Late Pregnancy Complications
1/121
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
122 Terms
What is chronic hypertension in pregnancy?
>140/90 mmHg before pregnancy or before 20 weeks gestation
What is gestational hypertension?
New onset HTN after 20 weeks gestation without proteinuria
When is antihypertensive medication indicated in pregnancy?
Persistent SBP >160 or DBP >110
What are the first line antihypertensive medications in pregnancy?
Labetalol, Nifedipine, or Methyldopa
What is preeclampsia?
New onset HTN after 20 weeks with proteinuria OR evidence of end-organ dysfunction/severe features
What are the high-risk factors for preeclampsia?
Preeclampsia in a past pregnancy, multifetal gestation, chronic HTN, diabetes, antiphospholipid antibody syndrome
What are the diagnostic requirements for preeclampsia?
BP ≥ 140/90 mmHg on at least 2 occasions, at least 4 hrs. apart
What constitutes proteinuria in preeclmapsia?
- excretion of 300mg protein or higher in 24hrs
- Spot urine protein/creatinine ratio of ≥ 0.3
How should the fetus be monitored in preeclampsia?
ultrasound every 3 weeks (weight, growth, amniotic fluid volume) and fetal non-stress test twice weekly
What are the severe features of preeclmpsia?
- BP ≥160/110
- Platelets <100,000
- Creatinine >1.1
- Pulmonary edema
- headache/visual symptoms
- elevated AST/AST
- persistent RUQ/epigastric pain
What is the treatment for severe preeclampsia?
IV hydralazine or labetalol (Target SBP 140-150 and DBP 90-100) and Magnesium sulfate (IM or IV)
What is HELLP Syndrome?
hemolysis, elevated liver enzymes, low platelets occurring in patients with preeclampsia/eclampsia
How is HELLP Syndrome diagnosed?
- LDH ≥600 international units/L
- AST and ALT elevated x2
- Platelets < 100,000
What is the #1 medical complication in pregnancy?
Gestational Diabetes
What are the risk factors for gestational diabetes?
obesity, family hx, > 25, previous hx, infant weighing > 8lbs 13oz at birth (>4,000g), repeated spontaneous abortions
How is gestational diabetes diagnosed?
≥ 2 abnormal results on a glucose tolerance test (≥ 130-140)
What are the complications of gestational diabetes?
macrosomia, placental abruption, congenital anomalies, prematurity, fetal demise, and preeclampsia
What are the glucose goals in gestational diabetes management?
Fasting levels: < 95 mg/dL
1-hour post prandial: < 140 mg/dL
What is the first line treatment for gestational diabetes management?
Insulin (does not cross placenta)
What delivery plans are in place for gestational diabetes?
Diet-controlled: delivery by 40 weeks 6 days
Medication-treated: deliver around 39 weeks
What is the postpartum follow-up for gestational diabetes?
Glucose tolerance test 4-12 weeks postpartum and every 1-3 years thereafter
What is Premature Rupture of Membranes (PROM)?
rupture of chorioamniotic membrane before the onset of labor after 37 weeks gestation
What is it called when PROM occurs before 37 weeks gestation?
Preterm Premature Rupture of Membranes and is the leading cause of neonatal morbidity and mortality
What are the risk factors of PROM?
BV/STI, chorioamnionitis, short cervical length, 2nd/3rd trimester bleeding, low body index, and smoking
What is the clinical presentation of PROM?
"gush" of clear or pale-yellow fluid from the vagina
How is PROM clinically evaluated?
Speculum exam only to reveal amniotic fluid draining from vercial os or pooling of fluid in the vaginal fornix
What diagnostics are used for a PROM suspicion?
Nitrazine test: pH > 7.1 is consistent with alkaline amniotic fluid
Fern Test: amniotic fluid is placed on a slide to observe for pattern

What is the management of PROM?
proceed to delivery, provide GBS prophylaxis, administer corticosteroids if between 34-36 weeks
What is chorioamnionitis (intra-amniotic infection)?
Infection of the placenta and amniotic fluid that poses a major threat to mother and fetus
What are the symptoms of chorioamnionitis?
Fever ≥ 100.5° F, tachycardia, uterine tenderness, spontaneous and dysfunctional labor
What is the treatment for chorioamnionitis?
Deliver baby and IV antibiotics
What is Preterm Labor?
Regular uterine contractions before 37 weeks & are associated with cervical changes; can be spontaneous or indicated
What are the risk factors for preterm labor?
prior hx, multifetal gestation, social determinants, low maternal weight, smoking
What are the symptoms of preterm labor?
cramps, backache, abdominal/pelvic pressure, increased vaginal discharge, uterine contractions
What are the complications of preterm birth?
respiratory distress, intraventricular hemorrhage, necrotizing enterocolitis, sepsis, neuro impairment, seizures, CP
When are corticosteroids indicated for preterm labor management?
24-34 weeks gestation if at risk of preterm birth within 7 days
What is the role of tocolytics in preterm labor management?
prolong pregnancy for up to 48 hrs. to administer corticosteroids
What are the types of tocolytics?
Nifedipine (CCB), NSAIDS, and Β-Adrenergic receptor agonist (Dopamine)
What is a postterm pregnancy?
Pregnancy lasting 42 weeks of gestation or beyond
What are the risks associated with postterm pregnancy?
increased maternal vaginal trauma, labor dysfunction, morbidity and mortality for mother and fetus
What are the associated conditions with postterm pregnacy?
Macrosomia (infant size ≥ 4,500 g), meconium aspiration syndrome, dysmaturity syndrome, oligohydramnios (amniotic fluid index < 5cm)
What is the management for postterm pregnancy?
Induction of labor at 41 weeks and antepartum fetal surveillance
What are the two most common causes of significant third trimester bleeding?
Placenta previa and abruption
What physical exam component should be avoided in third trimester bleeding?
Bimanual pelvic exam should NOT be done until placental position can be confirmed on US
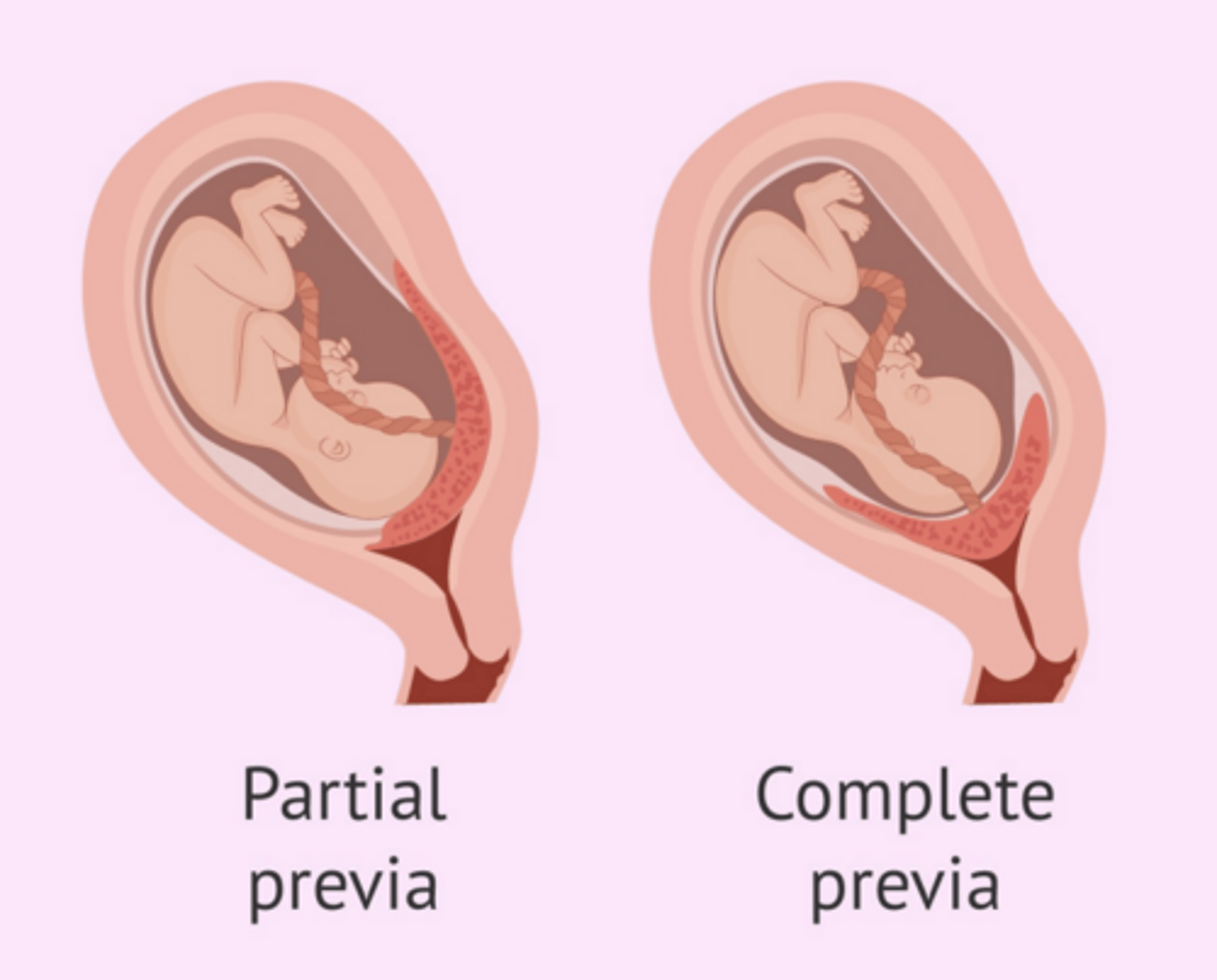
What is placenta previa?
Placental location close to or over the internal cervical os
What are the risk factors of placenta previa?
prior c-section/uterine surgery, multiple gestation, prior hx, advanced maternal age, and smoking
What is the difference between a partial and complete placenta previa?
partial overalies only part of the os whereas a complete covers the whole os
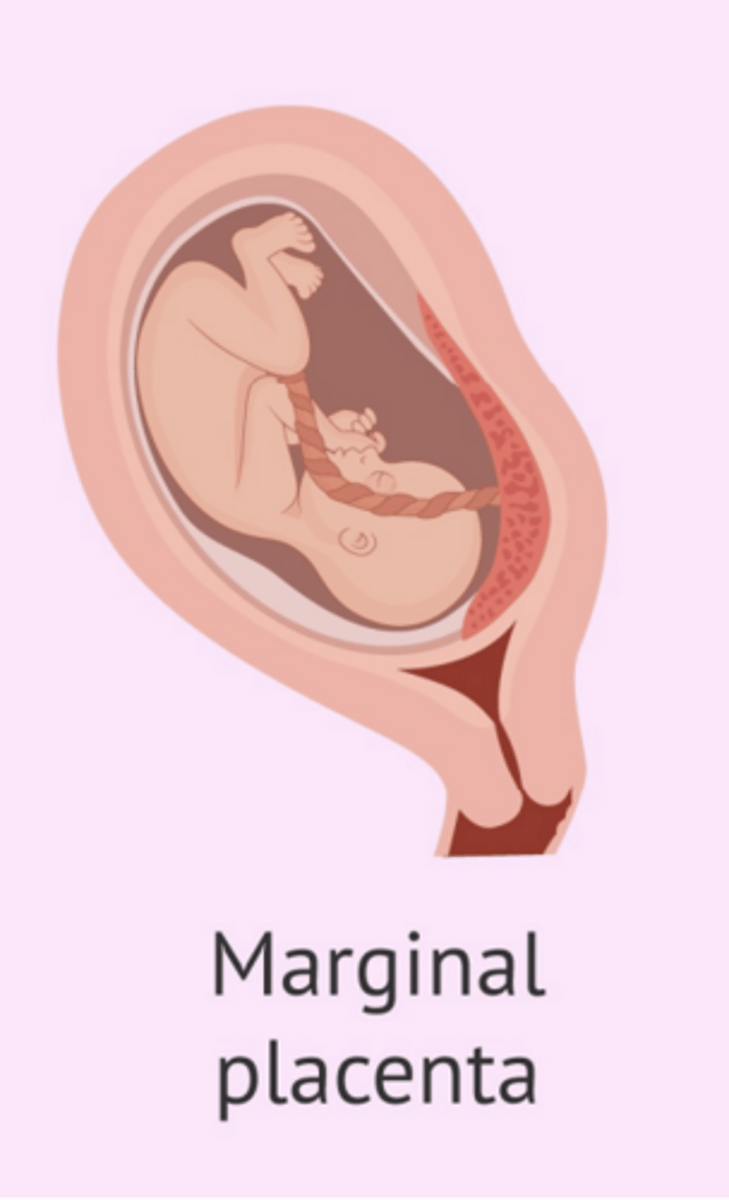
What is a marginal placenta previa?
Placenta edge within 2cm of the internal os without covering it
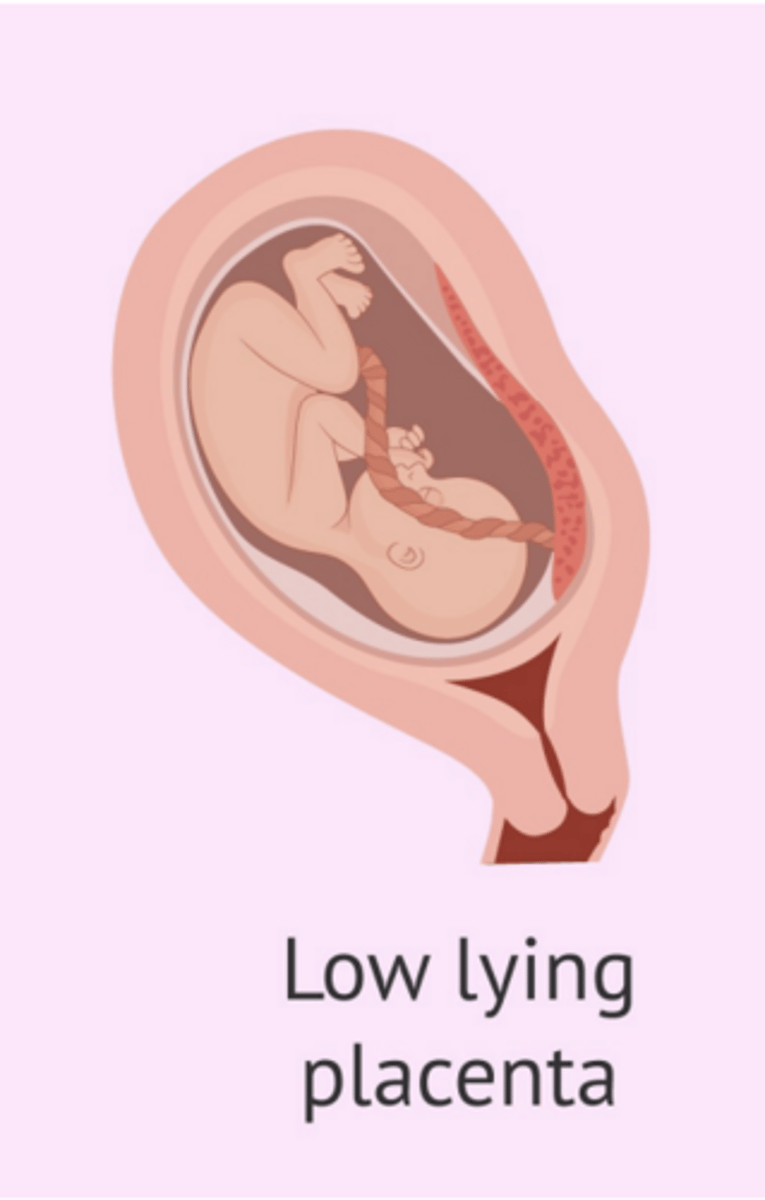
What is a low-lying placenta?
Placenta edge extends into lower uterine segment but is more than 2cm from the cervical os
What are the symptoms of placenta previa?
Painless vaginal bleeding after 20 weeks gestation (usually 29-30)
How is placenta previa diagnosed?
Transvaginal ultrasound
What is the treatment for asymptomatic placenta previa?
Avoid intercourse and decrease physical activity
What is the treatment for symptomatic placenta previa?
Admit to labor and delivery for maternal and fetal monitoring; if bleeding heavily, deliver via c-section
What is placental abruption?
Abnormal premature separation of a placenta after 20 weeks gestation; MC cause of coagulopathy in pregnancy
What are the types of placental abruption?
partial, complete, and marginal
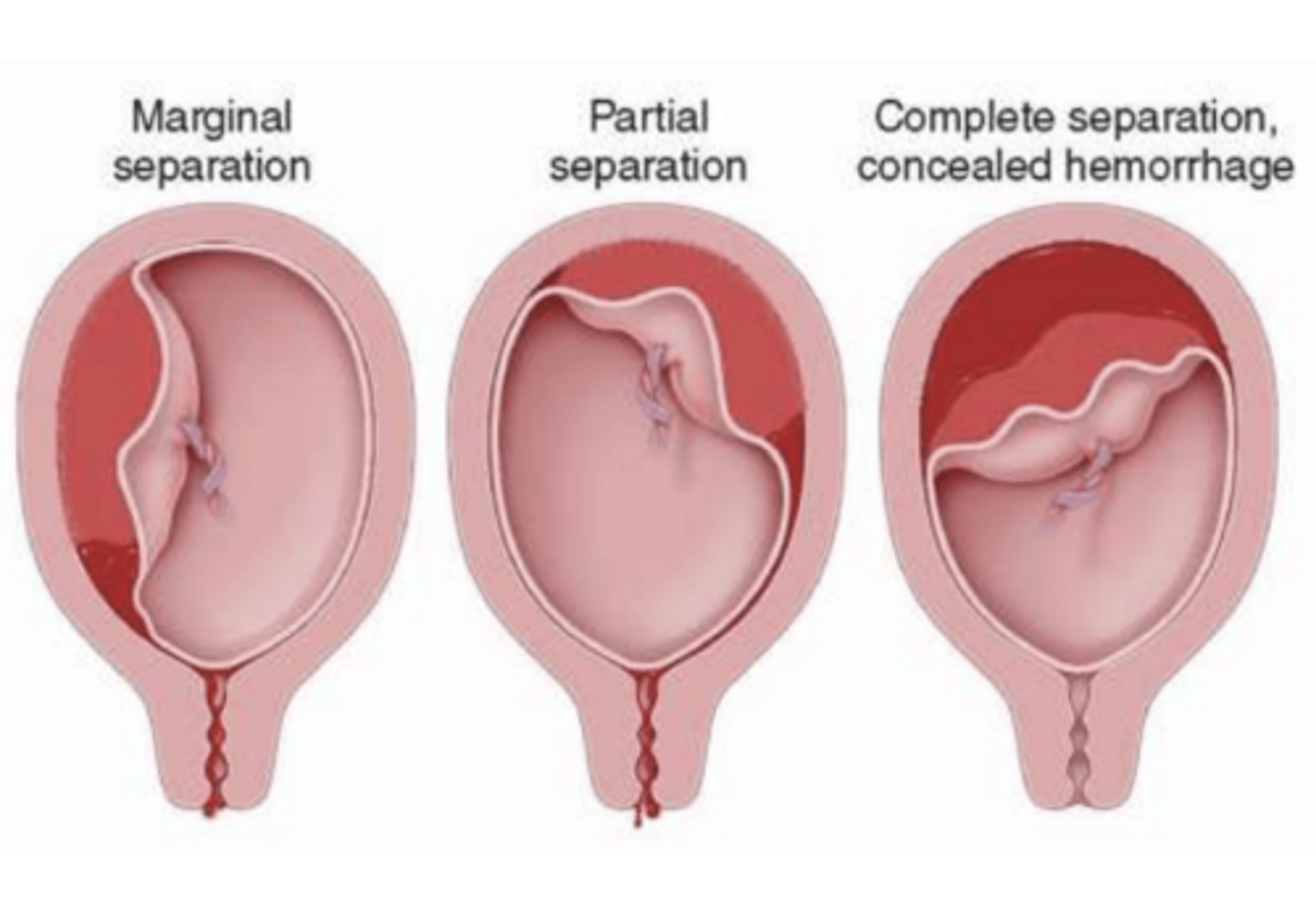
What causes placental abruption?
Rupture of maternal vessels accumulating blood in the decidua basalis causing separation of the placenta and further bleeding
What are the risk factors of placental abruption?
previous abruption, chronic HTN, preeclampsia, multiple gestation, advance maternal age, multiparity, smoking, cocaine, chorioamnionitis
What are the symptoms of placental abruption?
Painful vaginal bleeding after 20 weeks gestation, abdominal/low back pain, uterine tenderness, contractions, fetal HR abnormalities
What may appear on ultrasound in placental abruption?
retroplacental hematoma
What is management for placental abruption?
monitor hemodynamics, continuous fetal monitoring, c-section for unstable mothers
What is vasa previa?
Presence of fetal blood vessels over the internal os below the presenting parts of the fetus
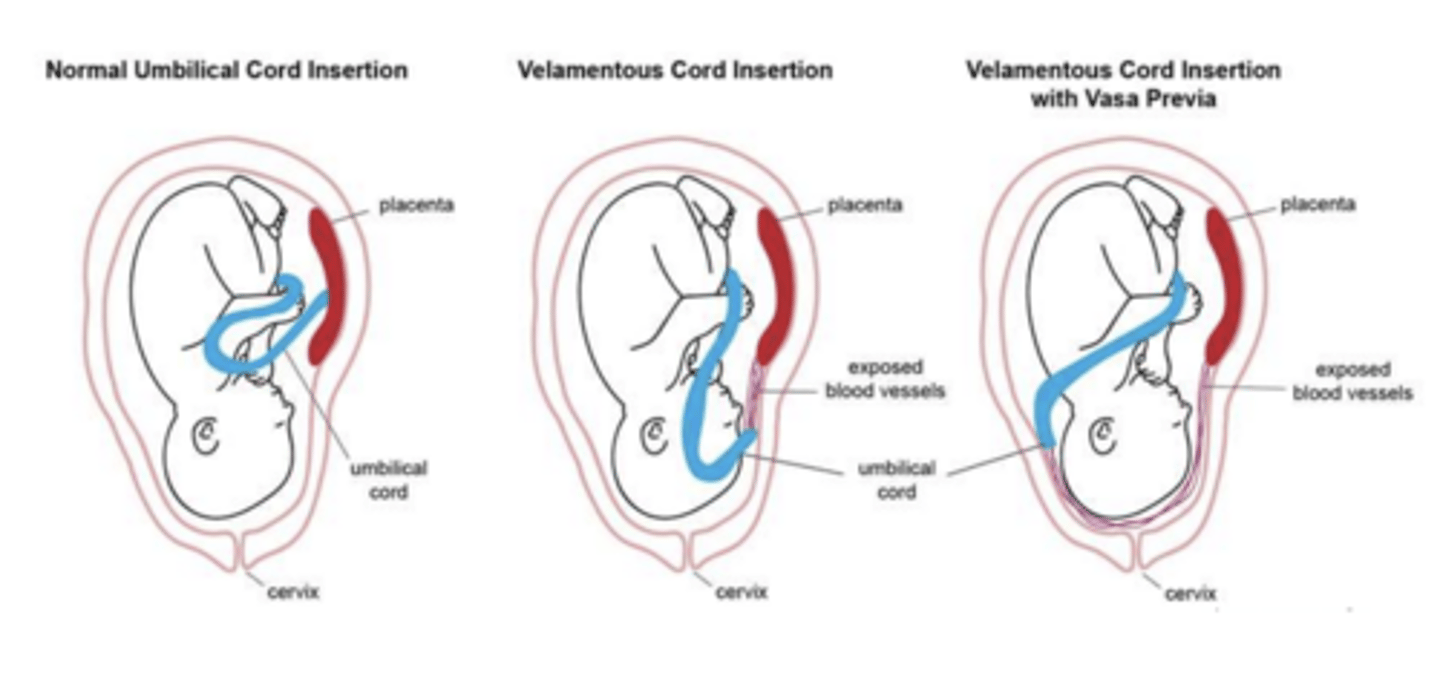
What is a complication of vasa previa?
Risk of rupture of fetal vessel
How is vasa previa diagnosed?
Transvaginal US with color doppler
What is the treatment of vasa previa?
C-section
What is placental insufficiency?
Inadequate placental blood flow resulting in reduced delivery of oxygen and nutrients to the fetus
What are the causes of placental insufficiency?
HTN, DM, placental abnormalities, smoking, autoimmunity
What are the complications of placental insufficiency?
fetal growth restriction, oligohydramnios, chronic fetal hypoxia, decrease FHS, stillbirth
What is fetal growth restriction (or intrauterine growth restriction)?
Fetal weight or abdominal circumference is < 10th percentile
What are the maternal factors of FGR?
chronic disease, substance use, multiple gestations, teratogens, infections
What are the fetal factors of FGR?
female fetus, chromosomal abnormality, congenital cardiac disease, multifetal pregnancy
What are the placental factors of FGR?
Placental abnormalities and Trophoblast invasion
What are the infant complications of FGR?
intrauterine death, avidemia, asphyxia, intolerance to labor
What are the neonate complications of FGR?
low apgar, hyperbilirubinemia, hypoglycemia, apnea, respiratory distress, seizure, neonatal death
What measurements are used to diagnose FGR?
- Biparietal diameter
- Head circumference
- Abdominal circumference
- Femur length
What is the management of FGR?
serial evaluation of fetal biometry q3-4 weeks with nonstress test, biophysical profile, and doppler studies
What are the risk factors for breech presentation?
preterm gestation, prior breech, polyhydramnios, hydrocephaly, placenta previa, multiparity, uterine anomalies and tumors
What is a frank breech position?
most common type with hips flexed, knees extended, and feet adjacent to head

What is a complete breech position?
both hips and knees are flexed
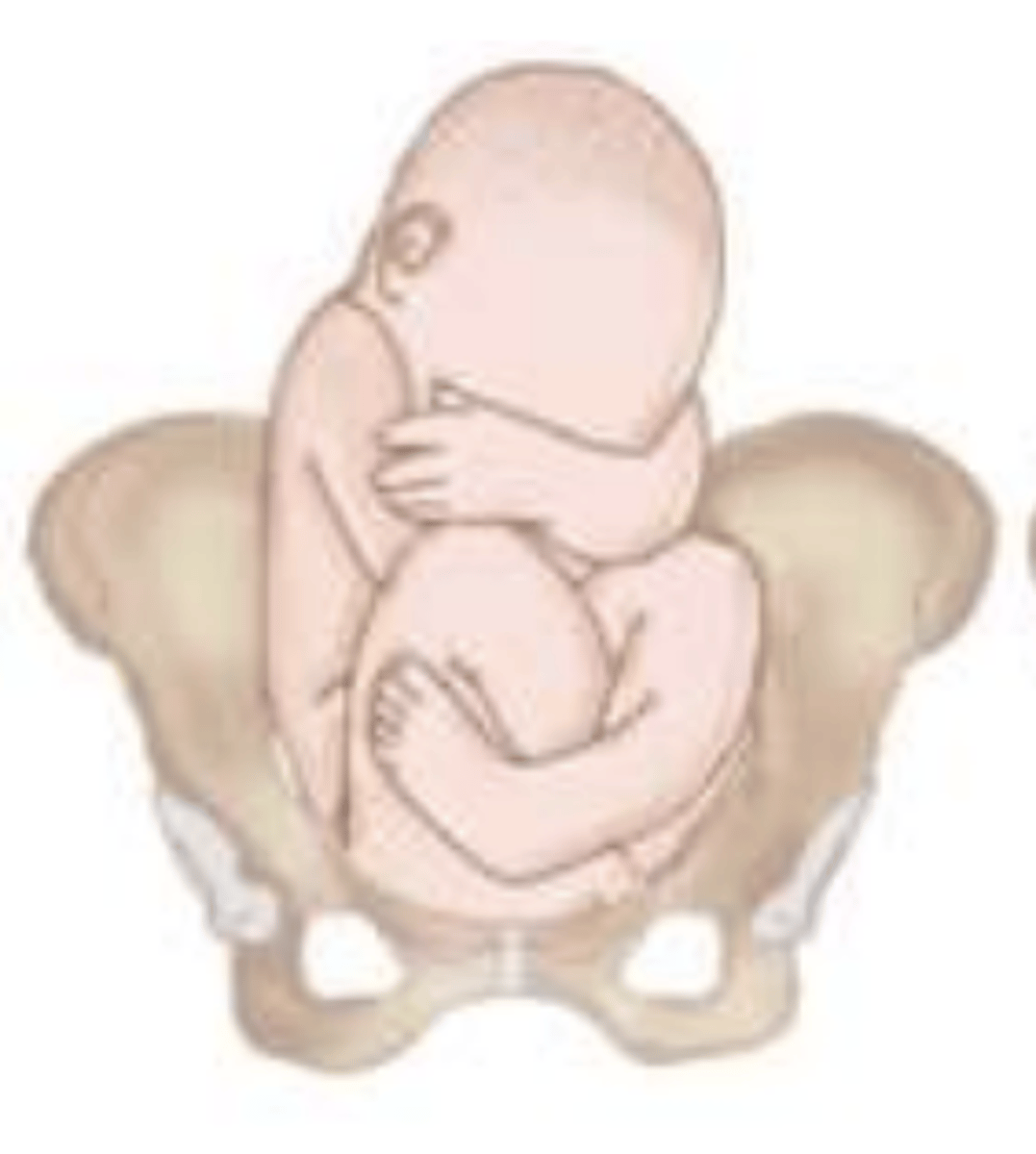
What is a incomplete breech position (footling)?
1 or both hips not completely flexed, presenting part maybe buttocks or one or both feet

How is breech presentation diagnosed?
leopold maneuvers, pelvic exam, and ultrasound
How is breech presentation treated?
External cephalic version (ECV) at 36-37 weeks gestation or cesarean delivery
What has caused an increased in multiple gestation births?
use assisted reproductive technology in the past decade
What are the other risk factors for multiple gestation births?
advanced maternal age, increasing parity, and family history
How do dizygotic (fraternal) twins form?
Occur when 2 separate ova are fertilized by 2 separate sperm; always dichorionic
How do monozygotic (identical) twins form?
Division of the fertilized ovum after conception; Chorionicity depends on timing of embryonic division
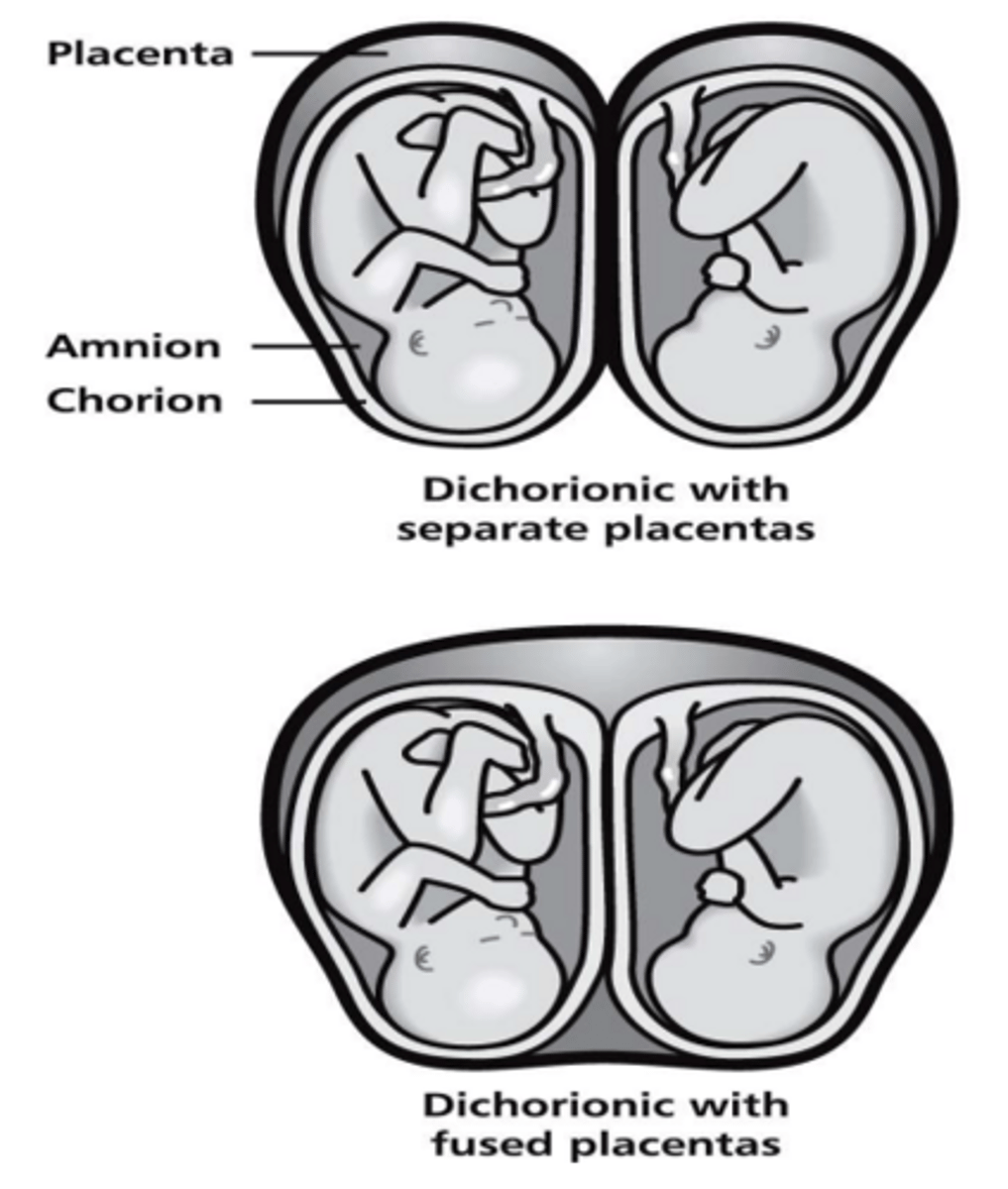
What is Diamniotic/Dichorionic?
2 placenta or 1 fused placenta/ 2 amnios/2 chorions
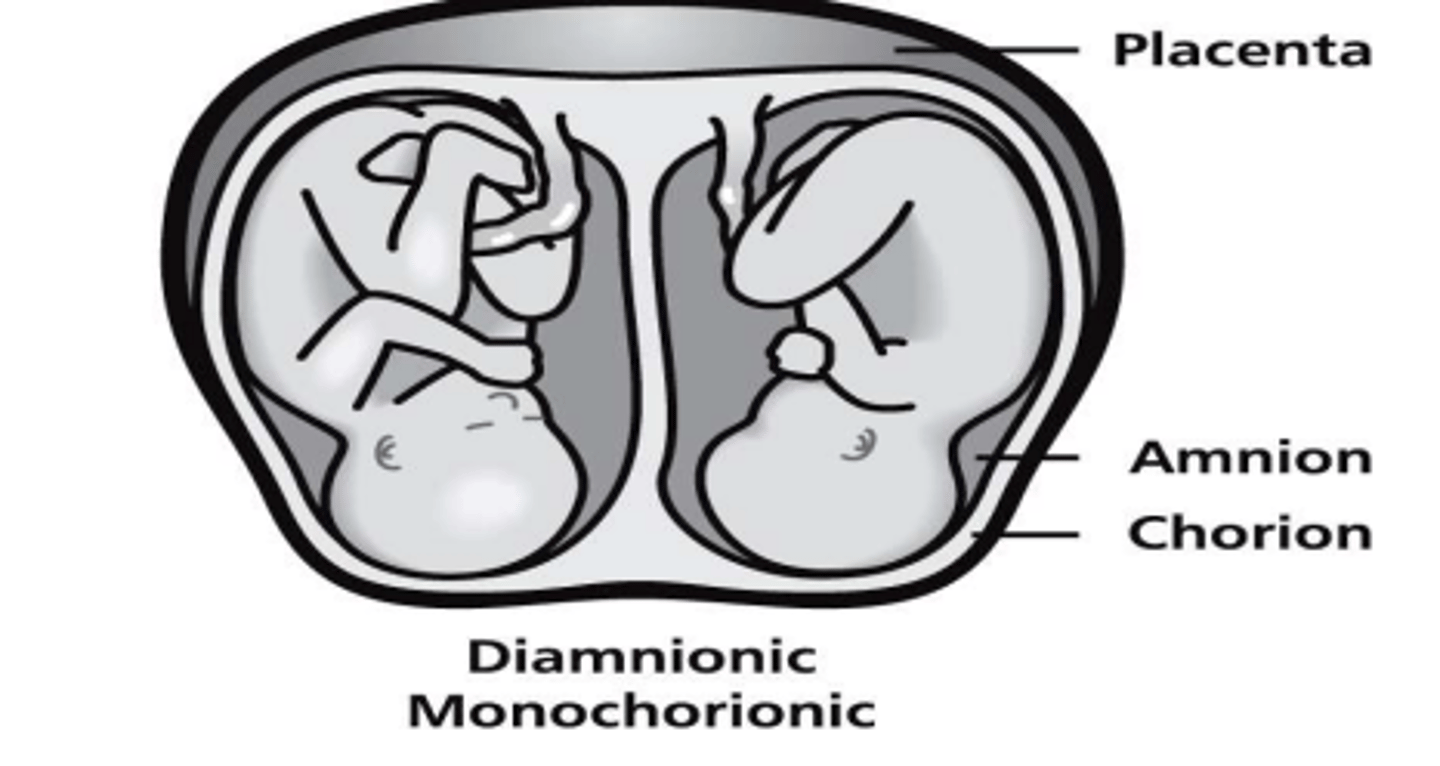
What is Diamniotic/Monochorionic?
1 placenta/ 2 amnios/ 1 chorion; concern for twin-twin transfusion syndrome (TTTS)
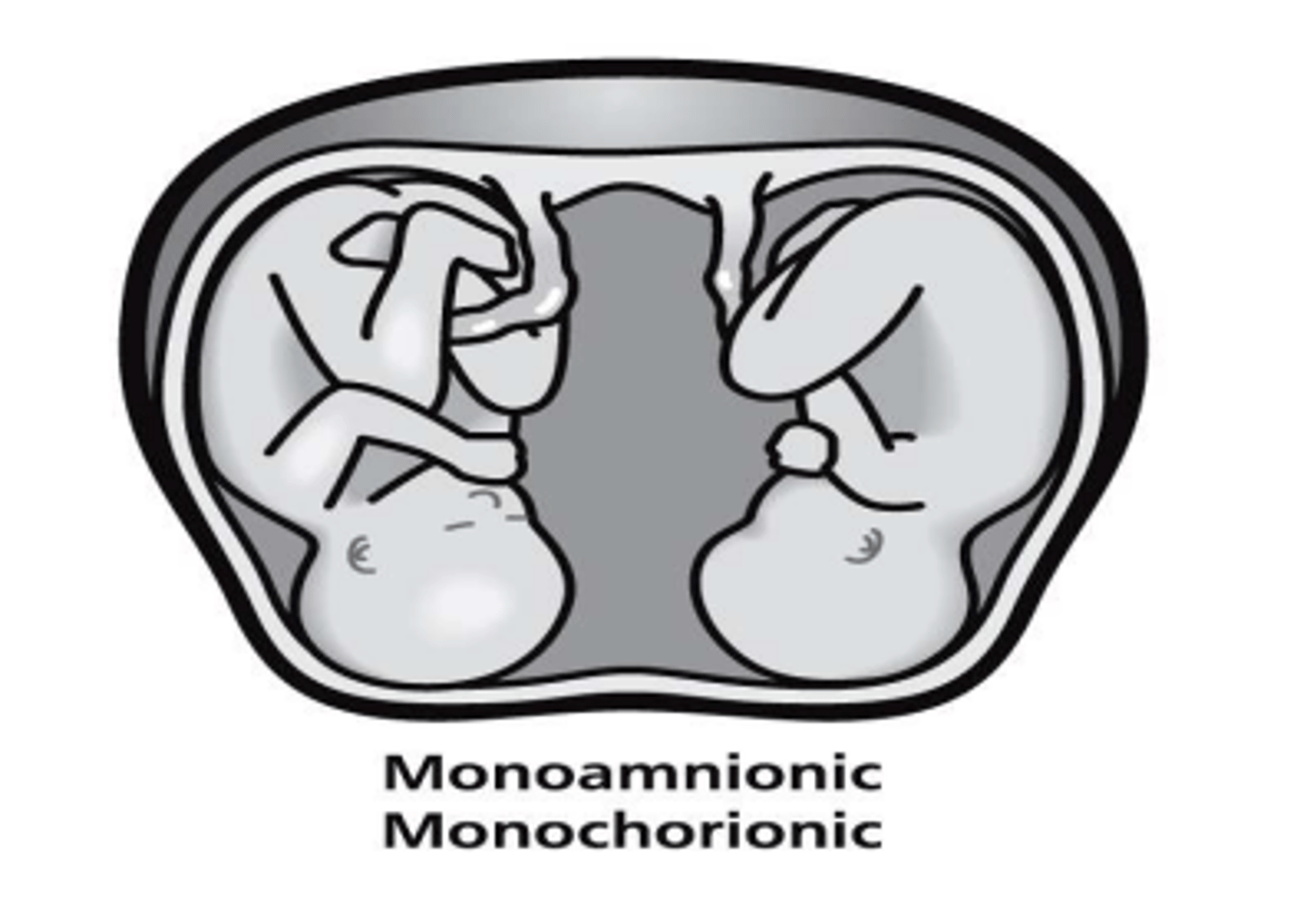
What is Monoamniotic/Monochorionic?
1 placenta/ 1 amnion/ 1 chorion; concern for cord entanglement
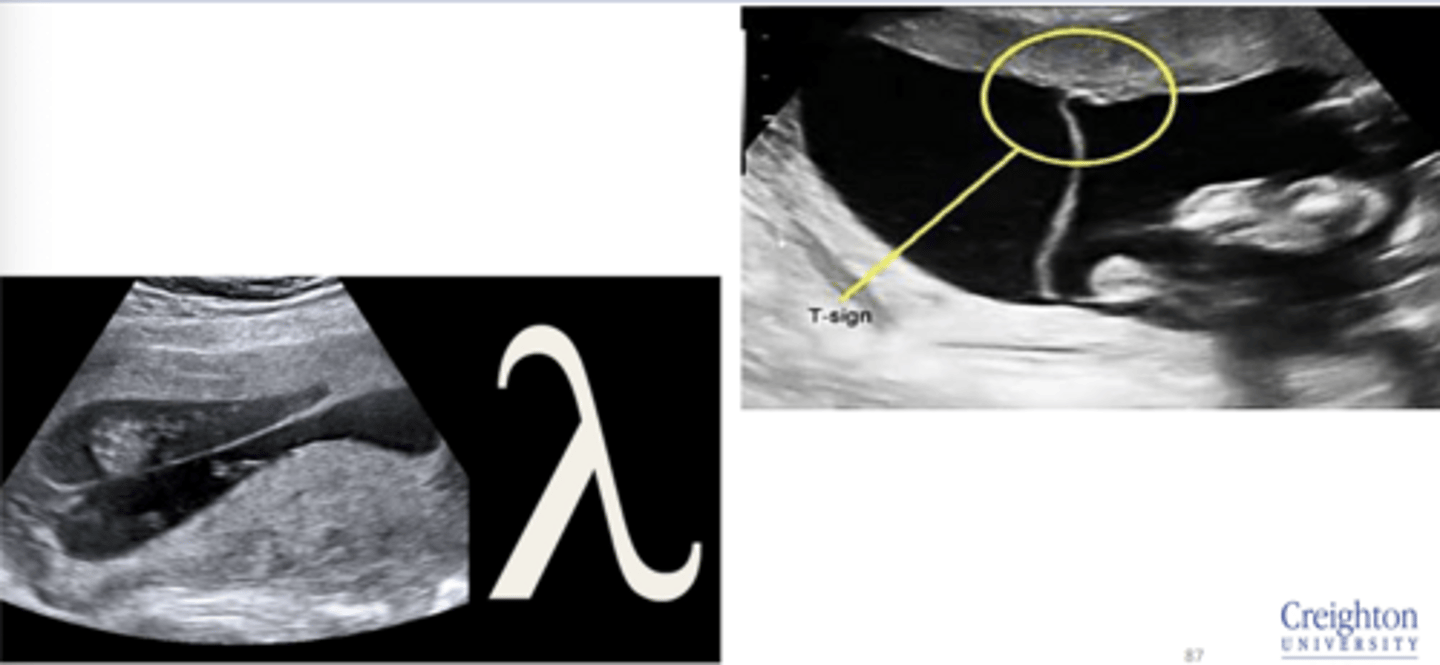
How does multiple gestation appear on ultrasound?
Dichorionic twins: Lambda sign
Monochorionic twins: T sign
What is the surveillance for Dichorionic twins?
Ultrasound for fetal growth every 4 weeks beginning around 24 weeks
What is the surveillance for Monochorionic twins?
Ultrasound every 2 weeks beginning at 16 weeks; Screen for TTTS
What is the delivery timing for multiple gestation pregnancies?
Di/DI ~38 weeks
Mo/Di ~36-37 weeks
Mo/Mo ~32-34 weeks (C section)
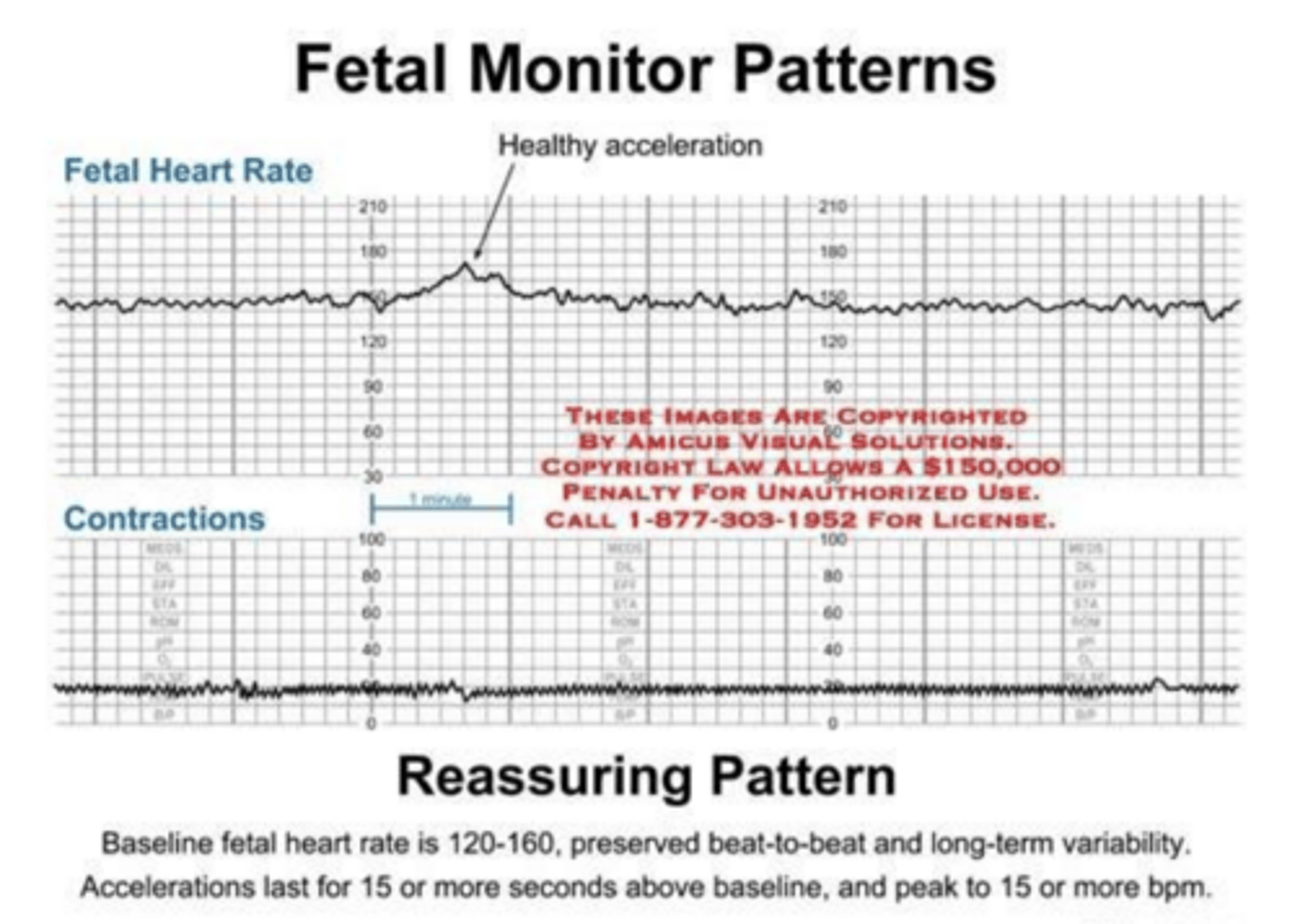
What are "reassuring" accelerations of fetal heart rate?
- 15 beats/min lasting 15 seconds or longer > 32w
- 10 beats/min lasting 15 seconds or longer < 32w
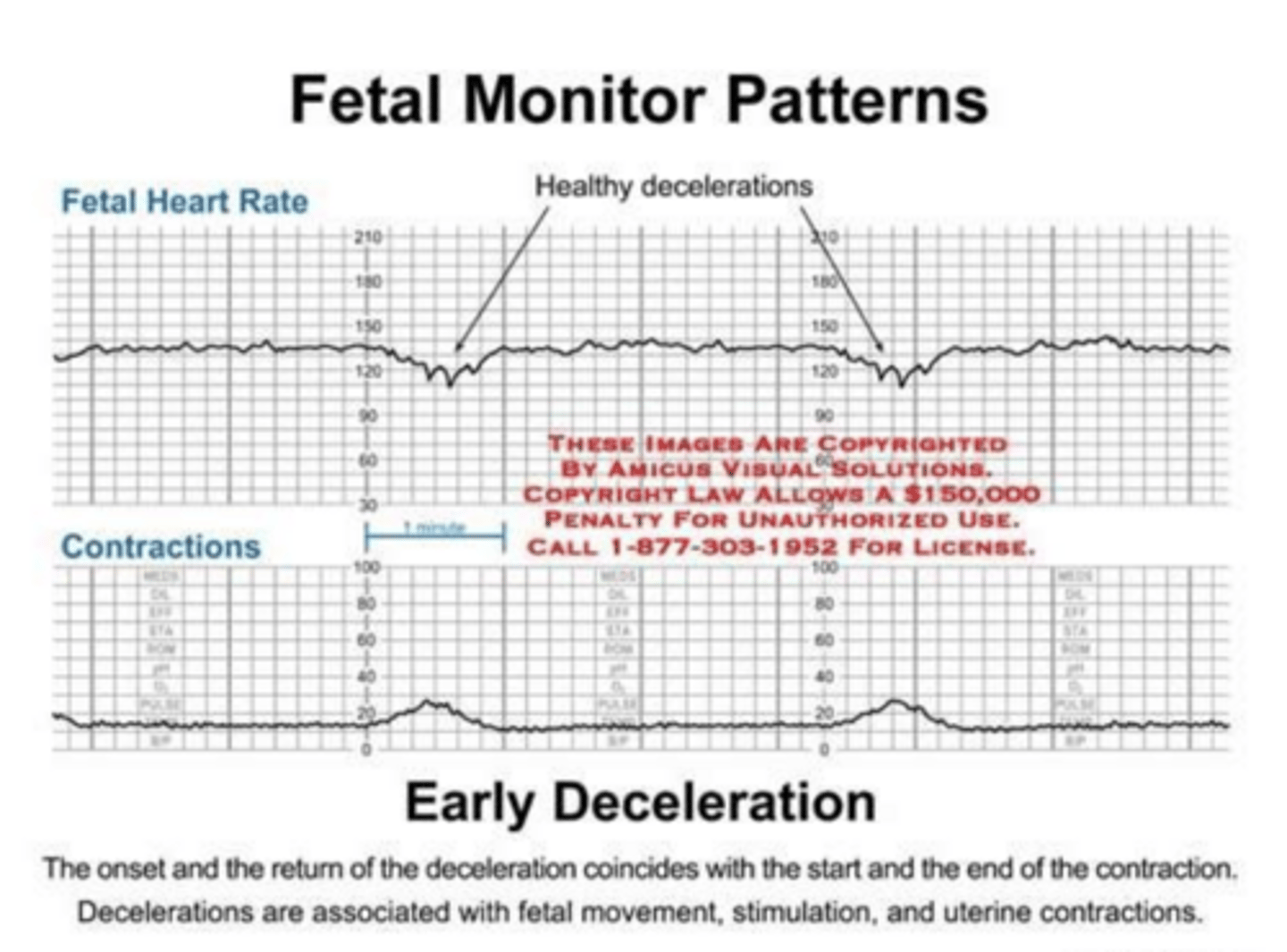
How does early deceleration appear on fetal heart monitoring?
Mirror contractions seen with head compression
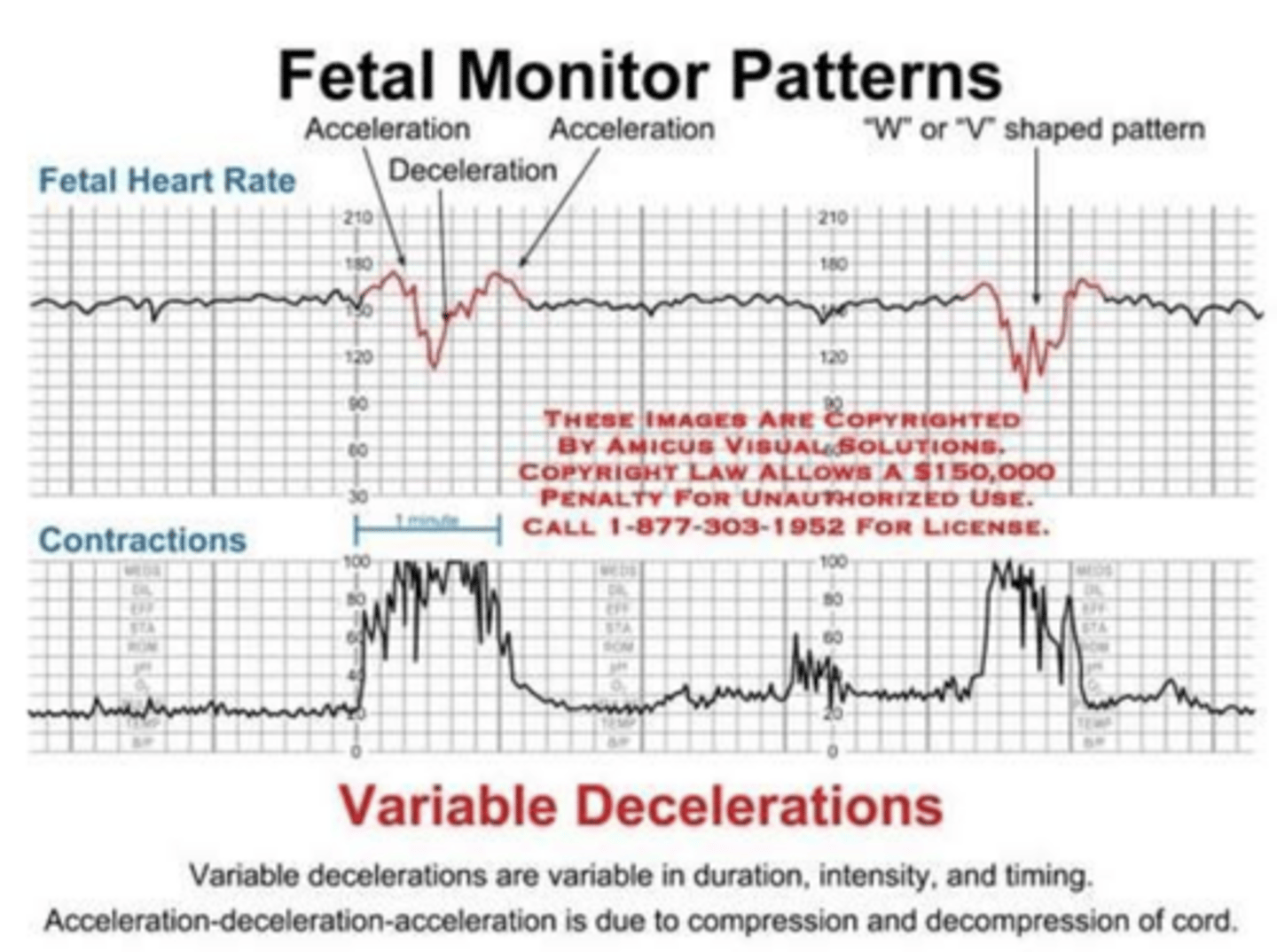
How does variable deceleration appear on fetal heart monitoring?
Irregular dips in fetal heart rate seen with temporary cord compression
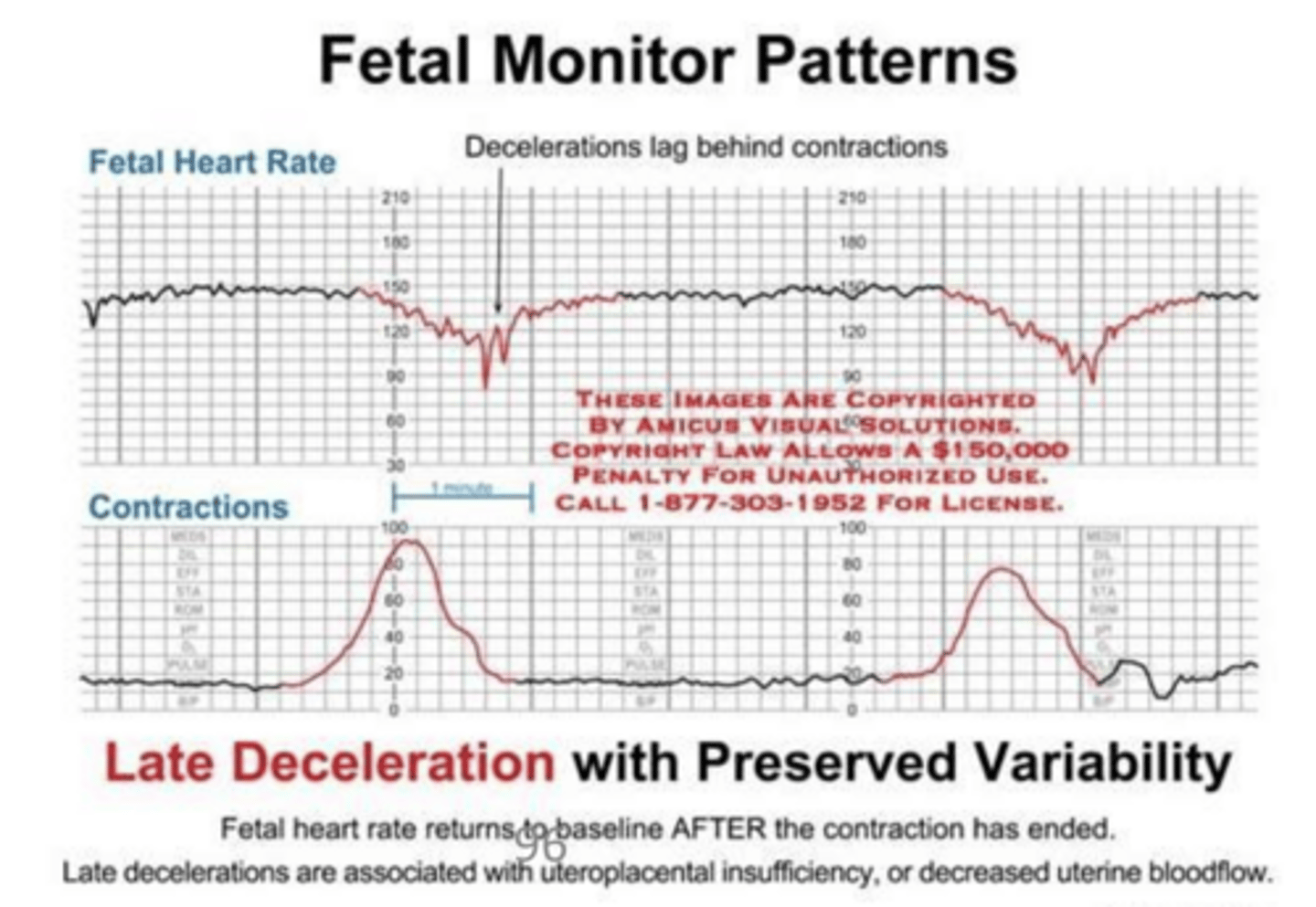
How does late deceleration appear on fetal heart monitoring?
Falls in heart rate after contraction has started seen with fetal hypoxia
What is uterine rupture?
Spontaneous complete transection of the uterus from the endometrium to the serosa
What is the primary complication of uterine rupture?
Fetal expulsion into abdomen with survival depending on if large portion of the placenta remaining attached to uterine wall
What is the treatment of uterine rupture?
Laparotomy with C-section delivery and hysterctomy if necessary
What are the types of "SCORTCH" infections?
Syphilis
CMV
Other infections (Zika)
Rubella
Toxoplasmosis
Chickenpox (varicella)
HSV