3.2 Pharmacological Treatments for Substance Use Disorders
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
ABCDE in addiction
Addiction is characterised by:
a)Inability to consistently Abstain;
b)Impairment in Behavioural control;
c)Craving; or increased “hunger” for drugs or rewarding experiences;
d)Diminished recognition of significant problems with one’s behaviour and interpersonal relationships; and
e)A dysfunctional Emotional response
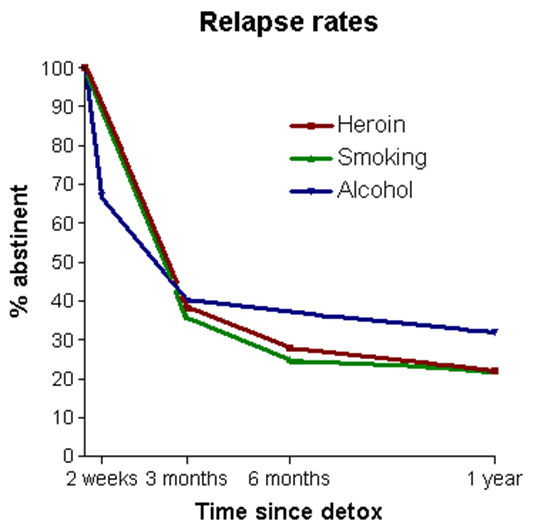
Relapse Rates -3 similar trends with the drug of..
Heroin, smoking, alcohol
•Relapse rates post treatment &/or withdrawal
•
•Similar curves for different drugs
•
•Implies common underlying mechanism(s)
Chronic Disease Model* idk what this slide is really talking about
•Asthma, Hypertension, Type 2 Diabetes, Schizophrenia
•Genetic predisposition (twin studies)
•Lack of definitive cure
•Similar results from treatment, ie 30-50% abstinence at 1 year
•Adherence (or concordance) lowest in lowest socio-economic groups / Dual Diagnosis / lack of supports
•Motivation / Control plays a major role in dependence
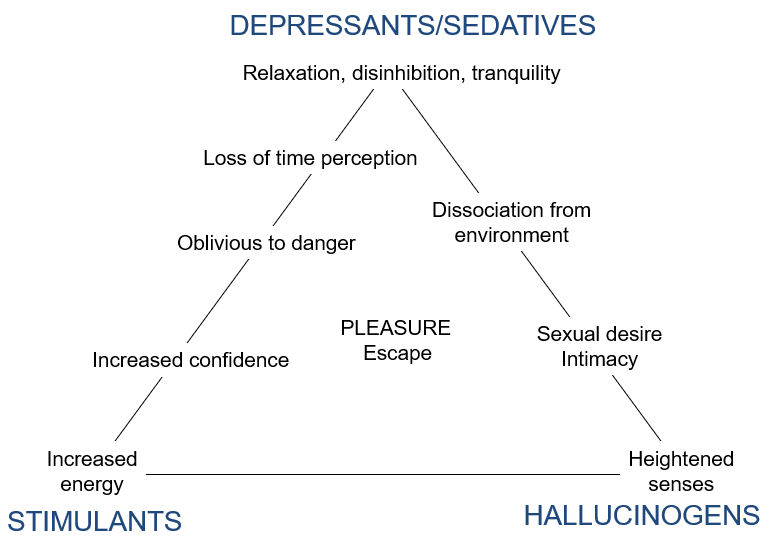
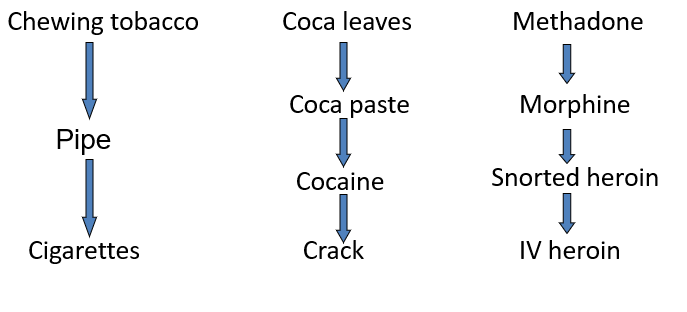
Triangle of drugs / effects
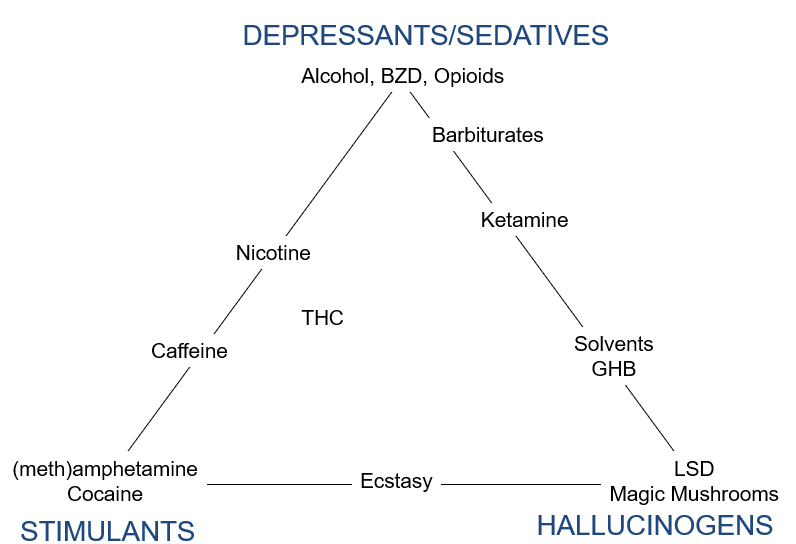
Triangle of drugs / effects, example of drugs
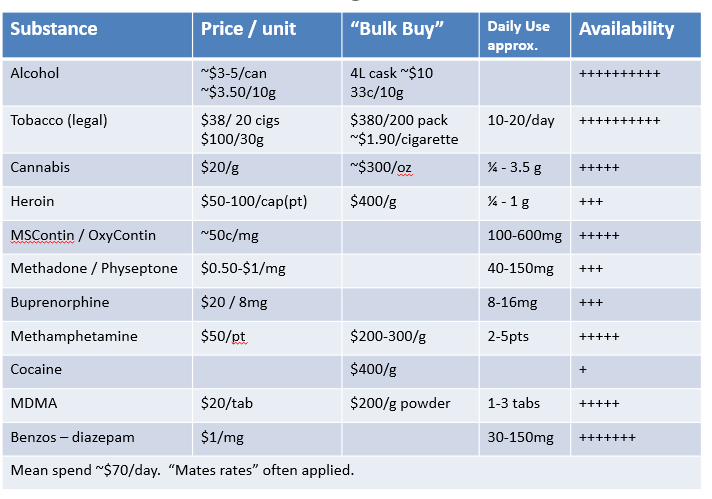
Market Forces, Queensland 2025 (inc. IDRS) * surely dont have to memorise this
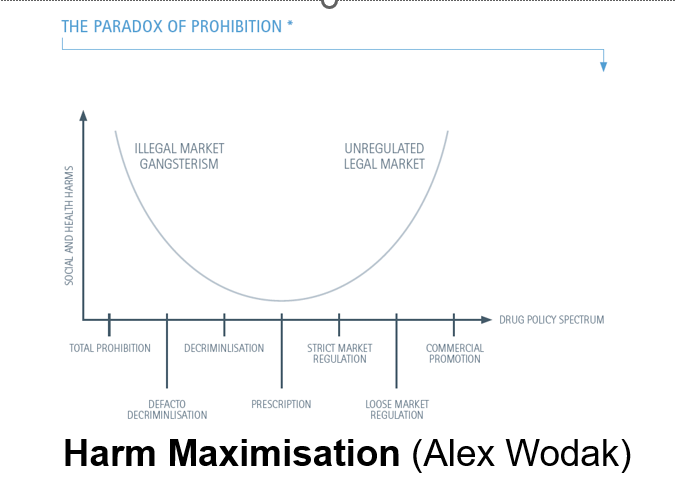
The war on drugs *
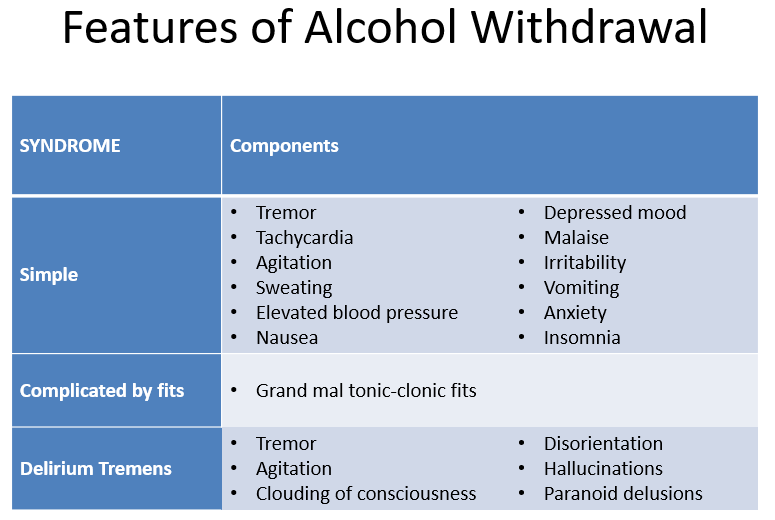
Withdrawal states *
•Drug decrease/absence > CNS rebound
•Reflects dependence / SUD
•
•Characteristic for each category of drug
•
•≈ Opposite of drug effect
•Withdrawal Syndrome
–withdrawal symptoms occur on cessation or reduction in use
–symptoms are generally opposite to acute effects of the substance
•i.e. for CNS depressants: tremor, sweating, anxiety, agitation, depression, malaise, nausea, dizziness, headache
–relief of withdrawal symptoms by further drinking or drug use
Pharmacokinetics
“the rush”
•Faster onset of drug effect = “better rush”
Faster onset related to speed of reaching the brain
crossing the blood-brain barrier
lipophylic
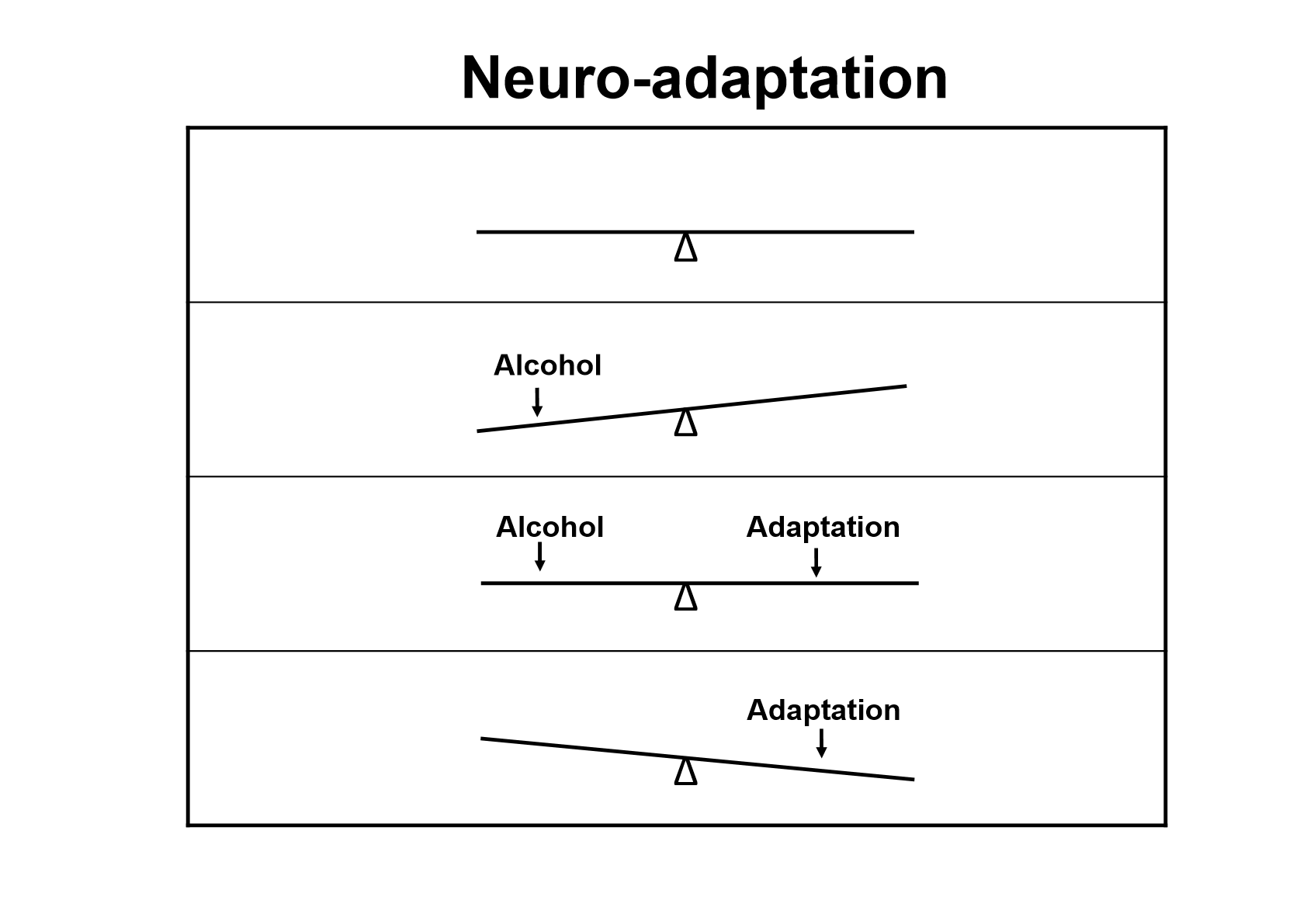
Neuro-adaptation *
Too much glutamate=increased, can lead to psychosis, convulsions and death
Gaba=inhibited, slow, death
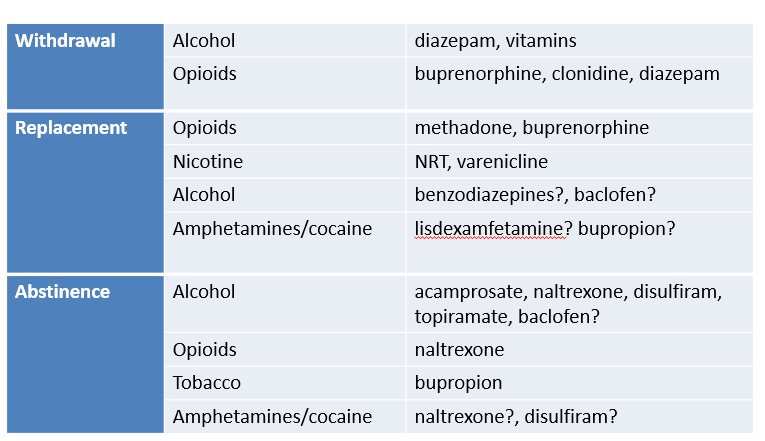
Pharmacotherapy for dependence:
3 paradigms
Actions of Alcohol: enhance and inhibit what? Indirectly does what?
•Enhance GABA-A function
–acts to facilitate GABA action at the receptor
•Inhibit NMDA Glutamate function
•Indirectly:
–release of dopamine
–release of serotonin
-release of endorphins
Neuropharmacology of alcohol:
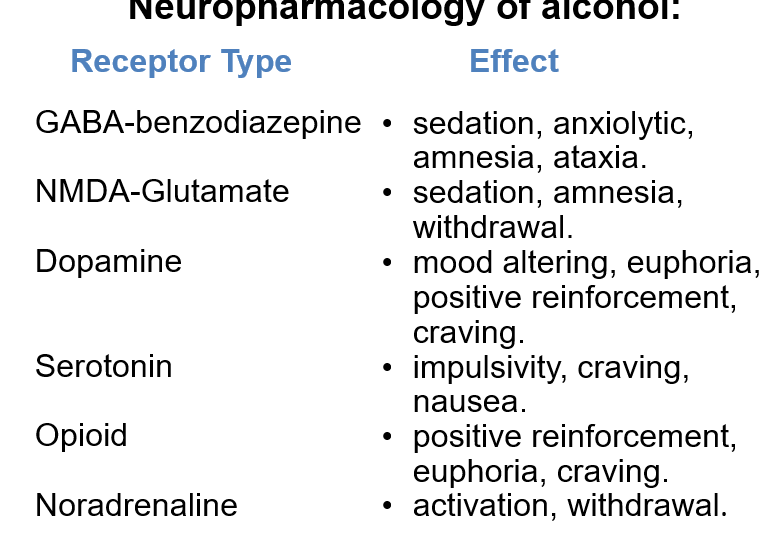
GABA-benozodiazapine effects
•sedation, anxiolytic, amnesia, ataxia.
NMDA-Glutamate
•sedation, amnesia, withdrawal.
Dopamine
•mood altering, euphoria, positive reinforcement, craving.
Serotonin
•impulsivity, craving,
nausea.
Opioid
•positive reinforcement, euphoria, craving.
Noradrenaline
•activation, withdrawal.
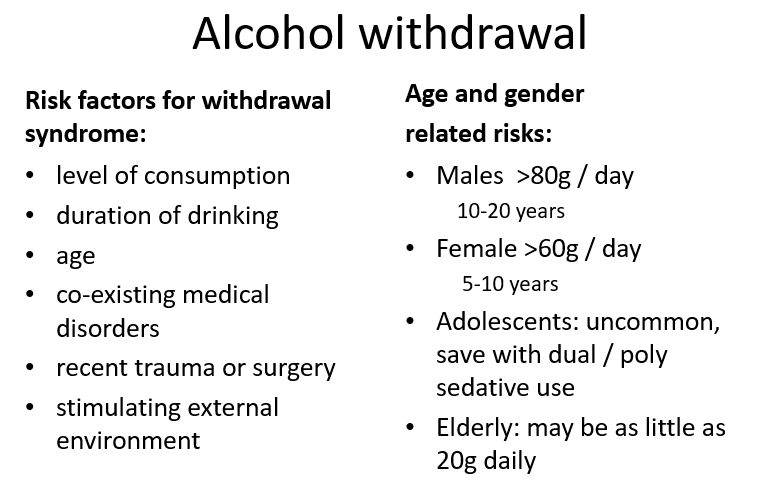
Alcohol withdrawal, risk factors and age and gender related risks
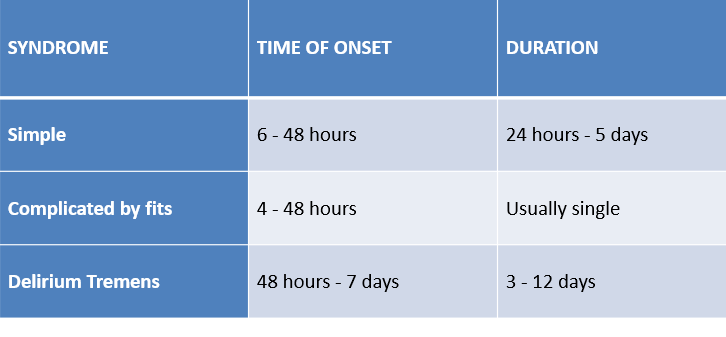
Alcohol Withdrawal, time of onset an duration (simple, complicated by fits and delirium tremens)
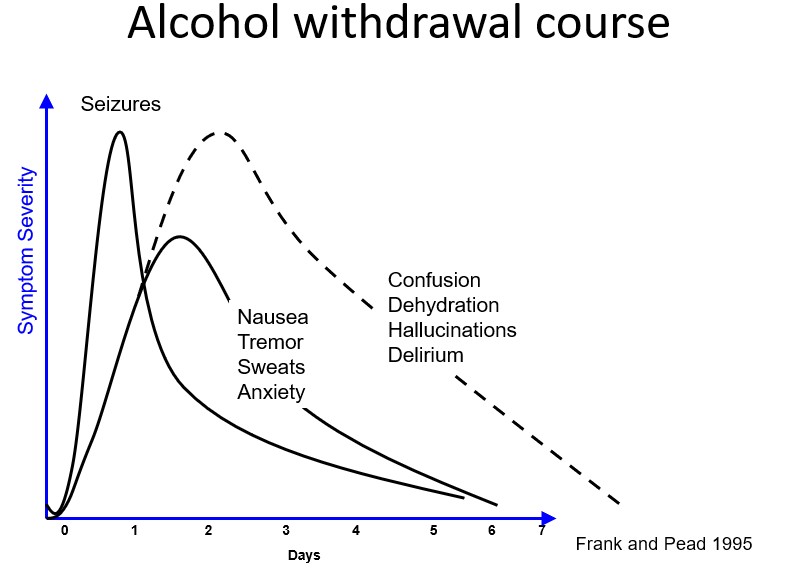
Alcohol withdrawal course
siezures last the shortest then nausea tremor sweats anxiety and then confusion ect last the longest
the nausea ect arent as severe as the others
Features of Alcohol Withdrawal (the 3 syndromes again)
Alcohol withdrawal - principles of management - 1/2
Assess risk
•severity of dependence
•previous withdrawals
•co-existing BZD dependence
•co-existing medical disorders
•? Suitable for ambulatory withdrawal
•Monitor progress i.e. daily review
•Treat agitation / hyperactivity
•Liaise with other health workers involved in care
-case conferencing, care planning
-early engagement with an A&D counsellor
•Assess for suicidality
Alcohol withdrawal - principles of management - 2/2
•thiamine IM (100mg) at least daily (Wernicke’s encephalopathy prophylaxis)
•Thiamine 100mg tds oral & multivitamins
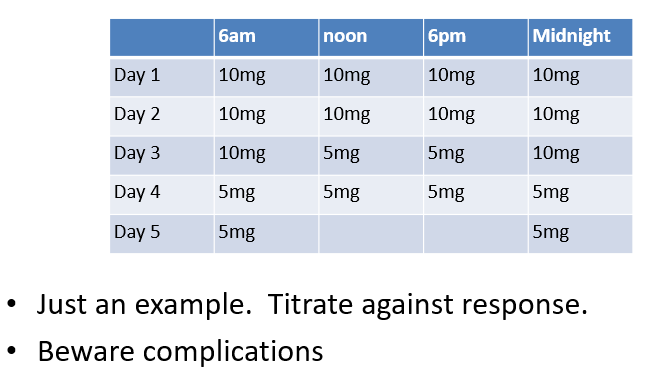
•Use a sedative with anti-convulsant properties
•diazepam is preferred - titrate with withdrawal symptoms (alcohol withdrawal scale AWS or CIWA-Ar)
•Ensure that symptoms improving each day
Example diazepam for alcohol withdrawal
After withdrawal, what next? 3 components
Gordon Livingston MD: “Too Soon Old, Too Late Smart” 2005
•Something to do
•Someone to love
•Something to look forward to
The 4 key ingredients in Recovery (Vaillant 2003)
•Finding a non-pharmacological substitute
•Compulsory supervision
•New relationships
•Involvement in spiritual programs
Pharmacotherapy for alcohol dependence =FDA-approved prescription medications used to treat Alcohol Use Disorder (AUD)
Naltrexone and Acamprosate most important ones?
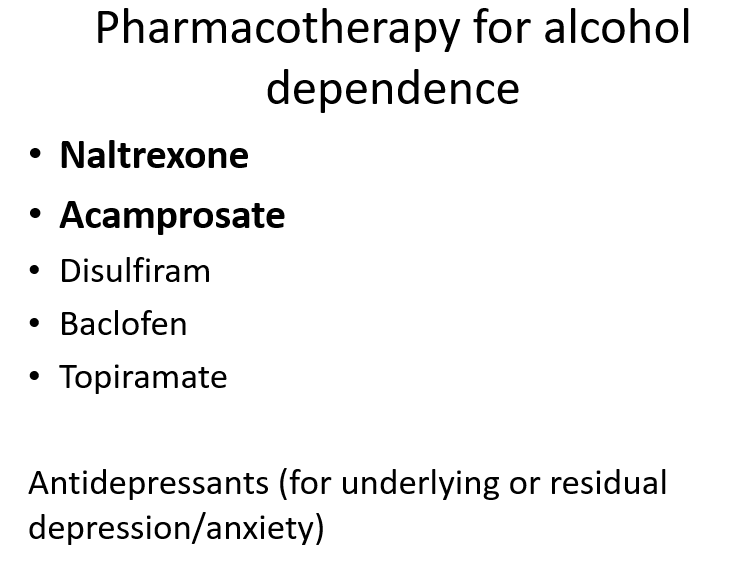
Naltrexone
•Pure m-opioid receptor antagonist
•Blocks the reinforcing effects of alcohol mediated by β-endorphin
•Dose 50-100mg daily
•Caution re LFTs and Opioids / Dependence
•sleep disturbance ?depression
•Not a “magic cure”
•Better with supportive Rx
•Abstinence model….
•Minor SE, hepatitis most serious
•Not if receiving opioids
•Not in pregnancy
Acamprosate
•A derivative of the amino-acid, taurine
•6 tablets x 333mg daily if > 60kg (ie 2 tds) (<60kg 2 bd)
•Agonist at GABAA receptor
•Facilitates GABAergic inhibitory neurotransmission
•Antagonist at excitatory NMDA Glutamate receptor
•GI side effects
•Not a “magic cure”
•Better with supportive Rx
•Better for abstinence
•Few SE, rash, diarrhoea, no interactions
•Not in renal failure
Not in pregnancy
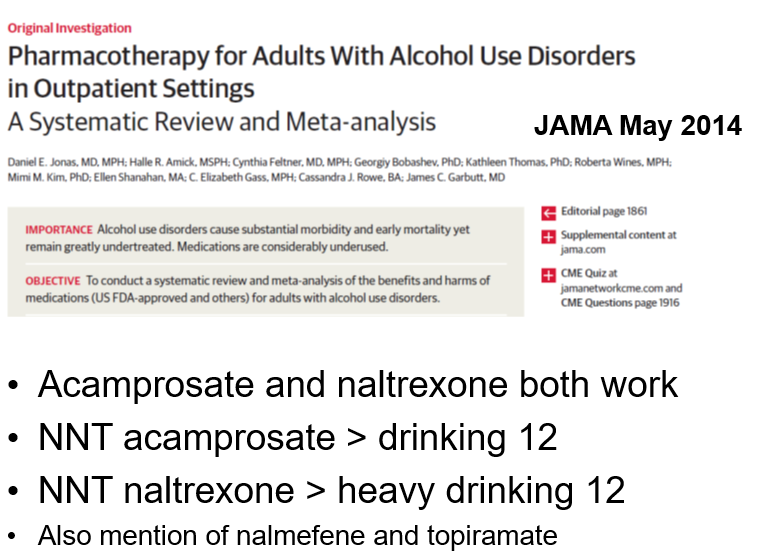
jama May study JONAS
NNT = Number Needed to Treat
It tells you how many people need to receive a treatment for one person to benefit.
NNT ≈ 12 for acamprosate → About 12 people need treatment for one additional person to stay abstinent compared to placebo.
NNT ≈ 12 for naltrexone (heavy drinking) → About 12 people need treatment for one person to reduce heavy drinking episodes.
Alcohol-sensitising drugs- the ones that give you a bad feeling
•Aldehyde dehydrogenase inhibitors
–disulfiram (“Antabuse”) 100 - 500mg daily
•Very unpleasant flush reaction if alcohol is taken
•Indications:
–alcohol dependence
–accepts goal of abstinence
–need for external aid to abstinence
–high risk situations for drinking imminent
•Abstinence may be higher first 3-6 months when patients take these drugs (not supported by EBM)
•Best given under supervision with contingency management
•Caution re inadvertent alcohol exposure
Not subsidised on PBS (~$80/month)
What about AA?
1 year abstinence is how much%?
Vaillant reports 100 P’s w A dependence and AA 10 yr follow up
?% achieved 3 yrs abstinence?
?% drank intermittently?
?% continued high A intake?
•Decentralised community based idea from Ohio (Bill W & Dr Bob in 1935)
•1 yr abstinence 25-50%
•Vaillant reported (1983) 100 patients with alcohol dependence and AA 10 yr follow up:
–29% achieved 3 yrs abstinence
–24% drank intermittently
–49% continued high alcohol intake
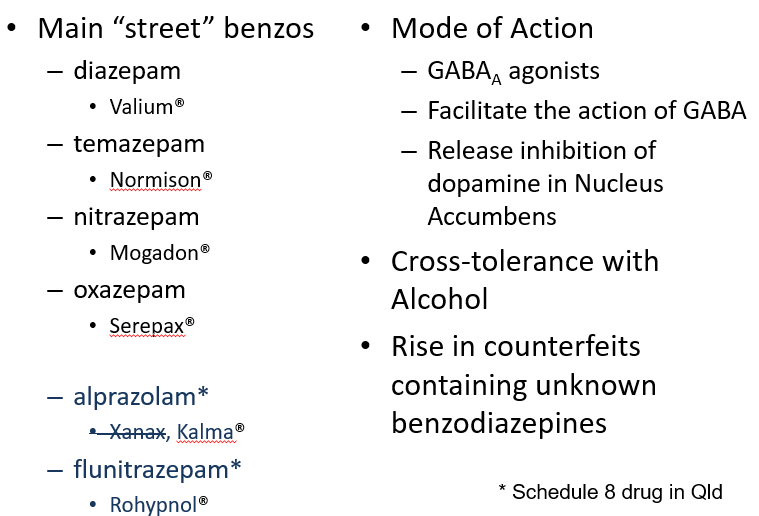
Benzodiazepines
Simple benzodiazepine withdrawal (somatic and psychological symptoms)
•Somatic symptoms
–tremor, muscle twitching, fasciculation
–aching and stiffness of muscles
–dizziness
–headache, visual disturbance
–gastrointestinal symptoms
•Psychological symptoms
–anxiety, agitation, insomnia, irritability
–depression
–perceptual distortions (“cotton wool” feelings)
Complicated benzodiazepine withdrawal
•Tonic-clonic seizures
•Delirium
–clouding of consciousness
–paranoid ideation/delusions
–visual and auditory hallucinations
Elective weaning from long term benzodiazepines
•Do not stop abruptly
•Switch to long-acting drug in equivalent dose
•Generally use diazepam
•Balance slow withdrawal and rapid withdrawal (with more intense symptoms which resolve earlier)
•Stepwise dose reduction, 10-15%, weekly - fortnightly
•Some patients need intensive support
•Regular monitoring
Risks with “street” drugs
•Variable strength increases risk of overdose
•May be ‘cut’ with toxic contaminants
–amphetamine used to be cut with strychnine
–Outbreaks of clostridia infection in Europe >50 deaths
–2008 >1000 deaths in USA re heroin cut with fentanyl
–previous levamisole cut with cocaine in Australia - > deaths
•Contaminants may be poorly soluble i.e. talc / gel-caps
•Risk of contamination with pathogens
–Buprenorphine and mouth flora
•Synthetics ie THC >90% would prefer the real thing
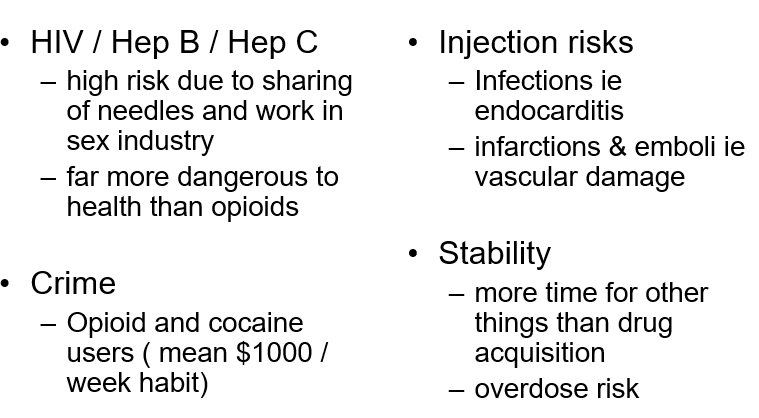
Harm reduction: Replacement prescribing, Needle & Syringe progs, Safer $ex
Story of HIV arrival in Edinburgh (1983):
Police confiscating needles & works -> shooting galleries
HIV +ve man arrived from Spain in the drug scene
Relative shortage of heroin -> more IV use
Net result was 70-80% IV users ended up HIV +ve
Initial effects of opioids
•Initially marked nausea / vomiting
•Rush – prickly itchy skin
•Drowsiness (the nod)
•Difficulty concentrating
•Euphoria (occasional anxiety)
•Altered pain threshold and perception
•Dry mouth, constipation, itching, sweating
•Pin point pupils, reduced respirations
Chronic opioid use
•Tolerance (may ‘tolerate’ 500mg morphine within 10 days)
•Dysphoria, depression, irritability, hypochondria
•Growing problem in patients with persistent pain disorder (low back / headache / fibromyalgia)
•\
•Still constipated and pupils pin-point
Opioid withdrawal - 1
•Onset of withdrawal reflects T½ (half life of opioid)
•Short T½ (e.g. heroin) 6-12 hours, peak at 24-48 hrs
•Long T½ (e.g. methadone) 2-3 days, peak at 7 - 10 days, may continue weeks
•Drug seeking behaviour may occur within a few hours and is often the principal manifestation after 72 hours
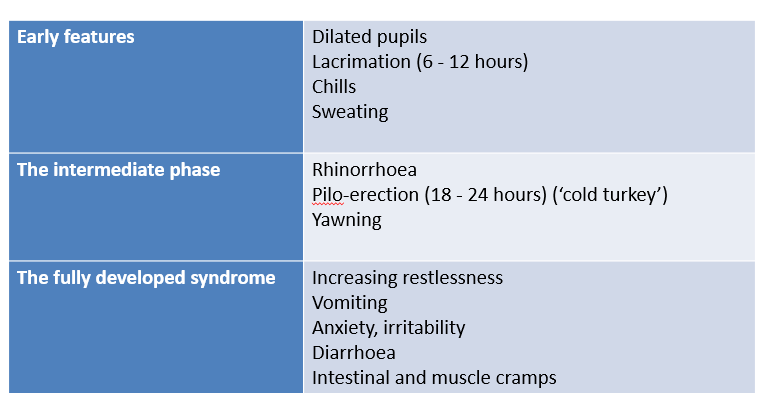
Opioid withdrawal - 2 (early, intermediate, fully developed)
Opioid withdrawal treatment
ie ‘detoxification’
•Buprenorphine, a partial opioid agonist, has transformed withdrawal
•Reduces heroin use in out-patient settings
•Long acting i.e. out-patient once daily dosing
•Duration of treatment: 4-8 days
•Daily dose regime: 8, 8, 6, 4, 2, 2 mg or similar
•Daily review
•Does carry risks…
Buprenorphine
(Subutex / Suboxone)
•Provides general relief so other symptomatic medications for opioid withdrawal are not routinely required
•Possible role for Long-Acting Injectable Buprenorphine (LAI-B) for “slow withdrawal”
•
•Unsupervised use of other sedative drugs in combination with buprenorphine can result in respiratory depression, coma and death