Autism
1/12
Earn XP
Description and Tags
EDEXCEL A-LEVEL PSYCHOLOGY
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
13 Terms
Autism
A developmental disorder that affects communication, behavior and social interaction. It is a spectrum disorder so symptoms and abilities vary widely between individuals.
Features of Autism (DSM-5)
Social Communication Difficulties - verbal communication and social interaction
Restricted and repetitive behaviors - speech, strict routines and intense interests
Early Onset - Appear in early childhood but may be more noticeable as social demands increase
SOCIAL COMMUNICATION DIFFICULTIES: (Theory of Mind)
Conversational reciprocity deficits
Nonverbal communication deficits
Lack of humour
Difficulty understanding social cues and forming or maintaining relationships
Preference for solitude
Problems organising tasks (executive dysfunction theory)
RESTRICTED & REPETITIVE BEHAVIORS:
Repetitive movements
Strict Routines
Intense Interests
Hypersensitivity
Hyposensitivity
Strengths of Autism
Strong Memory Skills: Excellent LTM
Attention to detail (weak central coherence theory - Frith (1989) - inability to see the bigger picture)
Logical reasoning and problem-solving skills
Support:
Clear communication
personalised learning
routines
Treatments for Autism
Applied Behavior Analysis (ABA) - builds social skills
Speech & Occupational Therapy - speech development, motor skills and daily tasks
Medication - prescribed for associated symptoms like ADHD or anxiety
CBT - Focuses on repetition and social cues. Researchers found this reduced anxiety and helped autistic children regulate their emotions, but this requires the child to speak.
Evaluation of Autism Diagnosis
STRENGTHS:
Frazier et al. (2012) - DSM-5 was valid and reliable in reflecting symptoms for an effective treatment plan and factor analysis was used.
WEAKNESSES:
Taylor et al. (2007) - 27 clinicians used DSM-5 criteria to classify symptoms in 9 video clips but this was only reliable 3/9 of the time.
Frith (2003) - too much focus on deficits - ASD individuals have poor global processing but skilled local cognitive processing.
Biological Explanation of Autism - Amygdala
Nordahl et al. (2012) investigated children with ASD:
6-9% had a larger amygdala than average at 2 years of age
Amygdala growth stalls over time, causing impairment
Social Brain Hypothesis (Brothers, 1990): Amygdala is linked with the PFC in regulating motivation, emotional responses and social behavior.
Baron-Cohen et al. (1999) - ASD children struggle to read facial expressions from eyes as fMRI scans showed under activity in the left amygdala.
Gallagher & Frith (2003) - reviewed studies using fMRI scans to identify brain areas linked to ToM and found anterior paracingulate cortex and superior temporal sulcus to be mainly involved, so this may be impaired for children with ASD. Cheng et al. (2015) found STS functions differ in ASD ppl.
Evaluation Of The Biological Explanation Of Autism
STRENGTHS:
Kennedy et al. (2009) case study of SM - FEARLESS WOMAN
Genetic disorder in amygdala - her comfortable distance with the female experimenter was much closer than 20 controls, showing the effect on social deficits
Application to drug-based treatment → ASD linked to amygdala dysfunction can lead to an earlier diagnosis
WEAKNESSES:
Inconsistent findings - Herbert et al. (2003): Smaller amygdala volumes was found in ASD children than controls, conflicting with previous studies
Indirect link - White et al. (2009) - link between amygdala dysfunction and social deficits may be caused by impaired anxiety processing
Oversimplification - Other brain structures besides the amygdala may also be involved in social and behavioral challenges. Paul et al. (2010) found that 2 women who had lesions on their left and right amygdala had some social deficits but not to the extent of ASD.
Gender Differences - Halladay et al. (2015) found males are less responsive to social cues and females may be better in disguising symptoms. Schumann et al. (2009) found ASD children show larger amygdala volumes, with females having more significant differences.
‘Theory of Mind’: Non-biological explanation of autism
ToM: Our awareness that others have separate thoughts and emotions. A key development in social cognition for empathy and social interactions.
Baron-Cohen (1995): MINDBLINDNESS. Impairments linked to developmental disorders like ASD.
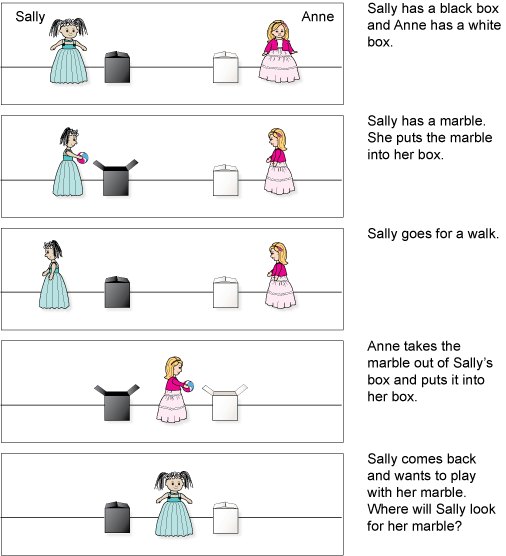
Wimmer & Perner (1983): Sally-Anne Test (False-Belief Tasks)
Baron-Cohen et al. (1985):
Neurotypical: 85%
Down Syndrome: 86%
ASD: 20%
Leslie (1987) - the capacity to pretend and understand the presence of others.
Joint attention - showing an appreciation for internal mental states. Scraife & Bruner (1975) - Neurotypical children show this in 14 months.
Development:
Understanding desires (18 months to 2 years)
Understand beliefs but not false beliefs (3 years)
Understand false-belief tasks (4-5 years)
Deception, sarcasm & complex beliefs (6-7 years)
Evaluation of ‘Theory of Mind’: Non-biological explanation of autism
STRENGTHS:
Baron-Cohen et al. (2001) - adults with ASD performed worse than controls on an ‘eyes test’, supporting the impaired ToM (unable to infer emotional states from facial expressions).
Kasari et al. (2012) studied children with ASD in a programme to improve joint attention skills and found significant language improvement. Can be applied to useful interventions like mindreading and the use of social stories to teach ASD children social situations.
WEAKNESSES:
ToM is a limited theory and cannot explain all symptoms of ASD: Frith & Happé (1994) found some people with ASD pass the eyes test and ‘Sally-Anne test’. Overemphasis on false-belief tasks and ToM is slightly earlier in boys.
Causes of ASD could be genetic or neurobiological impairment.
Autism Therapy: Picture Exchange Communication System (PECS)
Bondy & Frost (1985) - PECS is a visual communication system that uses pictures to help individuals with ASD express needs and ideas. Main aim is to develop functional communication based on applied behavioural analysis. PECS helps children with ASD make the first move in communication spontaneously rather than just responding.
Process of PECS:
Child selects picture card
Hands it to communication partner
Partner provides requested item
Pre-program preparation: find out which objects and activities the child is interested in. Exchange and association is taught.
STAGES:
Physical exchange - adult helps the child hand the card. Positive reinforcement.
Increasing independence - Physical distance between child and teacher is increased. Child learns to travel to the book to exchange picture for what they want.
Learning to discriminate - Child has to choose from a range of object pictures in the book to express what they want.
Building complex sentences
Spontaneously answering direct questions using sentence strip.
Child expands their vocabulary to expand sentences.
Meta-analysis by Ganz et al. (2012):
PECS is more effective with younger participants
Children benefit the most when finishing all stages
Evaluation Of Autism Therapy: Picture Exchange Communication System (PECS)
STRENGTHS:
Charlop-Christy et al. (2002) - PECS is easy and quick to use. Joint attention improved significantly and a reduction in problem behaviours.
Investment in PECS would lower costs to wider society of social care.
WEAKNESSES:
Flippin et al. (2010) - small gains in spontaneous speech so there is limited support
Only focuses on functional communication requests so there are negative effects on speech development
Baron-Cohen (2009) - therapies should focus on child’s intrinsic rewards.
Autism Therapy: Early Intensive Behavioural Intervention (EIBI)
Early Start - greatest success under 2 years
Intensive - Highly structured (20-50 hours a week)
Focused on positively reinforced behaviour - ABA
Elements:
Trained Behaviour therapist and supervised by a professional
Targets improvement in communication, social interaction and self care
practice learned skills in a new environment
Stages: Lovaas (2002)
Establish cooperation
Foundations skills
Socialisation & communication
Evaluation Of Autism Therapy: Early Intensive Behavioural Intervention (EIBI)
STRENGTHS:
Reichow et al. (2012) - 5 studies with a control group. Children with ASD who received EIBI had significant improvements in IQ and communication.
Dawson (2008) - EIBI can change brain development before the full ASD effects.
WEAKNESSES:
Healy & Lydon (2013) - Behaviorist techniques are outdated and unsupported by evidence.
Time intensive and costly
over-structured and not always child-led
Boucher (2009) - early intervention is successful in any therapy
Reductionist - over-emphasis on behaviorist view whilst other psychological and biological factors are ignored.