Nuclear Cardiology: Myocardial Perfusion Studies and Ventriculography
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
54 Terms
What is the main purpose of Myocardial Perfusion Imaging (MPI)?
To evaluate myocardial blood flow and detect ischemia/infarction
In MPI, decreased tracer uptake during both stress and rest indicates:
Myocardial infarction (fixed defect)
Decreased uptake at stress but normal at rest indicates:
Ischemia
The two essential conditions for detecting perfusion abnormalities are:
Increased coronary flow and proportional tracer extraction
During rest conditions, why might a stenosed artery appear normal on an MPI image?
At rest, myocardial demand is low and perfusion appears homogeneous
In stress imaging, coronary arteries normally:
Dilate 2–4× to increase blood flow
What does the size and location of a perfusion defect tell us?
Which coronary artery is affected and how severe the disease is
Which statement about tracer uptake is correct?
It’s proportional to coronary blood flow and viable tissue
In the schematic diagram, what causes the defect seen during stress imaging?
Limited vasodilation in stenosed arteries
What does MPI rely on to differentiate between normal and ischemic myocardium?
Disparity in blood flow between normal and underperfused tissue
Which type of emission releases two protons and two neutrons?
Alpha decay
Which radionuclide used in MPI decays by electron capture?
Tl-201
What type of decay produces positrons used in PET imaging?
Beta-plus decay
What do the short-, vertical-, and horizontal-axis views represent in cardiac SPECT imaging?
Cross-sections of the left ventricle in different orientations
In MPI, what does a perfusion defect that appears only during stress indicate?
Reversible ischemia
What is a bull’s-eye (polar) map used for?
To display LV perfusion distribution from apex to base
What is the typical rest and stress dosage for a Tc-99m dual-injection protocol?
8 mCi rest / 24 mCi stress
Why is the stress study often performed after the rest study?
To prevent high residual activity from affecting rest counts
What advantage does the stress–rest sequence have?
Useful when patient may not return for rest study
A Tc-99m Sestamibi SPECT study shows reversible perfusion defect in the lateral wall and transient LV dilation during stress. Coronary angiogram reveals distal LCX occlusion with good collateral flow at rest. What is the most likely explanation?
Reversible ischemia due to collateral insufficiency under stress
A fixed perfusion defect in the inferior wall that does not improve at rest represents:
Myocardial infarction
The papillary muscle appearing “too hot” can cause what type of image artifact?
False reduction of perfusion elsewhere due to normalization
Mild peri-infarct ischemia means:
Surrounding tissue has partial reversible ischemia
What coronary artery supplies the inferior and posterior septal walls?
RCA
What does a reversible Tl-201 defect indicate?
Viable ischemic myocardium
A defect that remains cold on delayed Tl-201 imaging represents:
Chronic infarction
What physiologic mechanism enables Thallium redistribution?
Active Na-K ATPase pump re-entry
Which finding implies hibernating myocardium?
Delayed “fill-in” on redistribution scan
LV dilation with mixed reversible and fixed defects suggests:
Ischemic cardiomyopathy with viable zones
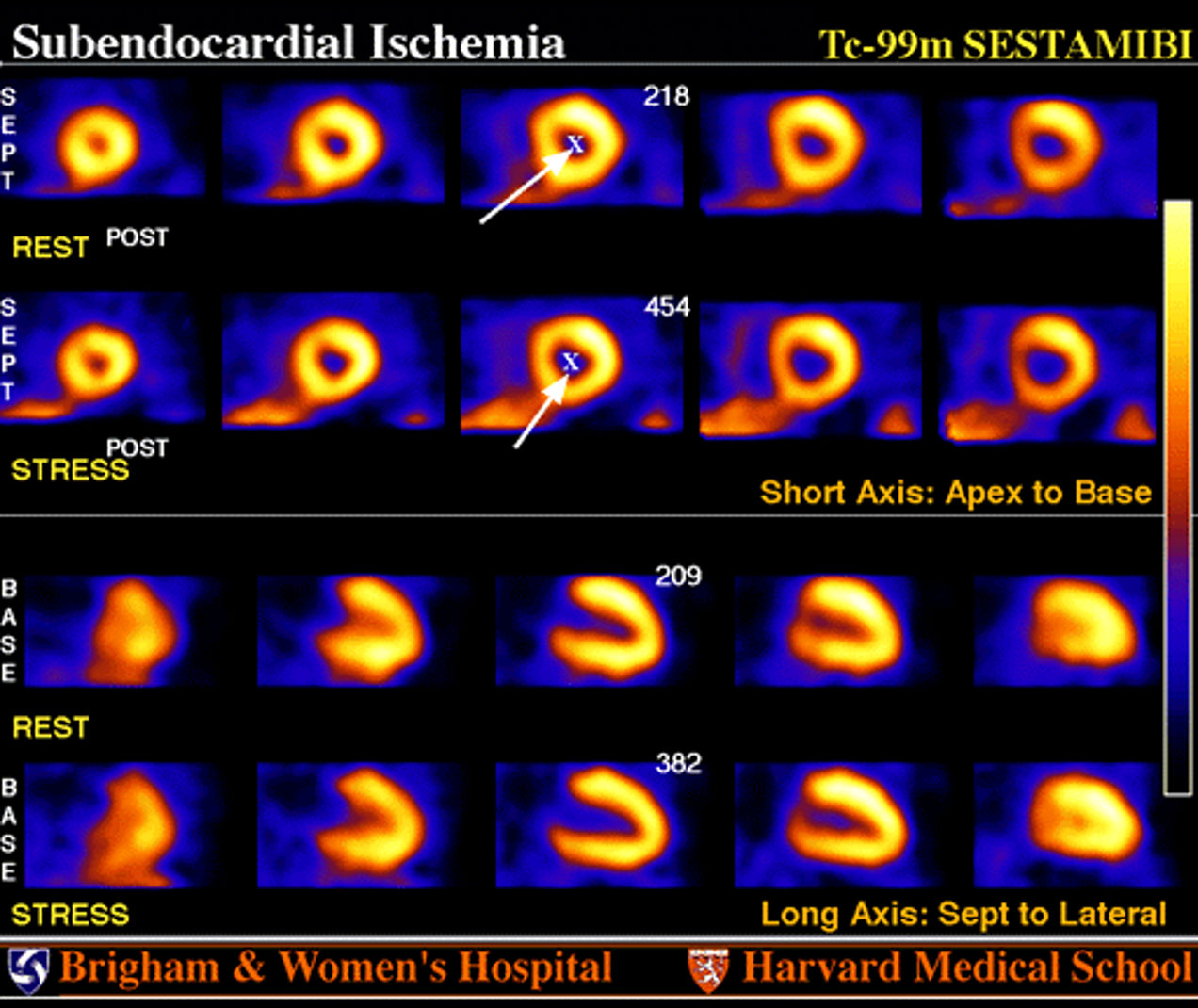
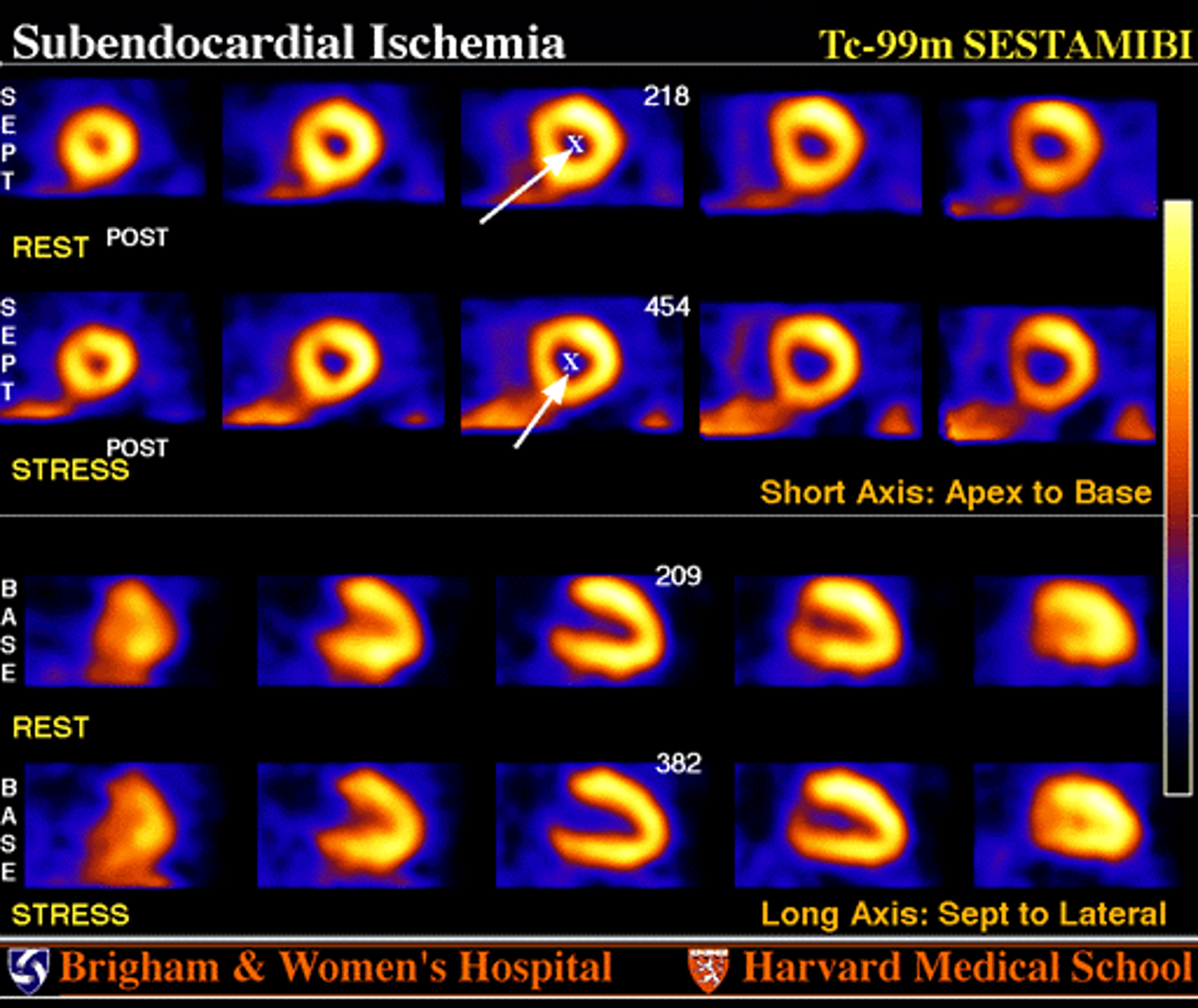
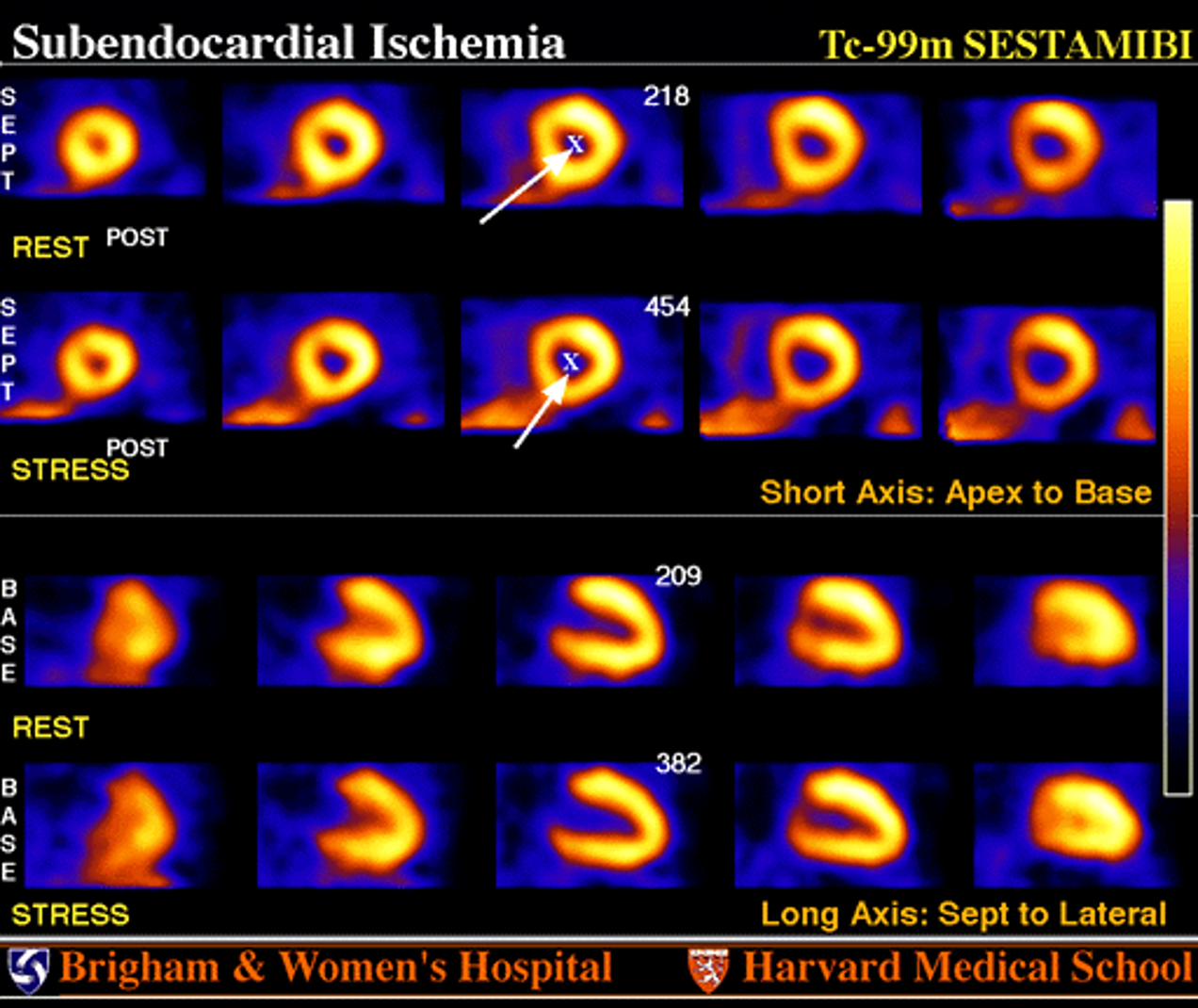
Which finding best supports global subendocardial ischemia?
Diffuse stress-related perfusion decrease with LV dilation
What is the most likely mechanism behind this patient’s ischemia?
Microvascular dysfunction + ↑ LV EDP
Which condition most commonly produces this pattern?
Hypertensive heart disease / LVH
What pharmacologic condition could mimic this finding?
Beta-blocker use during stress test (reduces coronary flow reserve)
Subendocardial ischemia usually shows what kind of LV change during stress?
↑ Volume (TID)
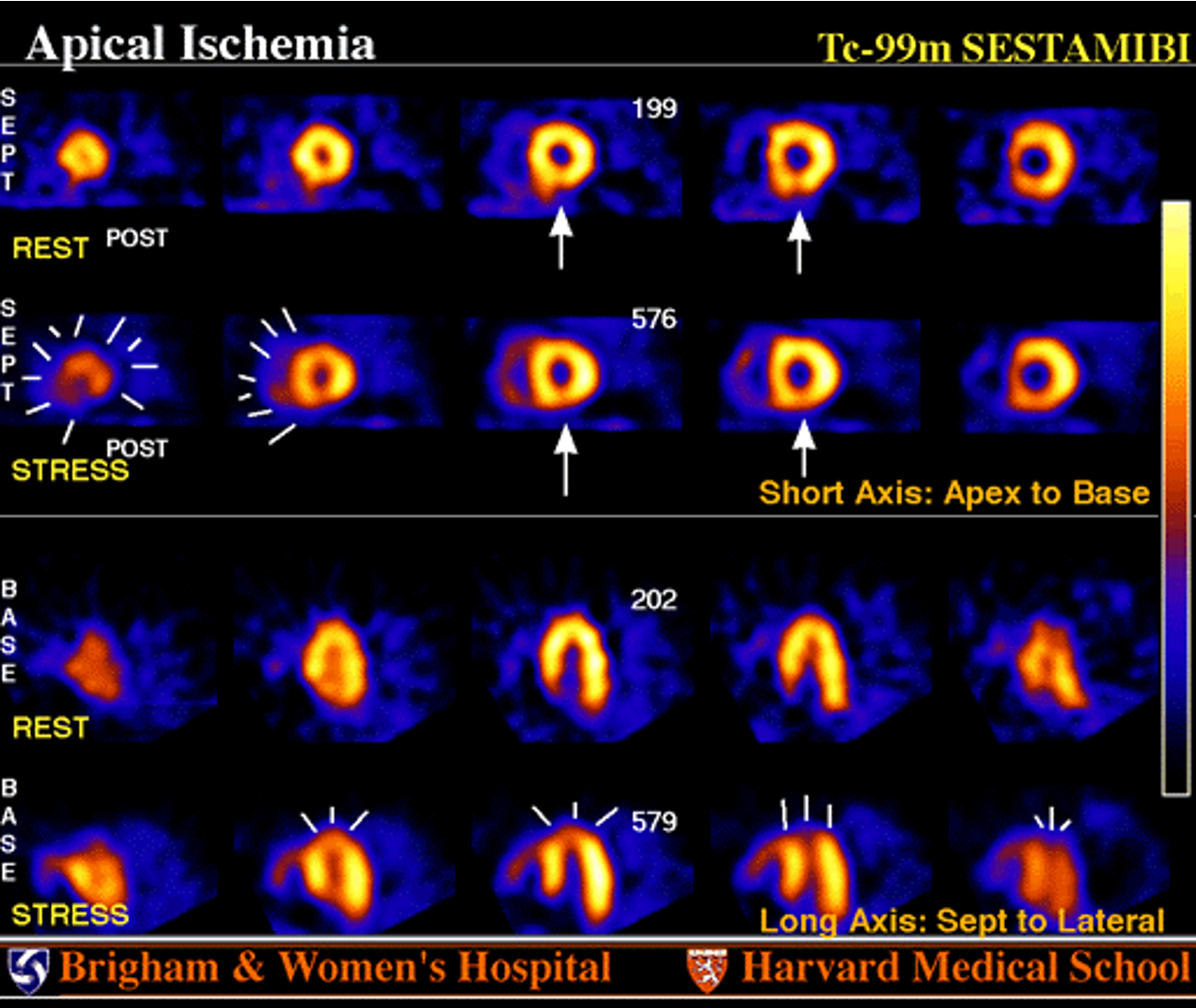
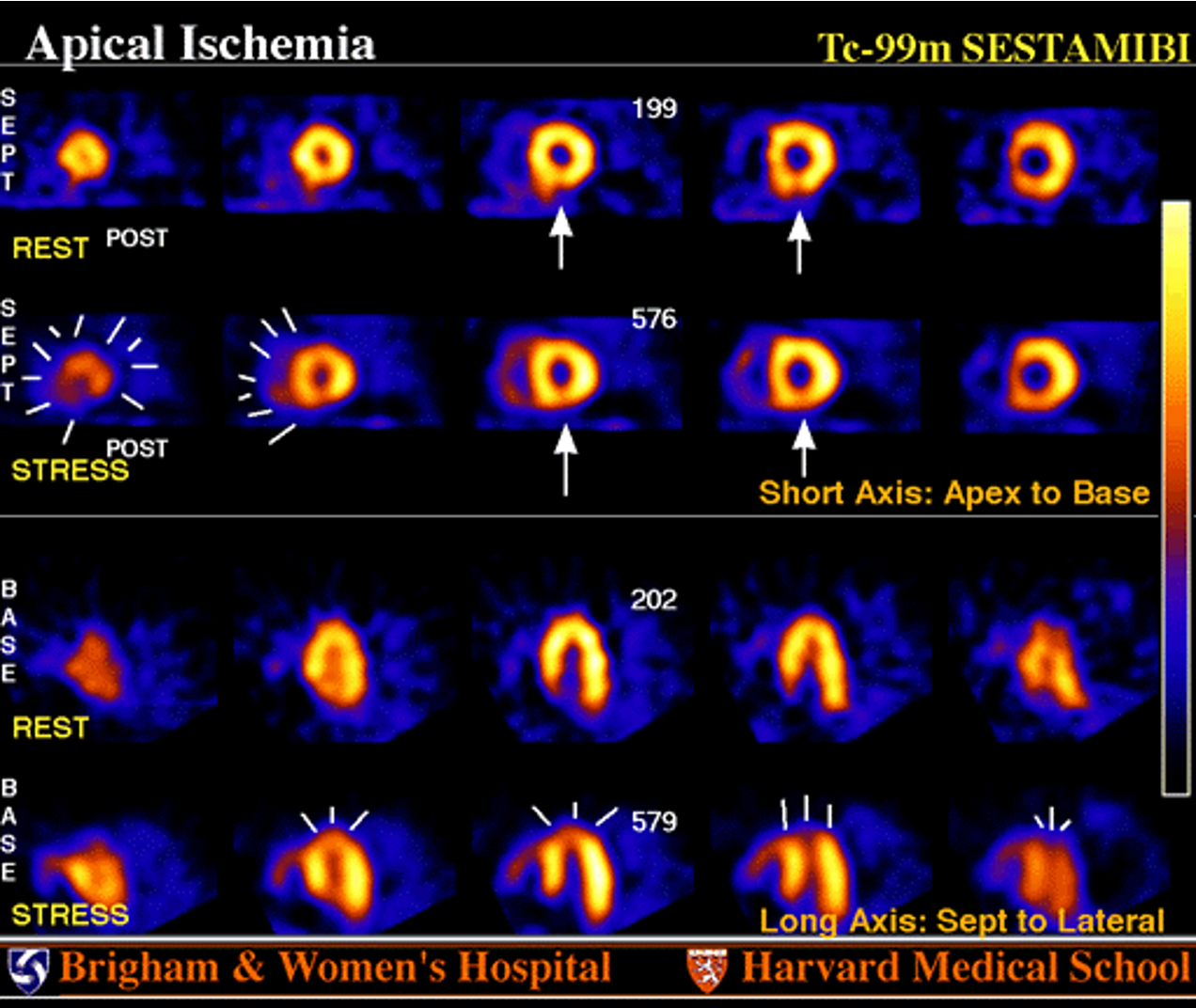
The reversible apical and septal defect corresponds to which coronary artery?
LAD
The inferior wall defect that persists at rest most likely represents:
Attenuation artifact
Collateral flow that maintains rest perfusion but fails under stress leads to:
Reversible ischemia
Which coronary lesion combination explains this pattern best?
LAD only
Why can coronary anatomy alone misrepresent ischemic severity?
Collateral pathways and microvascular flow alter actual perfusion
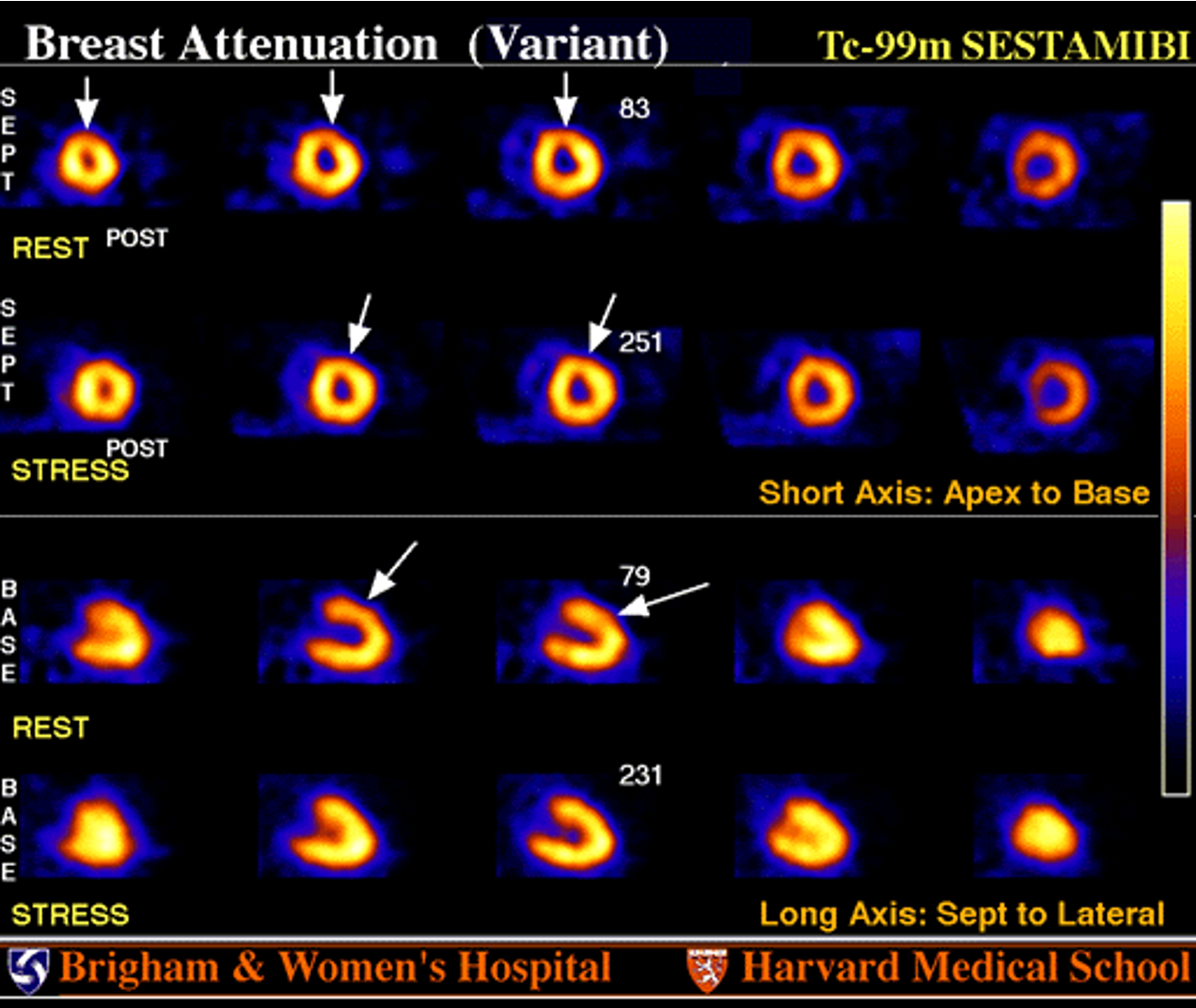
An anterior wall defect present on both rest + stress images but with normal wall motion likely represents:
Breast attenuation artifact
Breast attenuation usually affects which myocardial region?
Anterior/apical wall (12 o’clock)
Which imaging feature helps confirm attenuation rather than infarct?
Normal wall motion on gated SPECT
Which of the following best explains the mechanism?
Soft-tissue photon absorption over the LV
What imaging adjustment can help identify this artifact?
Prone or attenuation-corrected imaging ✅
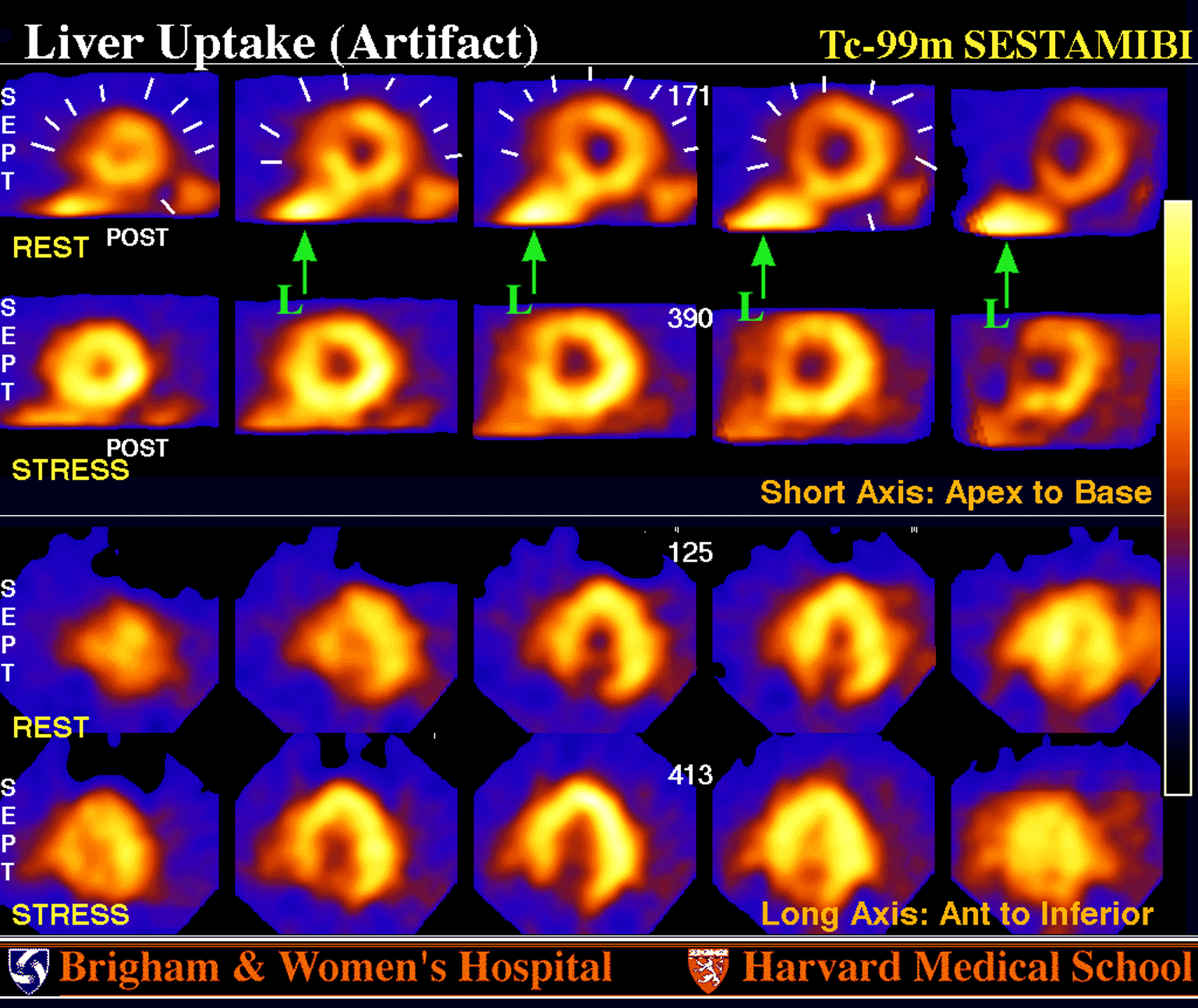
What caused the apparent global myocardial hypoperfusion?
Normalization to intense liver activity
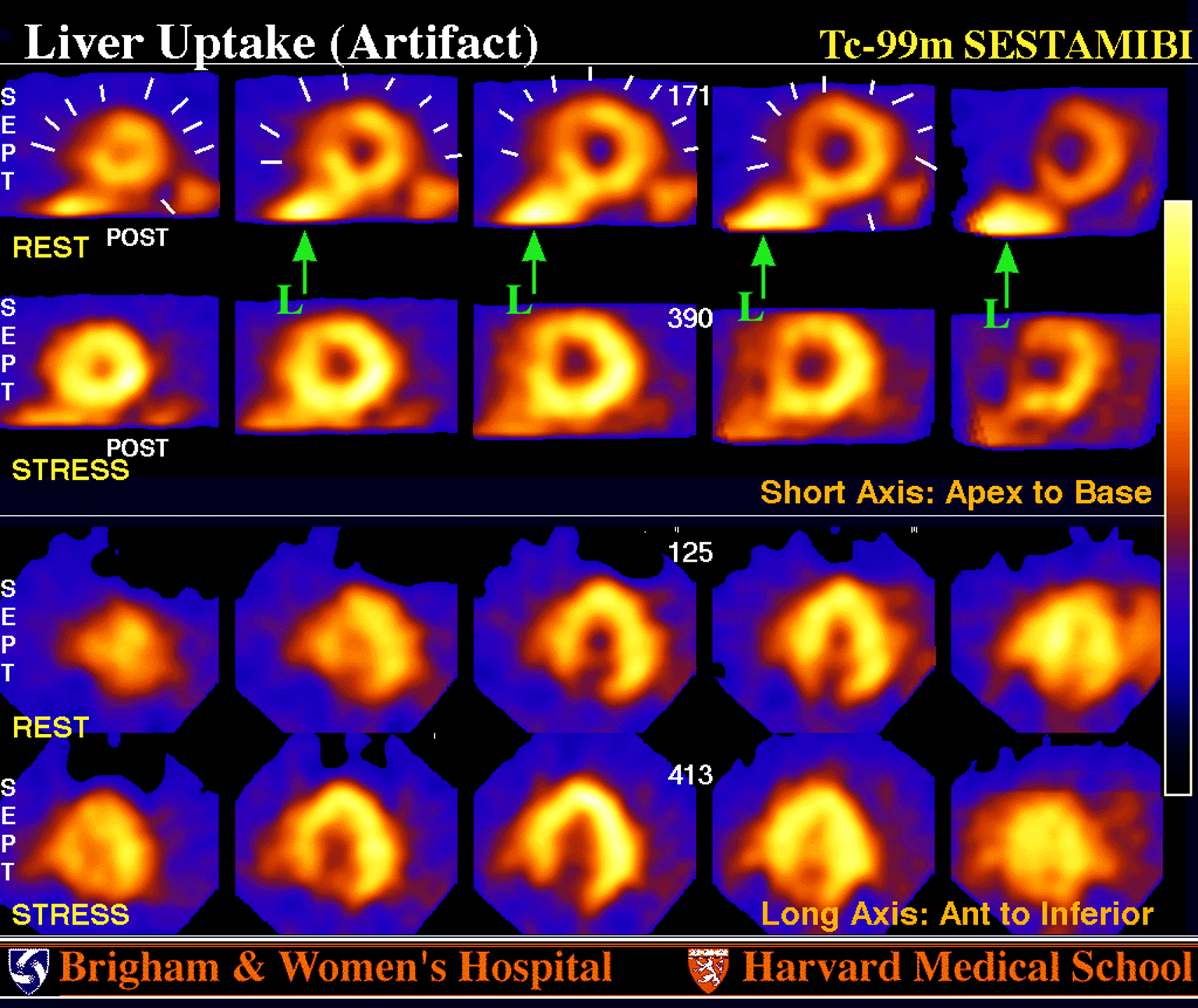
How can this artifact be prevented?
Delay imaging 45–60 minutes to allow hepatic clearance
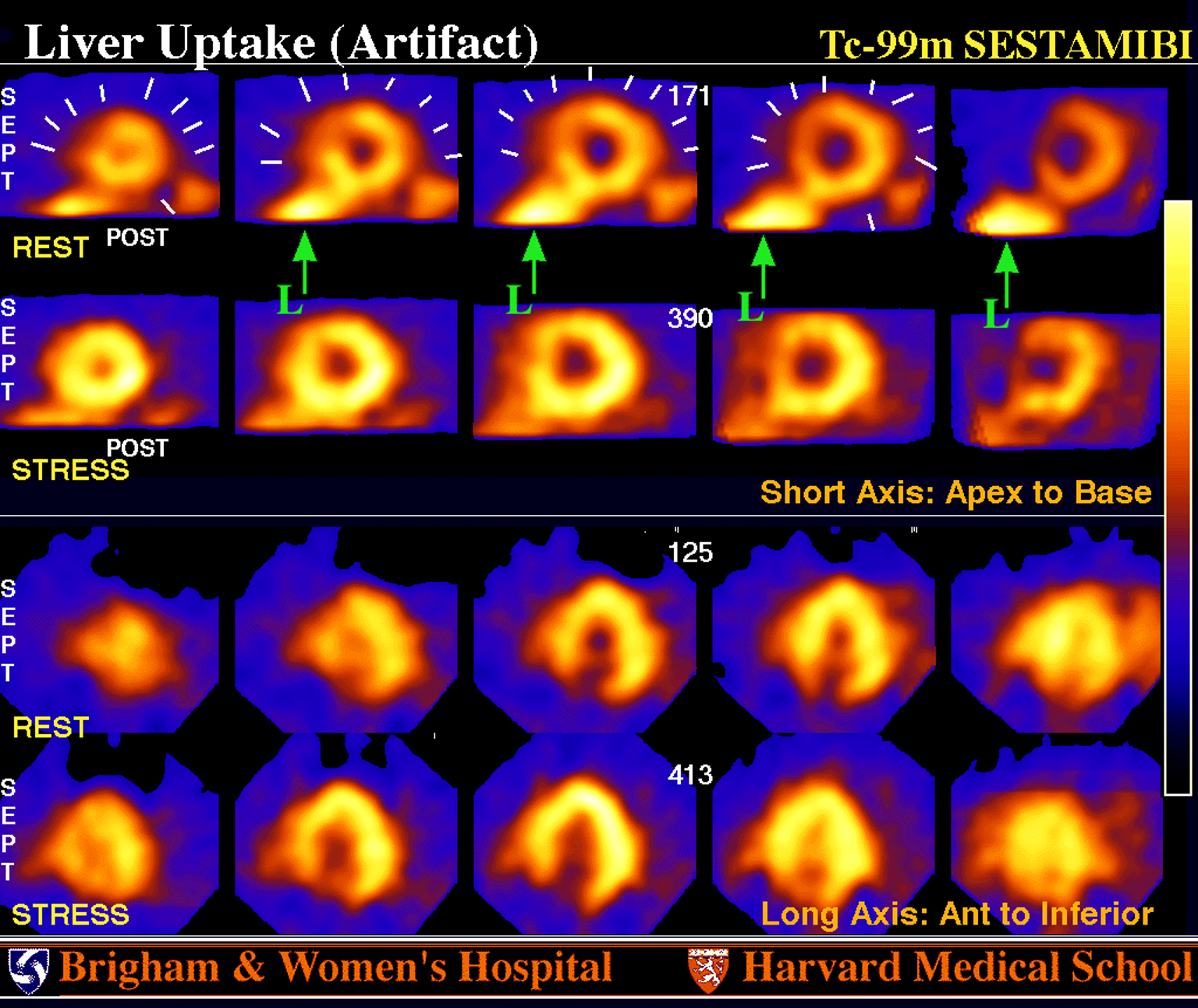
After reprocessing, a small fixed anterior-septal defect remains. What does this likely represent?
Mild non-transmural MI (LAD territory)
Why is LBBB a less likely cause here?
Because septal defect persists on rest only, not stress; no conduction abnormality present
What is the main clue that the defect was artifact-related?What is the main clue that the defect was artifact-related?
Normal perfusion restored after re-normalization to myocardium
What does MUGA primarily evaluate?
Cardiac function and wall motion
What radiopharmaceutical mechanism allows RBC labeling?
Reduction of Tc-99m pertechnetate by intracellular stannous ion
How many frames per cardiac cycle are typically acquired?
16–32
What is the primary advantage of MUGA over echocardiography?
High reproducibility of ejection fraction
What is the purpose of the beat rejection window?
To prevent temporal blurring from variable R-R intervals