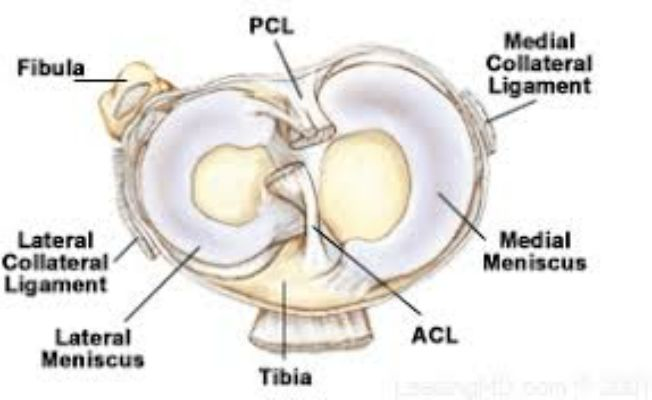
How does the lateral and medial meniscus differ?
Lateral Meniscus
More circular or "O-shaped"
Covers smaller area of the tibial plateau
Medial Meniscus
Semi-lunar Shaped
Covers larger area of tibial plateau
Thicker and "more bound down"
The ________ meniscus is more commonly injured / torn
Medial
The ________ meniscus is thicker
Medial
What is the structural make-up of the menisci?
Collagen
Type I Collagen on the outer portion of the menisci
Hyaline Cartilage on the inner portion of the menisci
Organization:
Collagen bundles run deep and circumferentially
Utilizes hoop tension to help provide stability (w/ compression it expands)
Proteoglycans
How does Type I Collagen differ from Hyaline Cartilage in terms of strength?
Hyaline Cartilage is deemed to be not as strong; this is why tears are more common in the inner portion of the mensci
What is the typical MOI for a mensci injury / tear?
Usually occurs at ≥ 60 degrees of knee flexion
What 3 forces can the mensci resist?
Compression
Shear
Tension
What portion of the meniscus has the greatest amount of blood flow?
Regarding blood flow, what occurs as we go more medially / to the center?
There is decreased blood flows as you move more medially / centrally of the meniscus
What are the different Blood Flow Zones of the Meniscus?
Red Zone -- this is the area with the greatest amount of blood flow
Red-White Zone -- still has some blood flow, but less compared to the red zone
White Zone -- minimal to no blood flow
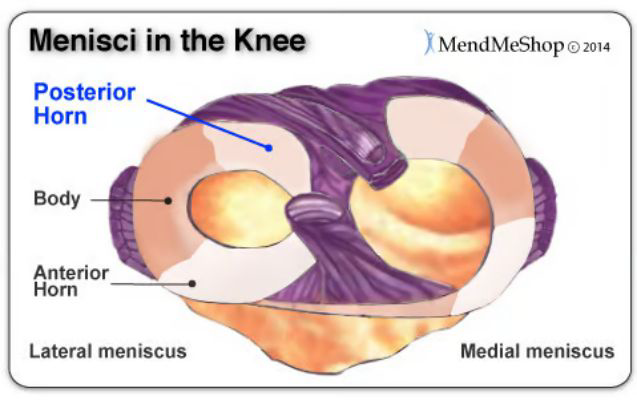
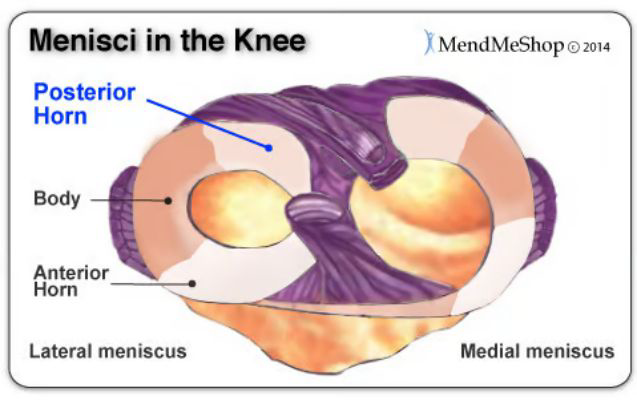
What portion of the medial meniscus is most often injured? Why?
Posterior Horn is the most commonly injured as it is where the meniscus is "most anchored down" / adhered
Blood flow is important for ________
What components does it specifically relate to?
Tissue healing
Blood flow relates to the ability of a tissue to heal and the time-frame it takes to heal
How do the different Blood Flow Zones of the Meniscus relate to different post-surgical / injury outcomes?
Areas of greater blood flow = higher likelihood of success / healing
Example:
A patient who has a red-to-red tear and gets a surgical procedure is clinically sound and has a good likelihood of recovery and a positive outcome
On the other hand, a patient who has a white-to-white meniscal tear and receives a surgical procedure has a much poorer outcome with surgery (and the decision to have surgery may not be clinically sound)
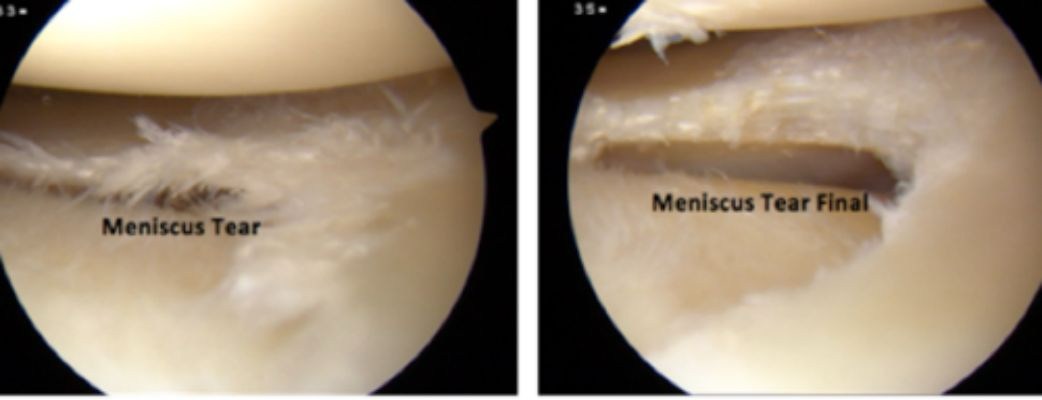
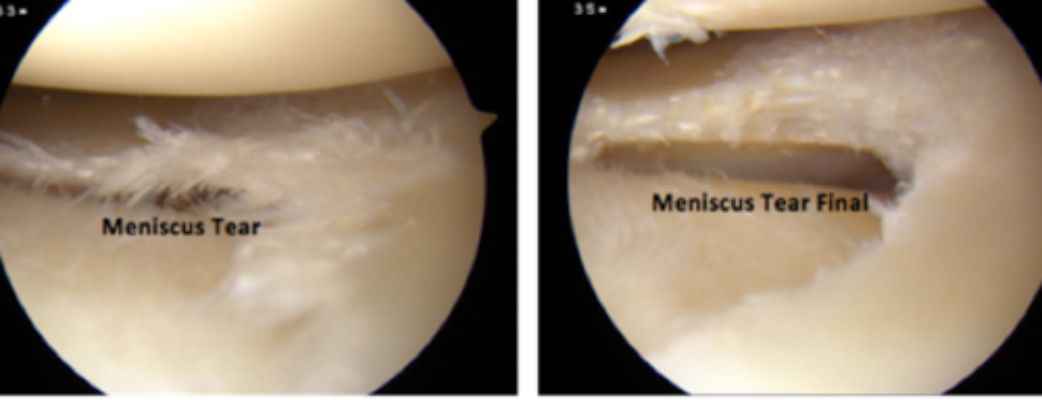
What is the Gold Standard for diagnosing a Meniscal Tear?
MRI with Contrast
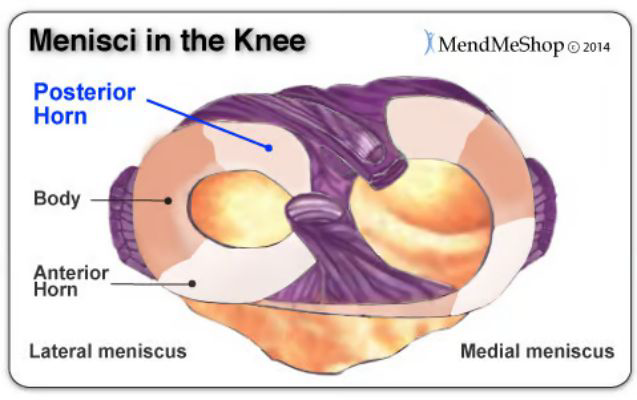
A tear of the ________ if often missed, even with a MRI
Posterior Horn
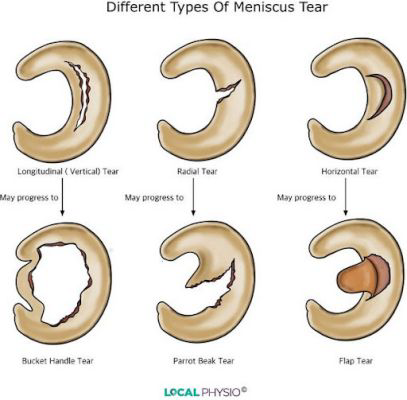
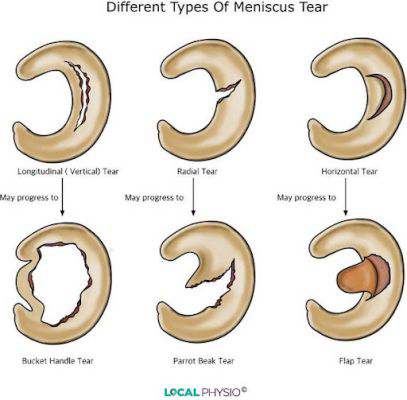
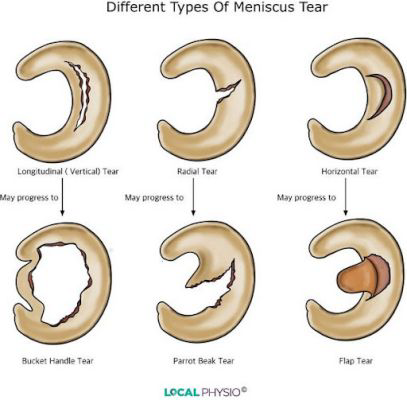
What are the three (initial) primary meniscal tears?
Longitudinal Tear
Radial Tear
Horizontal Tear
What meniscal tear type is typically the most successful?
Longitudinal Tear
How is a Longitudinal Tear of the Meniscus typically repaired?
The edges of the tear are "brought together" and then sutured
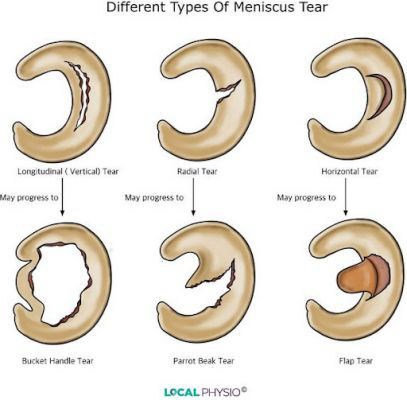
What might a Longitudinal Tear of the Meniscus progress to?
Bucket Handle Tear
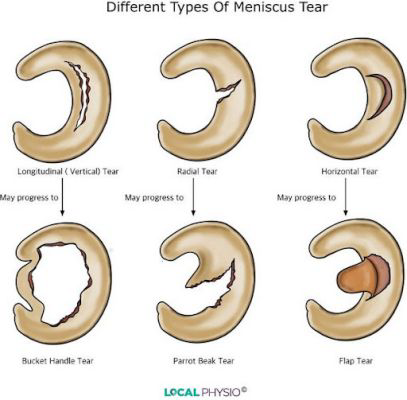
Discuss a Radial Tear of the Meniscus. How difficult is it to repair / heal?
Harder to repair due to location (poorer vascularization)
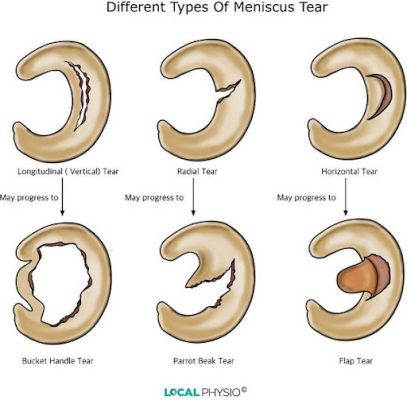
What can a Radial Tear of the Mensicus progress to?
Parrot-Beak Tear
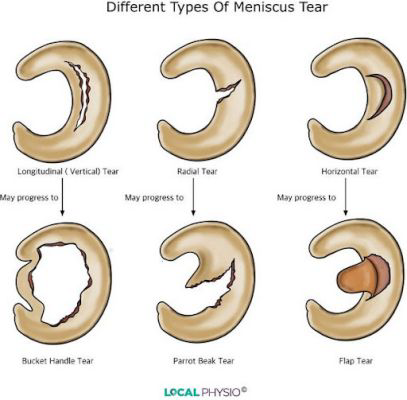
Discuss a Horizontal Tear of the Meniscus.
Decreased healing / vascularization; may give the feeling of catching/locking
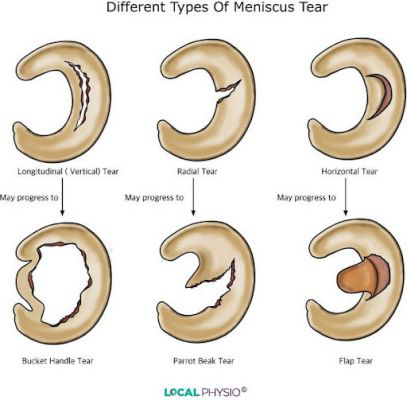
What may a Horizontal Tear of the Meniscus progress to?
Flap Tear (which has the ability to impede the joint space)
When is the outcome for a meniscal injury actually better?
When the meniscal injury occurs with a ligamentous injury
This brings greater blood flow and healing factors to the area, and thus better healing (especially when repaired via surgery)
Do traumatic or degenerative meniscal tears "do better"?
What is the Gold Standard to "pick up" meniscal tears / injuries that do not show up on an MRI?
Arthroscopy
What is a Meniscectomy?
Removal of the menisucs
Full meniscectomies are not commonly performed anymore d/t increased risk / prevalence of DJD
If performed today -- likely to be a partial meniscetomy (removal of just the injured / torn part of the meniscus)
What are the benefits of a meniscal repair?
It helps to prevent the onset of DJD
If we take away the meniscus, this causes more loading on the articular cartilage
Idea is "long-term preservation"
What are the different ways that a meniscal repair can be performed?
The edges of the tear are approximated and either sutured or tacked down
(sutures are more common d/t tacks sometimes falling out)

If a patient reports a MOI for the knee, what do we need to screen for?
Meniscal Injury / Involvement
What is the key subjective information for a patient with a meniscal tear?
Felling of catching or clicking in the knee
Feeling of "buckling"
Pain with CKC
Pain with ascending stairs
MOI where they stated a "pop"
Should NOT see a lot of swelling (if ONLY meniscal involvement)
If swelling = ligament likely involved
What is the end-feel for a patient who has a meniscal tear?
Springy
What is the MOST specific "special test" for a Meniscal Tear?
Thessaly / DISCO Test

What is rehab progression limited by following a menisectomy?
Since nothing has technically been repaired (just removed), there are no WB restrictions
Delayed ________ is commonly seen with a meniscal / articular cartilage injury
Swelling
What precautions should we take if a patient has had a menisectomy?
While there are no strict limitations / restrictions (because nothing is being repaired), there are still some things we should limit / minimize
Minimize joint reaction force (use pain as our guide)
Prevent DVT
Decrease swelling
If a patient has a lot of swelling (acutely) following a menisectomy, what can we do to reduce this?
If someone does not have a good quad contraction what can be utilized to improve quadriceps activation?
Post-Menisectomy we should be checking ________
Why?
Patellar Mobility
Patiets who have had a menisectomy are likely to get PFPS; therefore want to make sure we keep patellar mobility
What are indications for a Meniscal Repair?
Younger Patient (< 50 y/o)
Concomittent Ligamentous Injury (e.g., ACL tear)
Tear is Reducible (""can we get the edges of the tear together?)
Red-to-Red Tear or Red-to-White Tear
Patient Compliance!
It is 4-6 months before patient can perform deep squats or running; therefore they ned to be willing to be compliant to these restrictions
What are Contraindications for a Meniscal Repair?
Older Patients (> 60 y/o)
Degenerative Tear (with poor tissue quality)
White-to-White Meniscal Tear
Patient Non-Compliance
Patient will not wait the proper 4-6 months before running, deep squats, etc.
Frontal Plane Positioning at the Knee / Lots of Varus or Valgus of the Knee
What are the ROM and Weight Bearing Restrictions following a Red-to-Red Meniscal Repair?
ROM
0-2 Weeks: 0 - 90 degrees flexion
Weight-Bearing Status
At first -- 50% WB in a long leg brace; patient will also be locked in extension whenever we are WB (we DO NOT want a flexion load on the knee)
Weeks 3-4: progress to full WB with brace still locked in extension
4 Weeks: unlock the brace to 90 degrees and promote equal weight bearing
Considering a Red-to-Red and a Red-to-White meniscal tear, when can Isolated Hamstring Activation occur?
Red-to-Red = ~6 weeks
Red-to-White = ~ 8 weeks
What are the ROM Restrictions following a Red-to-White or Complex Meniscal Repair?
Longer ROM Restrictions (compared to Red-to-Red)
2 Weeks: 0 - 90 degrees
4 Weeks: 120 degrees
6 Weeks: 135 degrees (OR equal to what the unaffected side is); essentially FULL ROM
** Even if the patient reaches their ROM goal early, make sure to keep them in their range!
When would a meniscal transplant (cadeveric donor) be the preferred method of treatment?
Performed for patients who have had multiple menisectomies and in patients who are younger

What is the time-frame for a patient to start running following a mensical transplant?
Patient can return to running at approx 12-16 weeks post-op
What is Reactive Effusion?
Swelling that is caused by re-introducing movements to ACL-R patients
Make sure minimize swelling as quick as possiblein order to prevent neurogenic inhibition
What can articular cartilage lesions occur as a result of?
Occur as a result of macrotrauma or summative microtraumas
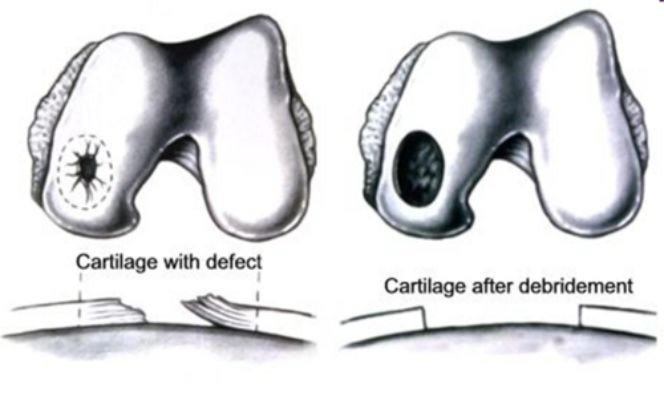
What is an Arthroscopic Debridement (of articular cartilage)?
The "first" and "easiest" method of repairing articular cartilage
Performed in there is fraying of the Articular Cartilage
The debridement will help to "clean up" the fraying / fibrillation of the tissue
How would you rehab an individual who has had an Arthroscopic Debridement of an Articular Cartilage Injury?
Treat just like a Menisectomy! Since the patient has not had anything repaired
What is a Microfracture Reparative Articular Cartilage Procedure?
Based on age, size, and location
The "second best option"
Typically performed in either:
Small Lesion in a high demand area; OR
Large Lesion in a low demand area
Small holes are drilled into the bone to expose mesenchymal cells and create bleeding for regeneration and fibrin clot / healing
What are the rehab precautions following a Microfracture Procedure?
WB Precautions for 6 weeks
Patient may be NWB
Want to be careful and avoid load / shearing as to not damage the fibrin clot
Patient Locked in Long Leg Extension Brace for 6 wks
In what patient population is a microfracture procedure most succesful in?
Younger Patients (< 35 y/o)
Smaller Lesion (< 2 cm)
Patients with Low BMI (< 30)
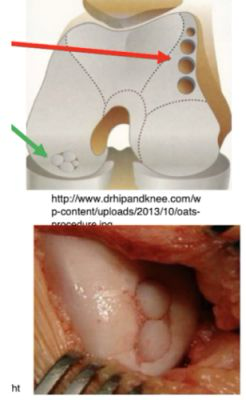
What is an Osteochondral Autograft Transfer System Repair (OATS)?
"Fill in the dot"
Take and harvest chondral / bone plugs from low demand areas (e.g., on top of femoral condyles)
These plugs are then placed in the lesioned area
True; ther are synthetic transfers where synthetic plugs are put in the harvest / donor sites (not sure how effective these are; did not talk about in class)
What are the rehab precautions following an OATS procedure?
Similar to Microfracture Procedure -- want to avoid shear and loading (so limited WB)
Perform OKC exercises prior to CKC exercises
What is an Autologous Chondrocyte Implantation (ACI) Repair?
Used to repair defects in the articular cartilage
Chondrocytes are harvest, spun, and then put in "re-grown"
The lesion is cleaned and the cells are injected (kinda like STEM cells) with a periosteal patch placed over the area
Idea is that hopefully this will regenerate the articular cartilage
When might an Autologous Chondrocyte Implantation (ACI) Repair be utilized?
Varying lesion sizes; 2 - 10 cm (small or large)
Femoral Condyle Lesions
Older patients (> 50 y/o)
Patients with failed microfracture, debridement, or OATS procedures
What are the rehab guidelines following an Articular Cartilage Repar Procedure?
6-8 Weeks NWB
Avoid flexion / ROM where you would engage the lesion (often ~30-70 degrees flexion)
Limit high-impact activities
Pts may have CPM for PROM and cyclic loading
Perform Isometrics (especially at 0 - 20 degrees flexion since minimal contact)
Can progress to ISO at 90 degrees flexion (because there is increased contact area here so force can be dispersed)
OKC in the range of 70-90 degrees
Following an Articular Cartilage Repair Procedure, rehab may be ________
6-9 months
What are the risk factors for Knee Osteoarthritis?
Older age
Female
Obesity (NOT a risk factor, but increases progression)
Osteoporosis (higher risk but slower progression since not not laying down chondrocyte lesions)
Occupation (higher incidence in populations with repetitive squatting, kneeling, and bending)
Sports with torsional loads, overuse, and high-impact
Previous Trauma
Muscle Weakness / Dysfunction
Proprioceptive Deficits
Genetic Factors
What are the criteria for knee osteoarthritis?
Crepitus
> 50 y/o
Tenderness along the joint line
Joint enalrgement (from excess bone)
Decreased joint space
Sclerosing (as seen on radiograph)
This would be more indicative of RA rather than OA
The ________ compartment of the knee is more likely to get OA
Why?
Medial
Medial compartment has greater compression / load (esp. with tibial adduction)
What are the different grades of DJD?
Loss of 1/3 Joint Space = Mild DJD
Loss of 2/3 Joint Space = Moderate DJD
Loss of > 2/3 Joint Space = Severe DJD
What are the different forms of conservative treatment that can be utilized for knee OA?
Physical Therapy
Weight Loss
Viscosupplementation
Corticosteroid Injections
What can be performed in Physical Therapy to conservatively treat Knee Osteoarthritis?
Activity Modifcation!
Instead of running --> water aquatics, elliptical, biking, etc. (to decrease load)
Strengthening and Stretching of the Quadriceps and Hamstrings
Mobilization or Traction at the Tibial-Femoral Joint
Both anterior-to-posterior and posterior-to-anterior
How can Weight Loss be a conservative treatment method for knee osteoarthritis?
Weight loss is helpful to decrease load and assists in decreases knee adduction moment/load
What is viscosupplementation? How can it be used as a conservative treatment method for individuals with knee OA?
Hylauronic Acid injection at the knee (usually a series of 3 injections)
HA helps with lubrication and shock absorption
Has been seen to be beneficial in the short-term (however, in the long-term, potentially not optimal)
May slow-down progression of OA (but not stop it)
True!
They do use it in the hip but it is considered an "off-label" use
How can corticosteroid injections be a conservative treatment method for knee osteoarthritis?
Corticosteroid injections helps with pain relief
However, in the long-term, may cause more harm than good as CS injections are non-selective (therefore causing damage to not only the "bad" areas but also the "good")
What is a Knee Unloader Brace?
3-point counterforce brace
Helps to unload the medial compartment of the knee by pushing the knee into a "valgus moment" (thus opening up the medial side and compressing the lateral side)
Should be worn throughout the day
Patient Compliance = Not Good
Knee brace is bulky and may feel "funny" because we do not typically walk with our knee in a valgus position

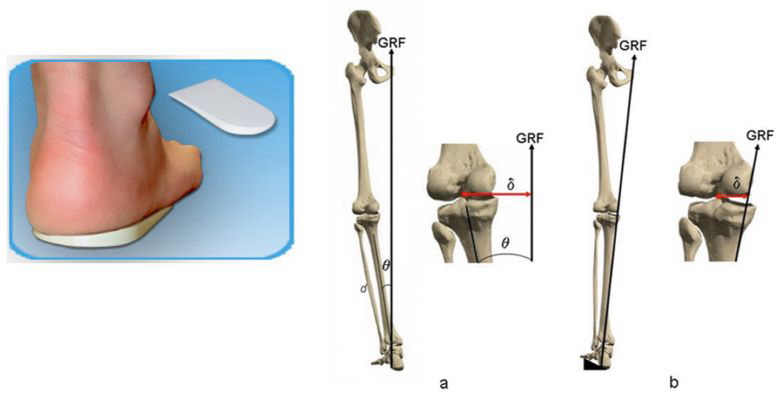
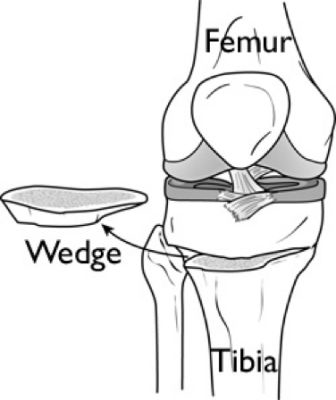
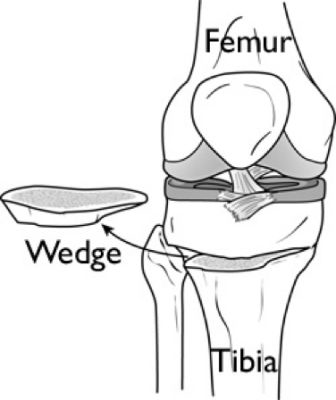
How can a Lateral Heel Wedge help with Knee OA?
Lateral heel wedge causes eversion at the rearfoot
Due to their being increased eversion, this causes increased pronation
This eversion and increased pronation causes an increased valgus moment (medial collapse)
This overall helps to decrease pain and changes the location of the GRF
What is a Hi-Tibial Osteotomy?
De-adducts the tibia
Puts the patient in a more "neutral-to-valgus" moment to help unload the medial compartment
What ligaments are spared with a Total Knee Arthroplasty?
Medial and Lateral Collateral Ligaments
However -- there is a PCL sparing technique now (so if utilized, the PCL can be spared as well)
What does rehab look for TKA patients?
Very Similar to the Hip!!
Get muscle activation
Quad sets, glute sets, HS sets, ankle pumps, etc.
Work on Mobility
STS and transfers
Patients should utilize the least restrictive AD (most often walker)
Patient might have CPM (depends on phsyician)
Patient will be in this for a lot of time
May need to educate these patients
Progress ~5 degrees per day based on patient tolerance
What do we need to consider for patients who are post-TKA? [Hint -- consider what PT would include in the hospital]
Make sure they are able to be mobilized
Do not want them still under anesthesia, have had pain medication recently, etc.
DVT Prophylaxis (TED Hose, SCD, etc.)
Integumentary Check
Incision and Swellling (observe odor, color, drainage, etc.)
Observe Quad Activation (quad sets, SLR)
Ask about Home Environment (steps, support available, etc.)
What are pre-operative predictors of TKA outcomes?
Age (e.g., 65 y/0 vs 105 y/o)
Pre-Operative ROM (if someone has limited ROM pre-op, we are not going to magically gain ROM post-surgery)
Pre-Operative Quadriceps Strength
Pre-Operative Level of Function
Self-Reported Disability Scores (lower = better)
What are post-operative predictors of TKA outcome?
Quadriceps Strength
Want to get early use of NMES and quad strengthening activities
Range of Motion
Full extension is top priority; want about 115 degrees of flexion
Realistic Expectations
If patient gets 110 degrees on table of surgery where they are sedated... going to be difficult to get to 120 degrees of flexion at therapy
Gait Symmetry
Decreased Hospital Stay
Patients post-TKA still have a patella and quad tendon (which can still get stiff!)
When would a Hemiarthroplasty be indicated?
If someone has a really "bad" or degenerated medial (or lateral) compartment, and the opposite side is OK
Typically performed in younger individuals (because it buys them more time before they need to get a TKA
What do we need to consider post-operatively for patients who have had a hemiarthroplasty?
Still in pursuit of full extension!
Want to get as much ROM as possible
No spacer in this patient
Patient typically has a quicker recovery (compared to TKA)
D/t patient population being younger and the surgery being less involved
Treat Impairments (strength, ROM, etc.)
What is a Baker's Cyst?
Fluid-filled sac in posterior portion of th knee
Occurs from swelling in the knee joint that gets pushed posteriorlhy
Typically seen in patients with recent trauma
TKA, Meniscal Injury, etc.
Patient complains of tightness, fullness, etc. in the back of the knee
Treatment
Typically calm down on its own (however if it doesn't, drainage may be option)
In regards to PT -- ROM + flexibility to decrease compression
What occurs with IT Band Syndrome at the Knee?
Most common in Runners!
Running on uneven surface
Increased intensity of running
Patient complains of lateral knee pain on gerdy's tubercle
When patient performs flexion ⇆ extension, the IT band moves anterior/posterior (""IT Band Friction Syndrome""
Flexion → Extension = IT Band Goes Anterior
Extension → Flexion = IT Band Goes Posterior
Around 20-30 degrees flexion is where it is the "worst"
What is the treatment for IT Band Syndrome (at the knee)?
Strengthen the TFL and Surrounding Structures
Soft Tissue Extensibility (e.g., quadriceps and hamstrings)
Realistically -- not gonna stretch IT band
Modify Running (probably by decreasing amount)
We cannot even tell these patients to go on the bike or elliptical because they are still performing flexion/extension movement pattern
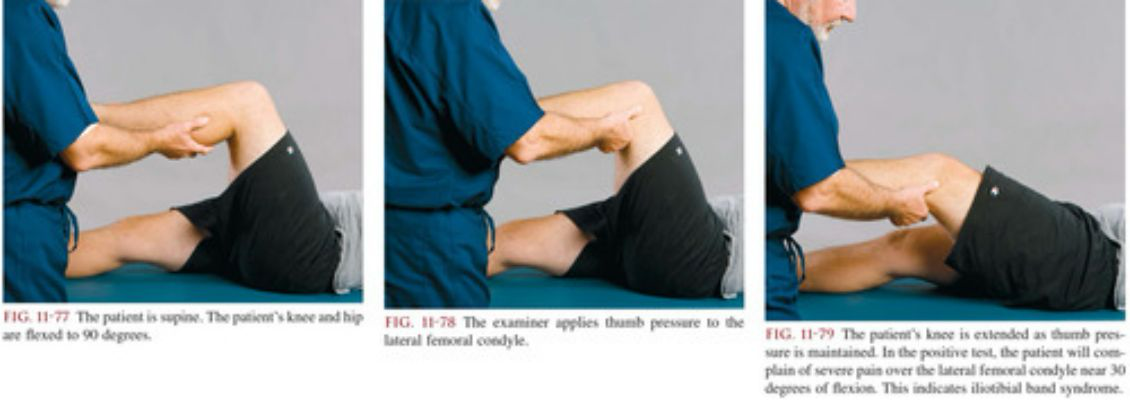
What special test can help diagnose IT Band Syndrome (at the knee)?
Noble's Compression Test!
Patient is supine on the table, bends their knee, and the PT palpates gerdy's tubercle
PT starts patient in knee flexed position and moves to extension while palpating for movement of the IT band
Positive = Reproduction of Pain / Symptoms
What is the ALS-RSI?
Measure of confidence that a patient has in the knee and abilities
Scored on a 0-10 scale
Increased Score = Decreased Fear (or greater confidence)
What is the Tampa Scale for Kinesiophobia?
Higher Score = Higher Kinesiophobia
If a patient has increased kinesiophobia, they are likely to not load the limb and have difficulty with returning to pre-injury level of function
What is the LEFS?
Performed when there is no ACL or ligamentous injury
Includes questions on the patient's ability to perform ADLs and some sport-specific questions
Grading Scale of 0-4 for each item
0 = Unable to perform
4 = No difficulty
Higher Score = Better