Theoretical Foundations of Neurologic Rehabilitation
1/139
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
140 Terms
what is a THEORY
is a speculation, general idea + notion
- not directly testable
- abstract
what can a THEORY be used to generate
testable hypotheses
in principle, what are SCIENTIFIC THEORIES always classified as
tentative + subject to corrections/inclusions in a wider theory
what are 2 REASONS why we need THEORIES
1. framework for interpreting behavior
2. guide for clinical action
what are 2 CHARACTERISTICS that THEORIES should always be
1. changing
2. dynamic
what are the 3 MOTOR CONTROL THEORIES
1. reflex
2. hierarchical
3. systems
what is the REFLEX THEORY based on
classic experiments of Sir Charles Sherrington ("reduced" cat preparations)
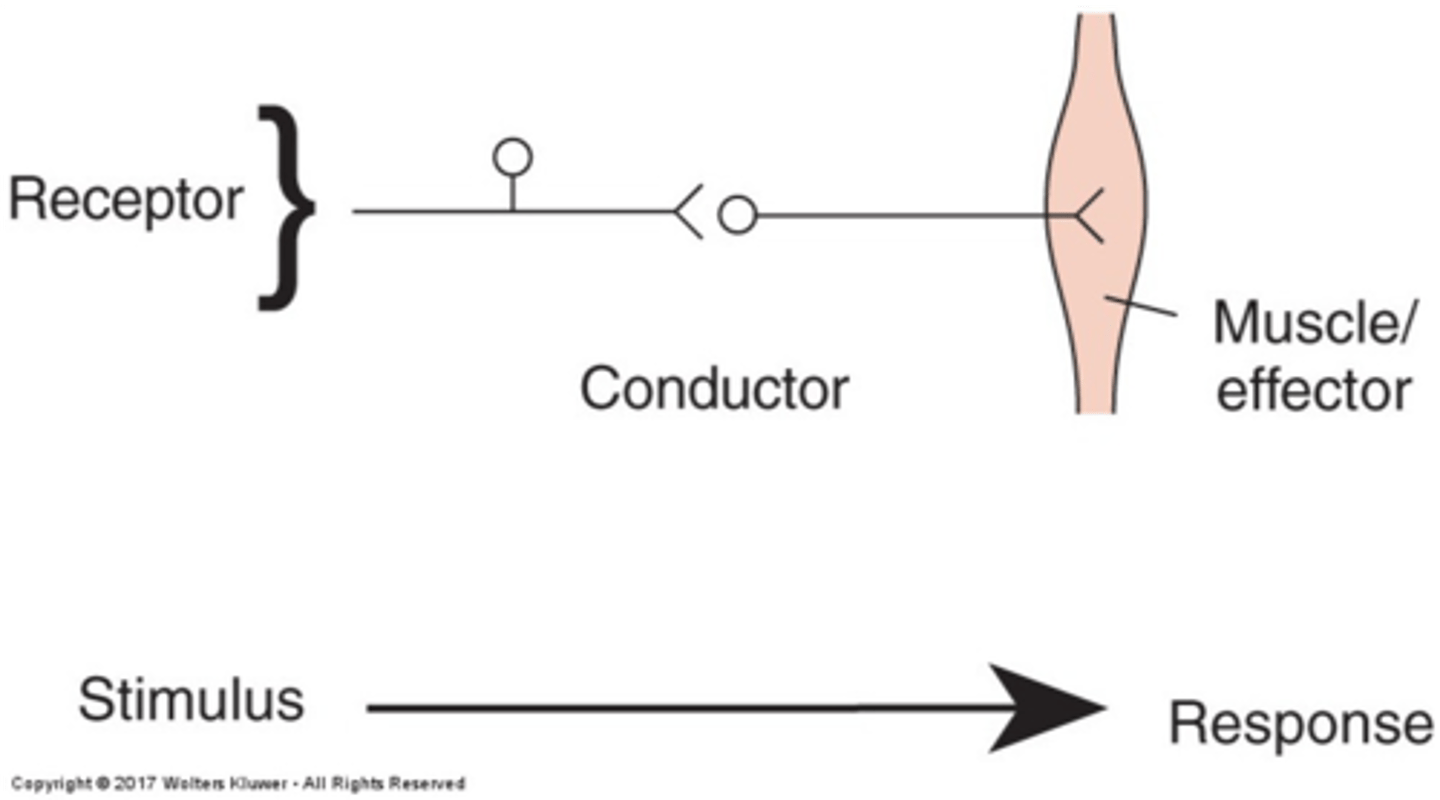
what does the REFLEX THEORY state
all movements are based on simple reflexes + there's a stimulus that causes a response
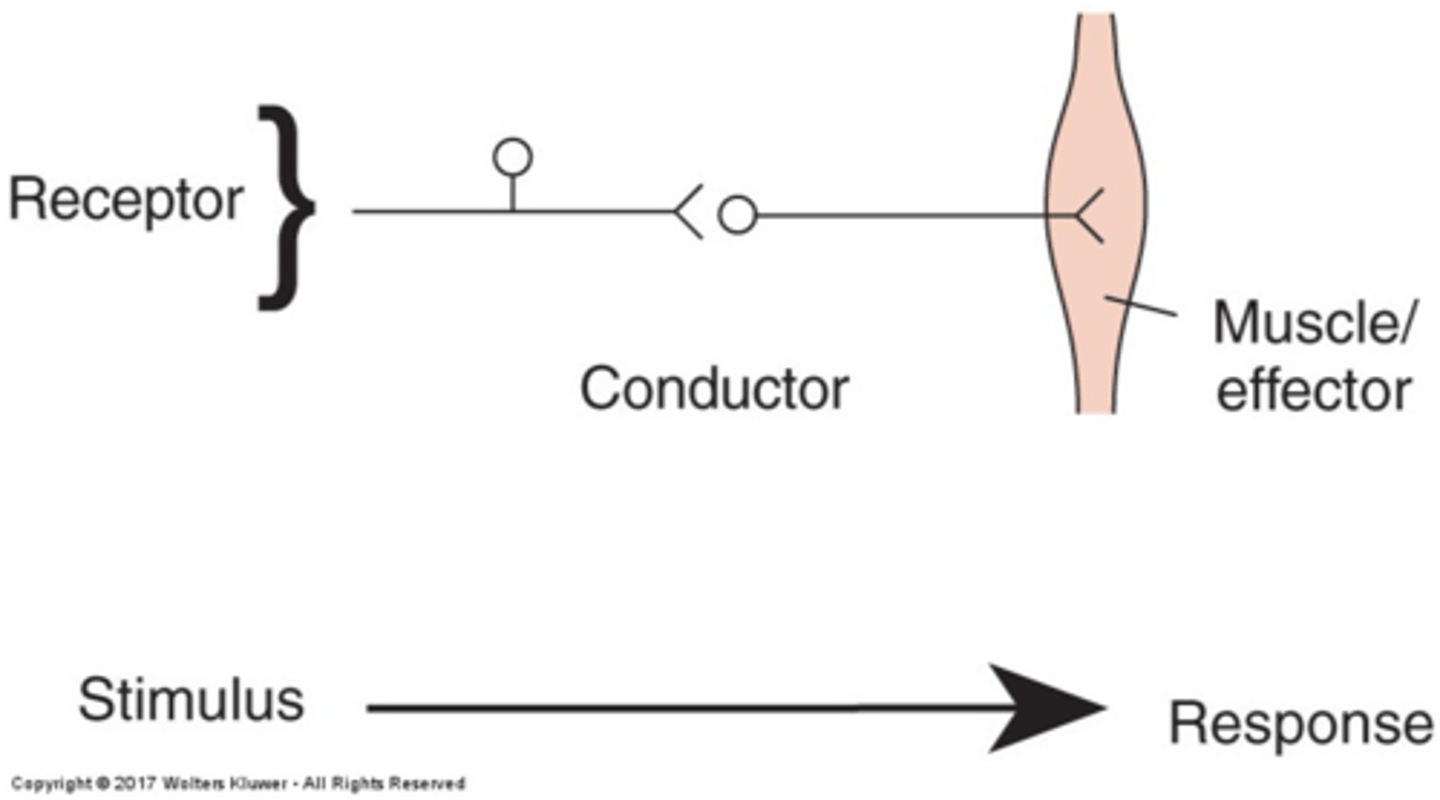
what are 3 ASSUMPTIONS of the REFLEX THEORY
1. sensory inputs control motor outputs
2. sensation in necessary for movement
3. movement is a summation of reflexes
what are 3 LIMITATIONS of the REFLEX THEORY
1. de-afferented animals show coordinated movement
2. open-loop control demonstrated
3. anticipatory, feed-forward control
what is the CLINICAL IMPLICATIONS of the REFLEX THEORY
use of reflexes to facilitate movement
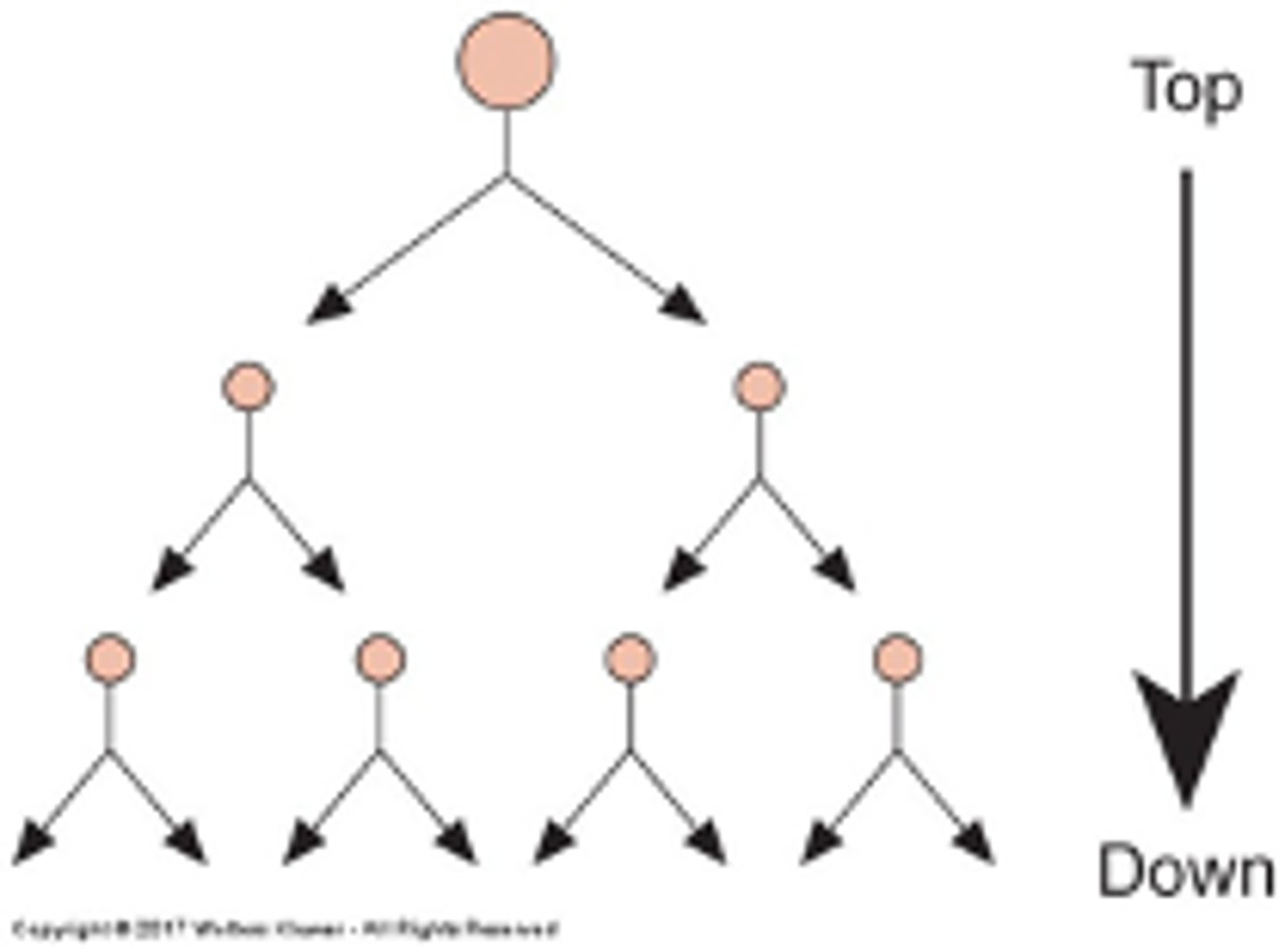
what is the HIERARCHICAL THEORY based on
top-down structure
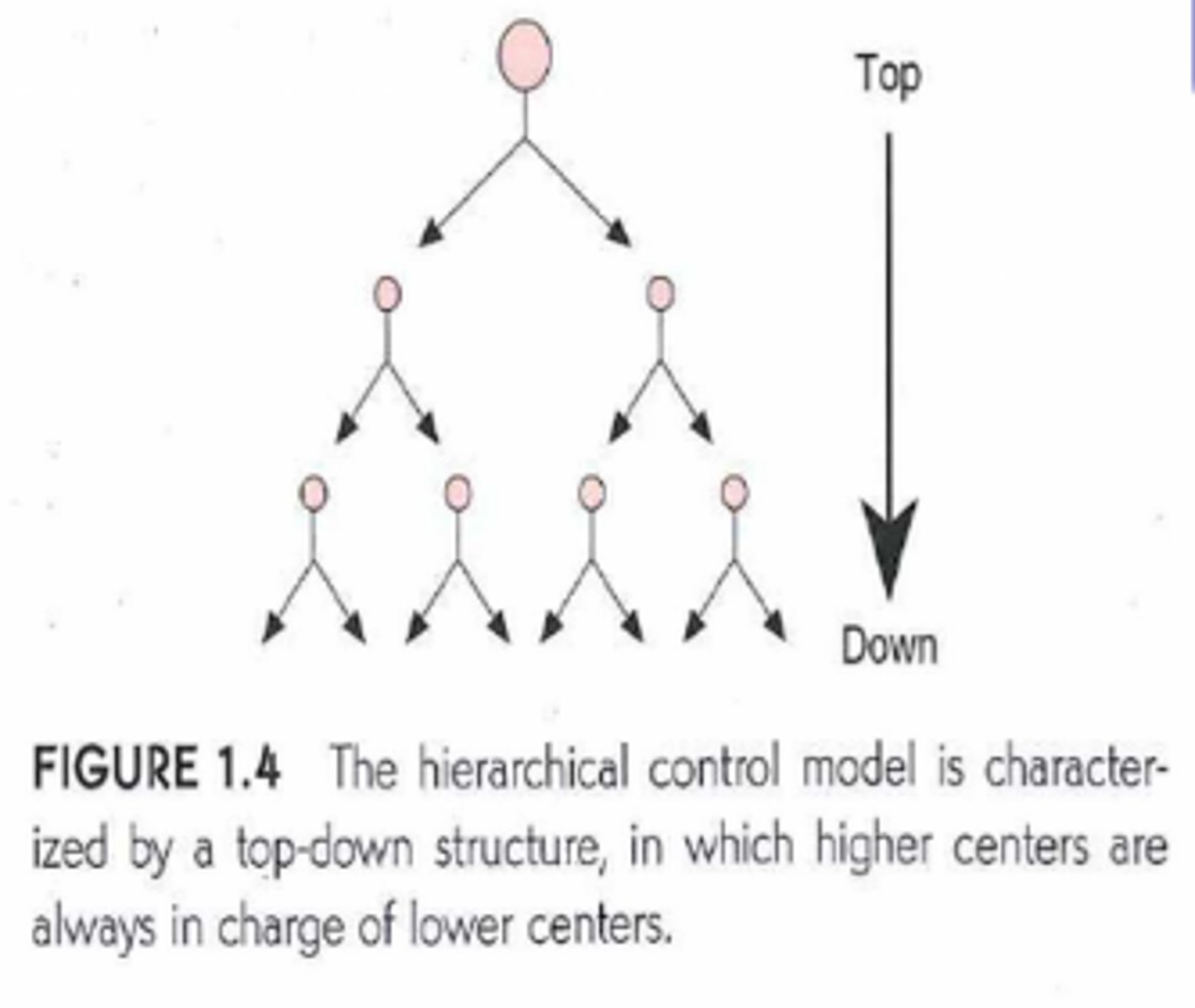
regarding the HIERARCHICAL THEORY, what does TOP-DOWN STRUCTURE state
that the higher centers are always in charge of the lower centers
who was the key figure in proposing the HIERARCHICAL THEORY
Sir Hughlings Jackson (english neurologist)
what has the HIERARCHICAL THEORY formed a basis for
clinical neurology up to current
what are 4 ASSUMPTIONS of the HIERARCHICAL THEORY
1. central programs/reflexes control muscle activation patterns
2. organization is top down
3. motor control emerges from reflexes + nested in a hierarchy of levels in CNS
4. recovery from injury follows a pattern similar to child development
regarding the HIERARCHICAL THEORY assumptions, recovery from injury follows what PATTERN
follows step like pattern similar to CHILD DEVELOPMENT
what are 4 LIMITATIONS associated with the HIERARCHICAL THEORY
1. locomotion in spinal cats (low level of control)
2. central pattern generators (CPGs)
3. development not step like following CNS damage
4. blurred distinctions between voluntary + reflex
what do CENTRAL PATTERN GENERATORS (CPGs) generate
reciprocal movements linked to optimizing energy expenditure
where are CENTRAL PATTERN GENERATORS (CPGs) mainly located
in spinal cord
what are 2 CLINICAL IMPLICATIONS associated with the HIERARCHICAL THEORY
1. lesions disrupt high level control of lower level reflexes
2. goal: facilitate normal mature reflex action + inhibit more primitive reflexes
regarding the HIERARCHICAL THEORY, what is the THERAPY GOAL
facilitate normal mature reflex action + inhibit more primitive reflexes
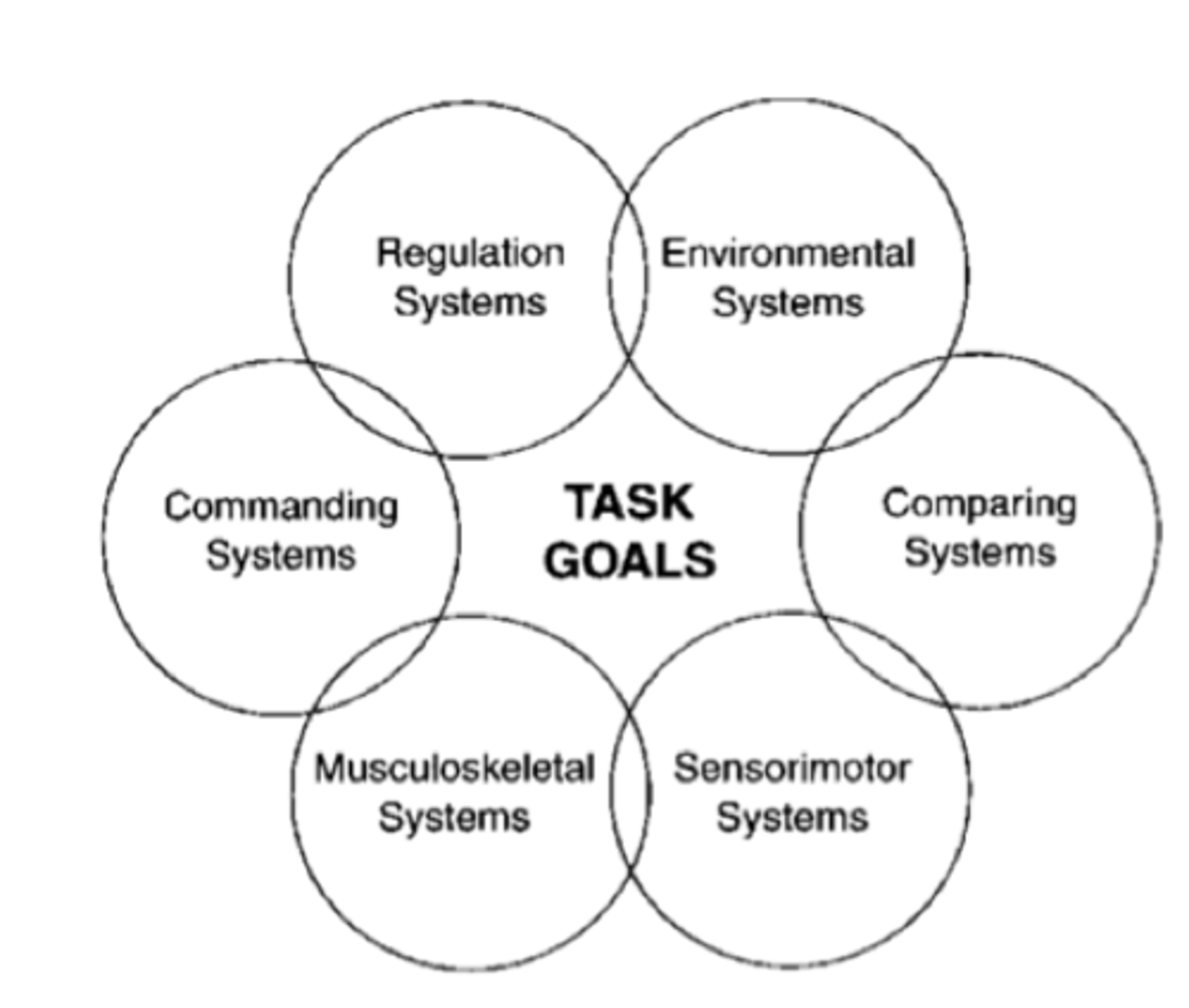
what is the SYSTEMS THEORY of MOTOR CONTROL based on
task goals is the center of treatment + movements aren't solely controlled by a central command, but rather by interactions among multiple systems
who first proposed the SYSTEMS THEORY of MOTOR CONTROL in 1932
nicoli bernstein
what are 3 ASSUMPTIONS associated with the SYSTEMS THEORY of MOTOR CONTROL
1. adaptive anticipatory mechanisms
2. reflexes + synergies are normal strategies to limit degrees of freedom
3. interactive systems on same level control motor behavior to achieve task
what are 3 LIMITATIONS associated with the SYSTEMS THEORY of MOTOR CONTROL
1. lack of consensus on terminology + definitions
(dynamic action, distributed control + ecological theory)
2. difficult for scientific study
3. relation of neuroanatomy to systems unclear
what are 2 CLINICAL IMPLICATIONS associated with the SYSTEMS THEORY of MOTOR CONTROL
1. movement organized around behavioral goals
(e.g. weight shifting)
2. motor deficits following brain damage not only reflect lack of neural control but reflect best attempt by remaining system to accomplish task/goal
("abnormal" synergy hierarchical vs systems)
what is the purpose of using NEUROLOGIC REHABILITATION PHILOSOPHIES
to build frame work for treatment
what should NEUROLOGIC REHABILITATION PHILOSOPHIES be based on
latest research + scientific knowledge in many areas (i.e. motor)
what 5 AREAS should the NEUROLOGIC REHABILITATION PHILOSOPHIES be based on
1. motor control
2. motor learning
3. recovery of function
4. nervous system plasticity
5. psychology + sociology
what are 3 NEUROLOGIC REHABILITATION PHILOSOPHIES
1. muscle re-education
2. neurotherapeutic facilitation
3. contemporary task-oriented
who FIRST ADVOCATED for MUSCLE RE-EDUCATION
sister kenny
why did SISTER KENNY advocate for MUSCLE RE-EDUCATION
for treatment of poliomyelitis + felt patients would benefit from activity
what 2 MOTOR CONTROL THEORIES is MUSCLE RE-EDUCATION not really based on
1. hierarchical theory
2. reflex theory
PRIOR to MUSCLE RE-EDUCATION, what would the patients do
patients waited in bed to see what their outcomes would be
what is MUSCLE RE-EDUCATION based on
ISOLATED MUSCLE FUNCTION not systems model of motor control
what are the 4 THERAPEUTIC AIMS associated with MUSCLE RE-EDUCATION
1. isolate muscle actions by focusing on individual muscles
2. maximize strength + use of motor units remaining
3. teach functional activities
4. provide orthopedic support
what are 3 DISSATISFACTIONS associated with MUSCLE RE-EDUCATION
1. CNS plasticity not considered
2. can't isolate muscle action in upper motor neuron lesions
3. not lack of muscle activation but abnormal patterns often a problem
what 2 MOTOR CONTROL THEORIES is NEUROTHERAPEUTIC FACILITATION based on
1. reflex theory
2. hierarchical theory
who developed NEUROTHERAPEUTIC FACILITATION in the 1950s
therapists + physicians dissatisfied with muscle re-education model of rehab
what did the therapists + physicians who developed NEUROTHERAPEUTIC FACILITATION want
to affect nervous system itself rather than secondary effects of change to muscles + joints
what are the 4 THERAPEUTIC AIMS associated with NEUROTHERAPEUTIC FACILITATION
1. facilitate normal movement through proprioceptive input
2. modify CNS by allowing patient to experience "normal movement"
3. inhibit abnormal tone, primitive reflexes + synergies
4. don't allow CNS to learn abnormal patterns of movement
what are 4 DISSATISFACTIONS associated with NEUROTHERAPEUTIC FACILITATION
1. little functional carryover
2. patients passive recipients of therapy
3. doesn't look at biomechanical, musculoskeletal + environmental constraints
4. inhibiting abnormal reflexes doesn't necessarily allow normal movement
what is the NEWER THEORY of NEUROLOGIC REHABILITATION
contemporary task-oriented
what 3 MOTOR CONTROL THEORIES is CONTEMPORARY TASK-ORIENTED based on
1. reflex theory
2. hierarchical theory
3. systems model of motor control
what does CONTEMPORARY TASK-ORIENTED target (2)
1. peripheral nervous systems (musculoskeletal + environment)
2. central nervous system
what are 3 THERAPEUTIC AIMS associated with CONTEMPORARY TASK-ORIENTED
1. treatment centered around achievement of task/goal
2. "teach" problem solving skills (so adaptable to different contexts)
3. be aware of musculoskeletal + environmental factors
what are 4 DISSATISFACTIONS associated with CONTEMPORARY TASK-ORIENTED
1. no scientific consensus on definitions + terminology
2. requires cognitive processing by patient
3. hard to provide time consuming practice of skills
4. no specific techniques + requires creativity + thinking by therapist
what are 6 THERAPEUTIC TREATMENT APPROACHES
1. neuromuscular development treatment (NDT)
2. Brunnstrom
3. proprioceptive neuromuscular facilitation (PNF)
4. Rood
5. Johnstone
6. task-oriented
who developed the NEUROMUSCULAR DEVELOPMENT TREATMENT (NDT)
karl + berta bobath
what 2 MOTOR CONTROL THEORIES is NEUROMUSCULAR DEVELOPMENT TREATMENT (NDT) based on
1. reflex theory
2. hierarchical theory
what belief is the NEUROMUSCULAR DEVELOPMENT TREATMENT (NDT) based on
"spasticity" is due to release of gamma system from higher control which releases abnormal reflexes
what are 9 TREATMENT EMPHASIS associated with NEUROMUSCULAR DEVELOPMENT TREATMENT (NDT)
1. inhibit abnormal reflex patterns
2. special handling techniques used to facilitate movement patterns of higher control
3. avoid reinforcing abnormal movements
4. don't use associated reactions
5. treatment should be active + dynamic
6. need to establish righting + equilibrium reactions to allow foundation for normal movement
7. rotation is important to separate upper + lower trunk control
8. use sensory input to give patient a more normal sensation of movement
9. patient will learn midline only by moving in + out of it
what should the treatment be like for NEUROMUSCULAR DEVELOPMENT TREATMENT (NDT)
active + dynamic
regarding NEUROMUSCULAR DEVELOPMENT TREATMENT (NDT), what reflex patterns should be inhibited
abnormal reflex patterns
regarding NEUROMUSCULAR DEVELOPMENT TREATMENT (NDT), what motion is important to separate upper + lower trunk control
rotation
regarding NEUROMUSCULAR DEVELOPMENT TREATMENT (NDT), what will a patient learn
MIDLINE by moving in + out of it
regarding NEUROMUSCULAR DEVELOPMENT TREATMENT (NDT), what needs to be established to allow foundation for normal movement
righting + equilibrium reactions
what 5 KEY TERMS is associated with NEUROMUSCULAR DEVELOPMENT TREATMENT (NDT)
1. inhibition
2. facilitation
3. reflex inhibiting postures
4. key points of control (clavicle + lower back)
5. trunk control
who developed BRUNNSTROM
signe brunnstrom
what 2 MOTOR CONTROL THEORIES is BRUNNSTROM based on
1. hierarchical theory
2. reflex theory
what belief is BRUNNSTROM based on
patients in early recovery from CVA should be assisted to gain use of limb synergy movement patterns
regarding BRUNNSTROM, what is the necessary MILESTONE for further recovery
synergistic movements
regarding BRUNNSTROM, what is considered the primitive spinal cord pattern
basic limb synergies
regarding BRUNNSTROM, what is EVALUATION + PROGRESS based on
six stages of recovery
what is STAGE 1 of RECOVERY regarding BRUNNSTROM
no volitional movement initiated (flaccid)
what is STAGE 2 of RECOVERY regarding BRUNNSTROM
appearance of basic limb synergy (beginning of spasticity)
what is STAGE 3 of RECOVERY regarding BRUNNSTROM
synergies are performed voluntarily (spasticity increases)
- get through most ROM in a synergistic pattern
what is STAGE 4 of RECOVERY regarding BRUNNSTROM
movement patterns no longer totally dictated by synergy (spasticity begins to decrease)
- isolate some movement out of synergies
what is STAGE 5 of RECOVERY regarding BRUNNSTROM
increased movement out of limb synergies (spasticity continues to decrease)
- more functional movements
what is STAGE 6 of RECOVERY regarding BRUNNSTROM
isolated joint movements are performed with coordination
what are 4 SYNERGY PATTERNS
1. upper extremity flexion
2. upper extremity extension
3. lower extremity flexion
4. lower extremity extension
what 2 SYNERGY PATTENS are UMN PROBLEMS dominated by
1. upper extremity flexion
2. lower extremity extension
what are the 2 STRONGEST SYNERGY PATTERNS
1. UE flexion
2. LE extension
what are 5 FLEXOR SYNERGIES of the UPPER EXTREMITY
1. retraction (of scapula)
2. external rotation
3. abduction
4. elbow flexion
5. supination
what is the WEAKEST UE FLEXOR SYNERGY PATTERN
abduction
what is the STRONGEST UE FLEXOR SYNERGY PATTERN
elbow flexion
what are 5 EXTENSION SYNERGIES of the UPPER EXTREMITY
1. protraction (of scapula)
2. internal rotation
3. adduction
4. elbow extension
5. pronation
what is the WEAKEST UE EXTENSOR SYNERGY PATTERN
elbow extension
what are the 2 STRONGEST UE EXTENSOR SYNERGY PATTERNS
1. adduction
2. pronation
what are 6 FLEXION SYNERGIES of the LOWER EXTREMITY
1. hip flexion
2. hip abduction
3. hip external rotation
4. knee flexion
5. ankle dorsiflexion/inversion
6. toe dorsiflexion
what is the STRONGEST LE FLEXION SYNERGY PATTERN
hip flexion
what are the 2 WEAKEST LE FLEXION SYNERGY PATTERNS
1. hip abduction
2. knee flexion
what are 5 EXTENSION SYNERGIES of the LOWER EXTREMITY
1. hip extension
2. hip adduction/internal rotation
3. knee extension
4. ankle plantarflexion/inversion
5. toe plantarflexion (great toe may extend)
what is the WEAKEST LE EXTENSION SYNERGY PATTERN
hip extension
what are the 2 STRONGEST LE EXTENSION SYNERGY PATTERNS
1. hip adduction/internal rotation
2. knee extension
what are the 6 TREATMENT EMPHASIS associated with BRUNNSTROM
1. strength testing should focus on patterns of movement rather than isolated joint motions
2. limb synergies are necessary milestones for recovery
3. encourage + assist patient in using limb synergies + associated reactions initially then out of synergy
4. all patients will follow stage of recovery but may not attain all 6
5. functional training (bed mobility + transfers) should utilize associated reactions + limb synergies if needed early on
6. associated reaction can be elicited during treatment even if patient is flaccid
regarding the TREATMENT EMPHASIS for BRUNNSTROM, what should STRENGTH TESTING focus on
PATTERNS OF MOVEMENT rather than isolated joint motions
regarding the TREATMENT EMPHASIS for BRUNNSTROM, what is a necessary MILESTONE for RECOVERY
limb synergies
regarding the TREATMENT EMPHASIS for BRUNNSTROM, what is a patient ENCOURAGED + ASSISTED IN
using limb synergies + associated reactions initially then out of synergy
regarding the TREATMENT EMPHASIS for BRUNNSTROM, what will all PATIENTS FOLLOW
stages of recovery (but may not attain all 6)
regarding the TREATMENT EMPHASIS for BRUNNSTROM, what should FUNCTIONAL TRAINING utilize
associated reactions + limb synergies (if needed early on)
regarding the TREATMENT EMPHASIS for BRUNNSTROM, what can be ELICITED during treatment if a patient is FLACCID
associated reaction
what are 3 KEY TERMS associated with BRUNNSTROM
1. limb synergies
2. associated reactions
3. stages of recovery
who were the 3 INDIVIDUALS that developed PROPRIOCEPTIVE NEUROMUSCULAR FACILITATION (PNF)
1. kabat
2. knott
3. voss
what is PROPRIOCEPTIVE NEUROMUSCULAR FACILITATION (PNF) based on
idea that stronger parts of body movements are used to facilitate the weaker parts
regarding PROPRIOCEPTIVE NEUROMUSCULAR FACILITATION (PNF), what does NORMAL MOVEMENT + POSTURAL CONTROL rely on
balance between agonist + antagonist
regarding PROPRIOCEPTIVE NEUROMUSCULAR FACILITATION (PNF), what is there GREAT EMPHASIS ON
manual contacts + proper hand positioning to stimulate proprioceptors
what are 6 TREATMENT EMPHASIS for PROPRIOCEPTIVE NEUROMUSCULAR FACILITATION (PNF)
1. use diagonal patterns of movement (rarely move in straight planes of motion)
2. techniques must have accurate timing, specific commands + correct hand placement
3. verbal commands must be short + concise
4. repetition is essential for motor learning
5. give greater resistance if trying to achieve stability
- less resistance for mobility
6. techniques should be used that cause irradiation of strength from stronger to weaker muscles
regarding TREATMENT EMPHASIS for PNF, what should be USED
diagonal patterns of movement
(as we rarely move in straight planes of motion)