biopsychology 2
1/40
Earn XP
Description and Tags
with evaluation
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
41 Terms
name the 4 types of examination
post-mortem examination
fMRIs
EEGs
ERPs
what is a post-mortem examination?
dead person who had unusual characteristics in life is physically examined through anatomical and neurochemical examinsations
allows us to see the amount of neurotransmitters present when they died
name 2 strengths of post-mortem examinations
can provide access to areas others can’t
detailed anatomical structure and neurochemical aspects
access to hypothalamus and hippocampus- allows deeper understanding
found patients with schizophrenia had more dopamine in the limbic system which prompted research into treatments using this
research into broca’s area
the only word this man could say was ‘tan’
when he did a post-mortem showed a tumour in his broca’s area which damaged it
led to learning that speech is produced in the broca’s area which allowed for more research
name 2 limitations of post mortem examinations
hard to establish causation
confounding variables make it hard to establish causation.
e.g. age, cause of death, medication taken, time. between death and examination
lack of function may not be due to deficits in the brain. deficits or lack of function could be due to other illnesses or have occurred during death
ethical issues
mostly done on patients with severe psychological deficits like HM. they might not be able to give fully informed consent- e.g. HM might not be able to consent due to amnesia but one was still done
counterpoint: even though they’re invasive, they patient is dead so it doesn’t matter
explain fMRIs
measures blood flow in the brain during specific tasks
neurons use more oxygen when doing a task, so oxygen in that area is reduced.
this changes the magnetism of that part of the brain
this creates a 3D image of the brain
name 2 strengths of fMRIs
non-invasive
doesn’t involve radiation or cutting into the brain so they are harmless- unlike PET scans.
they are risk free so more patients are likely to do it, which means more data to help understand the braingood spatial resolution
can be very specific and pick up small areas in the brain
allows psychologists to discriminate between regions with greater accuracy1-2mm resolution- significantly greater than EEGs and ERPs
name 2 limitations of fMRIs
poor temporal resolution
can’t detect very quickly- delay of 1-4 seconds between when you do something and when the scan picks it uo
EEG and ERP have 1-10 milliseconds
makes it harder to predict accurately the onset of brain activity
correlation not causation
only scans blood flow so it’s impossible to infer causation at a neural level
blood flow may indicate activity within brain area but we are unable to conclude that that’s definitely associated with the particular function
can only show localisation of function within the brain area- can’t show communication that takes place which might be necessary for neural functioning
what is an EEG?
measures electrical activity in the brain
electrodes are attached to the scalp with a skull cap
brain waves are shown and displayed on a graph
4 brain waves associated are: alpha, beta, theta and delta
what are the brain waves associated with EEGs?
alpha, beta, theta and delta
what are ERPs?
electrodes are attached to the scalp using a skull cap
stimulus is presented to ppt- e.g. asked to look at a picture
researcher looks for activity triggered by stimulus
has to be repeated to avoid anomalies
what is the difference between EEG and ERPs?
EEG- no stimulus
ERP- stimulus
what are the 2 strengths of ERPs and EEGs?
non-invasive
it does not involve raditation or cutting into the brain
they are harmless unlike PET scans and risk free so they are more likely to get people to do it = more data
counterpoint: electrodes attached to the scalp is uncomfortable which means discomfort could affected the cognitive responses- FMRI doesn’t have this issue
good temporal resolution
detects very quickly and there is no delay between when you do something and when the scan receives. scans every 1-10 milliseconds
name 2 limitations of ERPs and EEGs
poor spatial resolution
can’t be very specific in where they pick up from and can’t access in depth areas to predict accurately where it’s coming from. can discriminate regions with greater accuracy. fMRIs don’t have this issue
correlational rather than causation
only scans brain waves so it’s impossible to infer causation at a neural level
waves may indicate activity within brain area but we are unable to conclude that that’s definitely associated with the particular function
can only show localisation of function within the brain area- can’t show communication that takes place which might be necessary for neural functioning
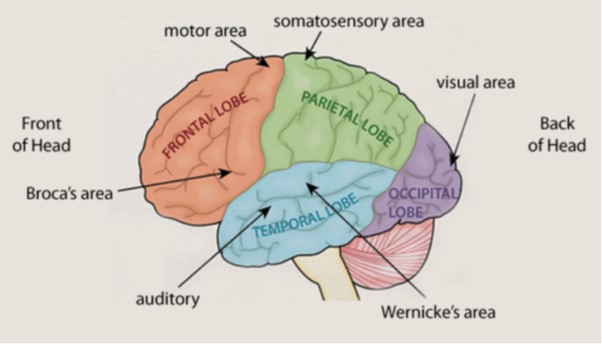
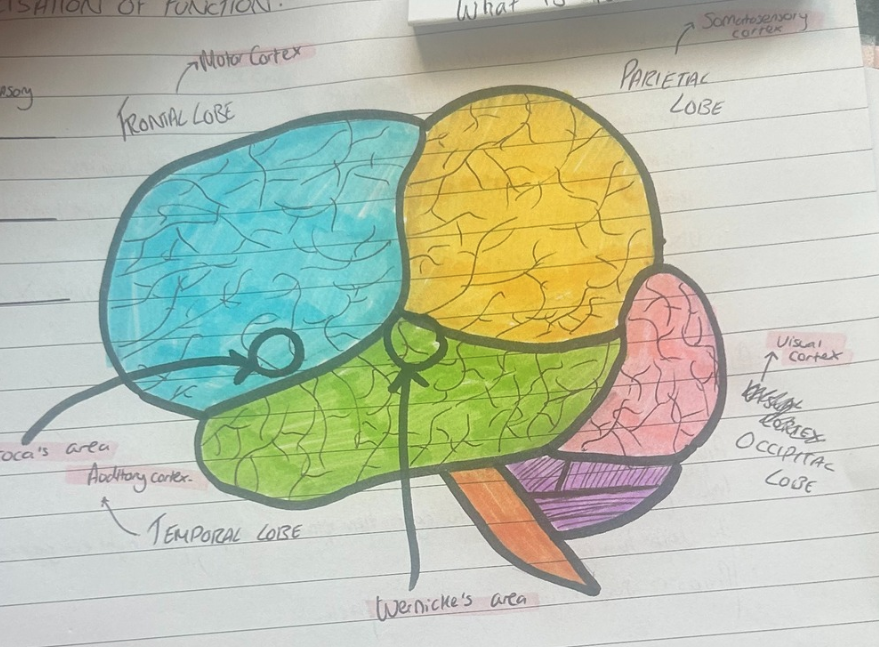
label broca’s area and wernicke’s area
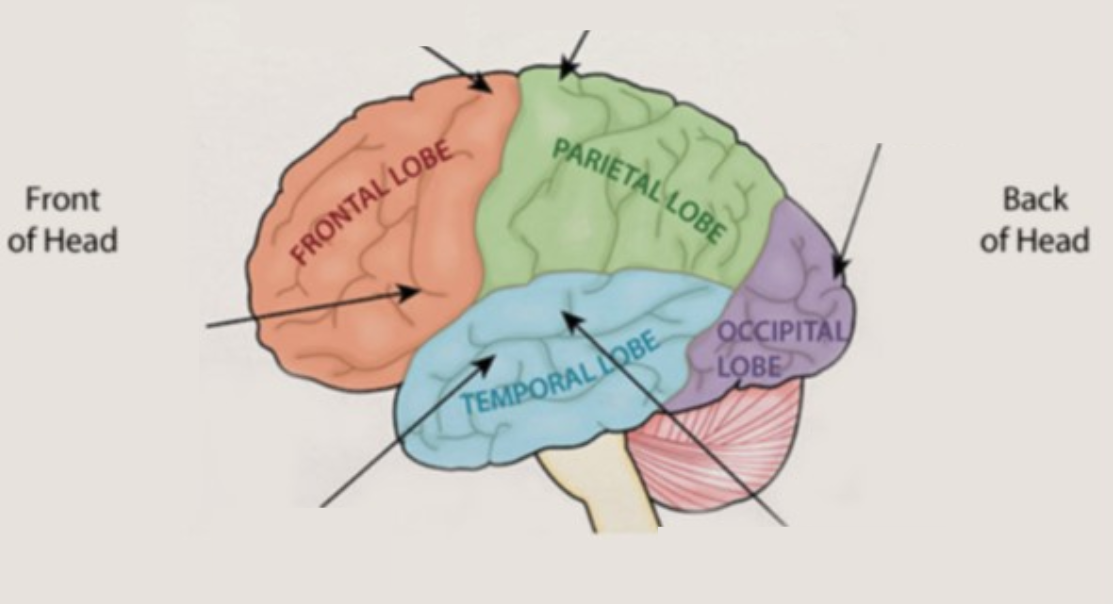
label the brain
what does localisation mean?
main functions are found in certain areas of the brain
shown by case study of phineas gage:
iron rod when through the brain and took some of the left frontal lobe
he experienced drastic personality change- e.g. impulsiveness, irritability and disrespectful
believed damaged area was responsible for emotion and personality
what is the motor cortex?
located in the frontal lobe
in charge of voluntary movements by sending signals in different parts of the body
discovered that different muscles are coordinated by different areas of the motor cortex by electrically stimulating motor area of dogs
this resulted in muscular contractions in different areas of the body depending on where the probe was inserted
regions of motor area are arranged logically- e.g. region that controls finger is beside the region that controls the hand and the arm and so on
what is the somatosensory cortex?
located in the parietal lobe
receives sensory information from skin to produce sensations related to things like temperature
different parts of the area receive messages from different body parts
this area was found to be highly adaptable- e.g. braille readers have larger areas for fingertips than non-braille readers (demonstrating plasticy of the brain)
what is the visual cortex?
located in the occipital lobe
receives and processes visual information
information from right visual field is processed in the left hemisphere’s visual area
information from the left visual field is processed in some of the right hemisphere’s visual area
visual area contains different parts which process different aspects of the information- e.g. shape, colour, size, movement
what is the auditory cortex?
located in the temporal lobe
analyses and processes acoustic information
information from left ear goes to right hemisphere
info from right ear goes to left hemisphere
processes sounds, volume, tempo and pitch
where are language areas?
only in the left hemisphere
name the 2 language areas and what they do
broca’s area- speech production
wernicke’s area- speech comprehension
explain broca’s area
speech production
discovered this area while studying patient known as tan
tan could understand language spoken to him perfectly but he couldn’t produce any coherent words and could only say ‘tan’
post mortem examination showed a tumour in his left frontal lobe
led to conclusion that broca’s area is responsible for speech production
people will damage to this area experience broca’s aphasia (slow and inarticulate speech)
what do people with damage to broca’s area experience?
broca’s aphasia
slow and inarticulate speech
explain wernicke’s area
speech comprehension
patients with damage to wernicke’s area were still able to speak perfectly well but can’t understand what they or anyone else said
this is known as wernicke’s aphasia
name 2 strengths of localisation of brain functions
supporting evidence
case studies on people with broca’s aphasia have damage to broca’s area and some with wernicke’s aphasia have this damage too
show the important role played by these brain regions for speech production and comprehension
phineas gage- showed important proof of localisation- most of frontal left lobe was removed by iron rod and he experienced drastic personality changes
counterpoint: evidence is based off case studies alone
case studies are done on small groups and therefore cannot be assumed just because their brain functions like that everyone else’s does
doesn’t allow for generalisations
phineas gage- may have had a personality change but that doesn’t mean everyone would + anger could be due to anger at the accident rather than damage to the brain
evidence from brain scans
showed area that was active during listening task was wernicke’s area and broca’s area was active during speaking and reading tasks
showed scientific proof that that brain function is localised in one place
tulving- brain scans showed episodic and semantic memories are stored in different parts of the pre-frontal cortex
scientific and objective support
name 2 limitations of localisation of brain functions
contradicting evidence
lashley- showed higher cognitive functions are not located in single parts of the brain.
removed 10-50% of cortex in rats that were learning to complete a maze
it did not make any difference to their learning which part of the brain was removed and their ability to learn wad damaged despite what part was taken
concluded its not any part of the brain responsible but the entire brain for higher functions + motor and sensory functions are localised but higher mental functions aren’t
dronkers- conducted MRI scans on Tan’s brain to confirm broca’s findings. Found damage in other area’s which may have contributed to the failure in speech production too. broca’s area may be involved in speech production but might not be the only region responsible
patients with broca’s aphasia may have damage to neighbouring areas of the brain
brain functioning is not fixed
lashley- brain has some degree of plasticity
undamaged parts of the cortex can take over specific cognitive functions after a brain injury/damage
suggests function isn’t localised if other uninvolved parts of the brain can take over and do those functions + suggests brain can recognise a lost function
there are limits to recovery but stroke patients have shown brain does have some plasticity
what is hemispheric lateralisation?
two halves of the brain are almost independent of each other- only joined by the small carpus callosum
they are functionally different
left= language
right = visual motor tasks, spatial awareness and facial recognition
what does the left side of the brain control?
language
what does the right side of the brain control?
visual motor tasks and spatial awareness and face recognition
what area allows the left and right side of the brain to communicate?
corpus callosum
what does contralateral control?
right hempishere controls left side of the body
left hemisphere controls right side of the body
what happens when the two hemisphere’s connection is cut during surgery? why would this happen?
two hemispheres can no longer communicate with each other
known as split-brain patients
used for very severe epilepsy
explain split-brain research
first to investigate hemispheric laterisation using split brain patients
wanted to examine the extent to which the hemisphere’s are specialised for the function
word/image was projected to the patient’s left visual field (processed in right hem) or their right visual field (processed in left hem)
when info is presented to one hem the information cannot be transferred to the other in split brain patients
used 11 split brain patients as ppts and had them do different tests
visual: picture was presented to ppts left or right visual field and they just had to describe what they saw
touch: object was placed in patient’s left or right hand (which was hidden from their view) and they had to describe what they felt or select a similar object
drawing: ppts were presented with a picture in either left or right field and they had to draw what they saw
results:
visual: ppt could say what the object was when it was in right visual field (bc lang is on the left) but not when it was in the left visual field
touch: object held in the right hand they could name but not in the left hand (lang is on left)
drawing: saw picture on the left visual field was drawn correctly- left hand could draw correctly (interpreted by right visual cortex) but the right hand couldn’t. if the right visual field had picture, the opposite was true
why does the brain change?
due to learning, experience, aging and injury
what is brain plasticity?
brain’s ability to change and adapt because of new experience, learning, injury, etc
brain continues to create new connections between different structures in the form of neural pathways
and alter existing pathways in response to changies
what happens to your brain from birth until 3
develops thousands of synaptic connections which connect with other neurons
continue to develop continues until 3
as we get older, the number of connections decreases as the ones we don’t use disappear and the ones we use a lot are strengthened
when can synaptic connections and neural pathways develop or decline?
at any point in life
what is functional recovery?
transfer of functions from a damaged area of the brain after a trauma to other undamaged areas
can do this through neural unmasking- where dormant synapses open connections to make up for nearby damaged areas
new connections recover any damage in specific regions
how does functional recovery occur?
brain seems to be able to rewire itself and reorganise itself following trauma by making new synaptic connections or by using connections that have been dormant for a while
connections that would not usually perform that function are activated and enable the function to continue
results in change of brain tissue structure
what brain structure tissue changes occur?
axonal sprouting- where damaged neurons make new axons to reconnect with undamaged neurons to rejoin/form pathways
recruitment of other brain areas- similar brain structures on the opposite side if the brain perform the function of the damaged area- e.g. if left motor cortex was damaged, the right motor cortex could take up the job of coordinating impaired movement