GI path cont. and anatomy
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
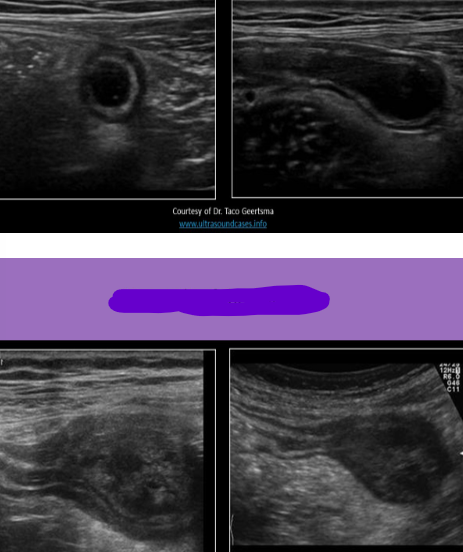
Mucocele of appendix
Appendix is obstructed by scarring or fecaliths
Isolated segment continues to produce mucus
Causes the formation of a retrocecal mass
Asymptomatic, 50% have palpable mass in RLQ
Usually benign
USA Mucocele
Elongated appendix filled with mucus
Variable internal echogenicity can calcs
Wall thickness an be normal or thickened
Onion signs - Layers of debris within the appendix appear similar to the layers of an onion
Mucocele of appendix
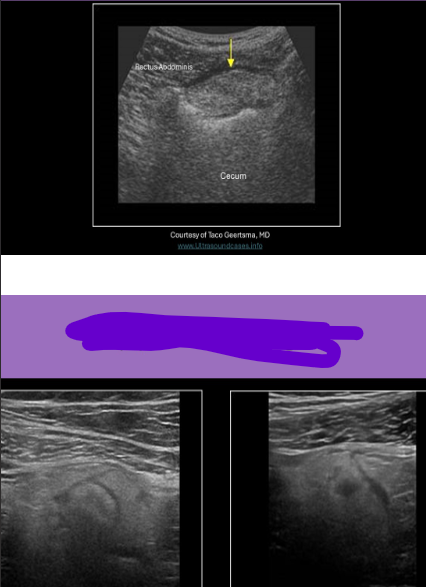
Epiploic appendagitis
Thick fatty strands that attach to the serosal surface of the colon
Torsion or thrombosis can cause ischemia or infarction of the appendage
Leads to localized inflammation and pain
Epiploic appendagitis USA
Echogenic finger-like projection from colon wall
The surrounding pericolic fat becomes thickened and echogenic
Can simulate appendicitis; must differentiate b/c the treatments are different
Look for wall layers that are seen with appendix
Epiploic appendagitis
Functional bowel obstruction
Paralysis of the muscle in the bowel wall, lack peristalsis
Mechanical bowel obstruction
Physical impediment to progression of the luminal contents
Causes of bowel obstruction
Material in lumen, intrinsic/extrinsic masses, and circulatory compromise
Number 1 cause of bowel obstruction
Adhesions
Bezoars are intraluminal masses of undigested material:
Concretions - Inorganic substances; medications, bubble gum
Trichobezoar - hairball
Phytobezoar - indigestible plant or vegetable materials (cellulose)
Lactobezoar - milk materials, seen in infants
Serious complication of bowel obstruction
Bowel ischemia
Ultrasound eval of bowel obstruction:
Describe location of gut loops
Eval the caliber of the segment and size of obstruction
Describe the contents of the segment; solid, fluid, gas
Assess peristalsis
USA bowel obstruction
Dilation of the GI tract proximal to the obstruction; >2.5cm is abnormal
Luminal contents tend to move to-and-fro within the lumen, instead of progressing forward
Visualization of the plicae circulares
Difficult to diagnose with US, assess GI tract caliber, content, peristalsis, site of liminal obstruction, location of gut loops
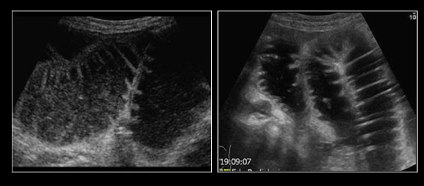
Bowel obstruction
Intussusception most commonly occurs at
Ileocecal junction in the RLQ
Most common cause of small bowel obstruction in children 6mo - 4yrs old
Intussusception
Intussusception
Usually the small intestine (ilem) involutes into the large bowel
Lymph nodes, mesentery and blood vessels can be pulled into the cecum
Causes anemia, dehydration, and leukocytosis
Severe pain with peristalsis, vomiting, blooD in rectum
Red currant jelly stool - contains a mixture of blood and mucus
Compression techniques used to eval
USA Intussusception
Non-compressibility of the affected segment
Telescoping segments demonstrate multiple concentric rings of tissue
Also described as a target or doughnut-shaped lesion in the transverse plane
Wall folded over on each other
Thickened walls
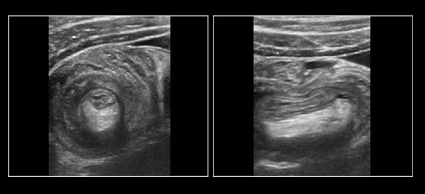
Intussusception
Midgut malrotation
Refers to any variation in the normal rotation and fixation of the GI tract during development
Associated with MALPOSITION of SMA and SMV
Varices are usually present
Left gastric vein is most common portosystemic collateral seen with malrotation
Midgut malrotation USA
Document the reversed position of the SMA and SMV
Doppler used to eval flow in the SMA, SMV and collaterals
Flow reversal occurs in the left gastric vein
Color Doppler can be used to assess loss of flow to wall

Midgut malrotation
Adenocarcinoma
Colon cancer is the 3rd leading cause of death from cancer
Increased CEA levels in blood
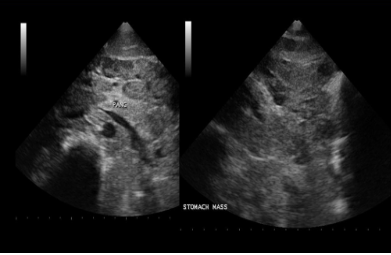
Gastric tumors usually arise in the pre-pyloric region, antrum, and lesser curvature
Most common location of colon cancer
Rectum
Most common malignant tumor of GI
Adenocarcinoma
USA adenocarcinoma
Solid intraluminal mass of varying echogenicity
Difficult to asses with US, but administering a water enema during the exam may help to visualize an intraluminal tumor or abnormality
Endoscopic sonography
Rotating high frequency transducer (7.5MHz)
Pt placed in LLD position
Used to localize and characterized benign masses
Also used to staging esophageal cancer and differentiation gastric lymphoma from gastric carcinoma
Lymphoma
May be primary or widespread dissemination
Nodular, ulcerative, or infiltrating
Common in AIDS pt
Lymphoma USA
Large hypoechoic ulcerated masses
Found in stomach or small bowel
Gas artifact or small bowel
Gas artifact seen within ulcerations
Mets of GI
Lung, breast, melanoma
Multiple small ulcerated nodules
Difficult to differentiate from primary carcinoma
Hodgkin lymphoma
Esophagus connects to the _______ of the stomach
Cardiac orifice
Valvulae conniventes
Intraluminal extensions/folds that increase surface area for absorption in the jejunum
What vitamin is produced by the colon
K
The wall of a normal distended bowl segment will demonstrate ______ layers and measure ____mm thick
5; <3
Hormones that stimulate the digestive system
Gastrin, secretin, cholecystokinin
Hematocrit can be tested to evaluate suspected ___________, while WBC levels can be tested to eval suspected __________
GI bleed; Infection
Graded compression and deep breathing can be used:
To displace gas out of the field of view
What causes stenosis in the median arcuate ligament syndrome
Compression
Which of the following indicates mesenteric ischemia?
Dilated IMA
Retrograde flow in the hepatic artery
Portal venous gas
All of the above
All of the above
The olive, doughnut and cervix signs are indications of:
Pyloric stenosis
Pts evaluated to pyloric stenosis are typically ________ in age and evaluated with US with the pt in the _______ position
2-10 weeks, Right lateral decubitus
Which of the following measurements should be obtained when evaluating a pt for suspected pyloric stenosis?
Muscle thickness, channel length, cross sectional thickness
What is evaluated on pts with suspected inflammatory bowel disease?
Fecal testing
Creeping fat and pseudokidney sign are findings associated with:
Crohn disease
Acute RLQ pain is commonly associated with_______, while acute LLQ pain is commonly associated with _______
Appendicitis; diverticulitis
Which of the following correctly described ulcerative colitis?
Associated with Marfan syndrome
Usually affects jejunum
Causes portal venous gas
All of the above
Causes portal venous gas
The normal appendix is identified posterior to the ___________ and anterior to the _________
Terminal ileum; iliac vessels
Appendix can be obstructed by:
Fecalith, corprolith, stercolith
Primary purpose for using graded compression during US eval of GI tract
To cause peristalsis
If the appendix is obstructed by a fecalith, a _________ typically forms
Mucocele
Epiploic appengitis is most likely to be mistaken sonographically for________
Appendicitis
How can you differentiate epiploic appendagitis from appendicitis?
Document gut wall signature