Duane's Syndrome
1/14
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
15 Terms
Characteristics
- CCDD
- Common LE – F, unilateral
- Sporadic – can be inherited
- Limited adduction/ abduction
- Globe retraction on adduction
- Palpebral fissure narrowing on adduction
- Widening on ab
- Up + down shoots = fibrotic LR or co innervation
- A/V patterns
- ↓ convergence
- Amblyopia
- AHP
A: Associated general conditions:
- Ocular: coloboma, hetechromia, microphthalmia
- Syndromes
Kippel-fiel: fused cervical vertebrae
Goldenhar: facial hypoplasia
Q: How is Duane's Syndrome classified?
UK System (based on clinical observation):
Type A: Abduction limitation > adduction
Type B: Limitation in abduction only
Type C: Adduction limitation > abduction
US System (based on electrical activity in muscles):
Type 1: Limitation of abduction
Type 2: Limitation of adduction
Type 3: Limitation of both abduction and adduction
Q: What is the current understanding of the aetiology of Duane's Syndrome?
- Myogenic/ mechanical
- Non elastic LR
- LR is fibrotic/ atrophic
- MRI: confirm absence of 6th CN
o Co- innervation abnormalities
(CCDD) due to hypoplasia or aplasia of the 6th cranial nerve (abducens nerve)
Misdirection of the 3rd nerve (oculomotor nerve) leads to co-contraction of the medial rectus (MR) and LR, causing characteristic eye movement abnormalities
MRI studies confirm hypoplasia of the abducens nerve and abnormal innervation by the 3rd nerve
A: Main eye signs in Duane's Syndrome:
Limitations: Fibrosis or atrophy of the LR along with co-contraction
Retraction: Co-contraction of MR and LR
Palpebral fissure changes: Narrowing due to retraction
Upshoots/Downshoots: Slippage of the LR due to fibrosis
A: Investigation of Duane's Syndrome includes:
History: Look for congenital history, AHP (abnormal head posture), and other eye signs
Visual Acuity (VA): Check for amblyopia- Cover Test (CT)/AHP: Relation to types A, B, or C. Esophoria controlled by face turn in type A/B; exophoria in type C
Ocular Motility (OM): Assess for eye movement limitations
measure duction, observe globe retraction + fissure changes
Convergence: Usually reduced, especially in type C
Hess Chart: squashed field
FOB: indicate extent of dip
Q: What are the non-surgical management options for Duane's Syndrome?
- Correct RE
- Tx amblyopia
- CI exercise
- Prism trial – sm angle
- BT
A: Indications for surgery in Duane's Syndrome:
Decompensation, significant AHP, or large non-functional deviations
Botox trial (BT) can be used to assess if surgery is necessary
Q: How is Duane's Syndrome surgically managed?
- Type A/B eso – esp
o MR recession
o Avoid LR resection
o Faden suture for AHP
o LR burification or recession – up + down shoot
Jensen improve ABduction – SR & IR to LR
§ Use fells modification
- Type C – exo
o LR recession
o Vertical rectus transposition – improve ADD
- Retraction of globe
o Faden or LR recession +/ burification
What are the key investigative tests that you would like to do at this orthoptic visit and likely findings? - Mum has indicated that she is keen for her 7-year-old son who has a left DRS type A to have surgery to help with the realignment of his eyes.
VA – amblyopia if manifest)
CT/AHP – AHP if present will be a FT to - left to move eyes away from abduction. The size of the AHP - if this is large, surgery may be needed to aid the head to be straightened.
W AHP patient control the deviation to esophoria - check recovery and size of deviation as may indicated surgery is required to reduce the angle.
Without the AHP - pt = esotropia & deviation - incomitant & larger fixing with the left eye. check if the pt notices diplopia with the head straight.
OM’s – ask the patient about diplopia in each position of gaze to establish how much of a problem this is in real life. There will be limitation of the left eye of abduction and adduction, the limitation of ab>add.
Palpebral fissure changes – narrowing on adduction and widening on abduction.
Retraction of the globe on adduction.
Up/Downshoots of the affected eye may be evident on adduction.
A and V patterns may be present.
Convergence may be reduced but more common in type C.
Assess the PFR with the AHP to assess control of the deviation, could also do CBA.
Measure stereopsis with the AHP.
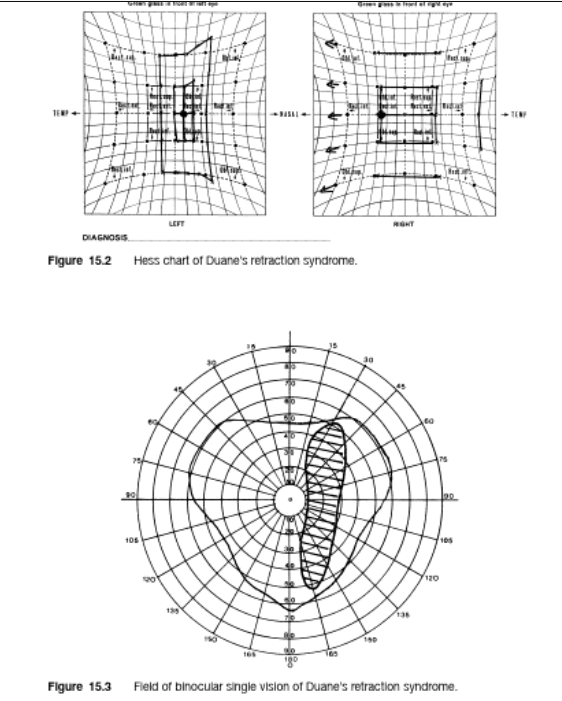
Field of BSV to indicate the extent of diplopia in real life, diplopia will be present on the left especially but also possible to the right due to the limitation of both abduction and adduction.
Hess Chart will show squashed field in the affected eye in the horizontal positions with overactions in the right eye.
PCT in pp and on lateral gaze (5 positions if A/V). This will demonstrate the extent of the incomitance and be useful in planning sx.

PP shows narrowing of the palp fissure in the LE (could be due to microphthalmos or some retraction of the globe).
L gaze indicates approx. -4 restriction of L abduction.
R gaze indicates approx. -2 restriction of L adduction (appears worse on laevo elev/dep). Also on R gaze there is a small downshoot of the LE on adduction.
Narrowing of the L palp fissure on R gaze (with possible associated retraction of the globe) and widening of the L palp fissure on L gaze.
No A/V pattern evident.
Limitations are caused by fibrosis/atrophy LR (absence of innervation)/co-contraction of MR and LR.
Retraction is caused by co-contraction, fibrosis LR.
Fissure changes, narrowing is caused by retraction of the globe and widening caused by extra-innervation.
· The downshoot may be caused by slippage of the fibrotic LR or abnormal co-innervation of the vertical muscles on adduction.
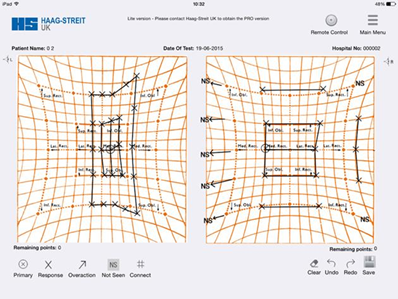
Hess chart
LE is the affected eye with a squashed field in opposing directions (horizontally).
Deviation in the pp is 5 degrees FR and 15 degrees FL.
Restriction of L abduction and L adduction Ab>Add.
O/a of RMR and RLR.
Small o/a of LSO and IO which may be related to upshoots/downshoots.
The Hess Chart is consistent with a DRS type A
surgical options
Large deviation (non-functional): left MR recession(s) AVOID LR RESECTION
To reduce retraction: left LR recession (plus MR recession/s)
To reduce large AHP: Faden and recession of right MR or bilat MR recessions
To reduce the downshoot: Faden to left LR or recession of LR with bifurcation
To increase the abduction of the left eye: vertical transposition of the left SR and IR to the LR, can combine with L MR recession but risk of ASI. Alternative could use Jensen’s (explain procedure)
INV
CH
abnormal eye movements/ AHP/ DEV- children
adults - decompensation - can be dip
VA
amblyopia if manifest strab or aniso
AHP
FT to affected side
CT
c & s AHP
typically - convergent dev
a typical - divergent dev
OM
limited abduction & limited adduction
retraction of globe on adduction
narrowing of palpebral fissure on attempted abduction
upshoots/ downshoots of affected eye on abduction
slippage of LR
A or V patterns
Convergence
poor if limited adduction
BV
good c AHP
AOD
differ
Hess
Field of BSV
area of bsv positioned away from position of max limitation
DD
DD
6th nerve palsy
medial wall fracture
localised inflammation
moeibus syndrome
iatrogenic cause
associated eye signs
lens opacities
heterochromia
iridies
fundal defect
microopthalmos
crocodile tears