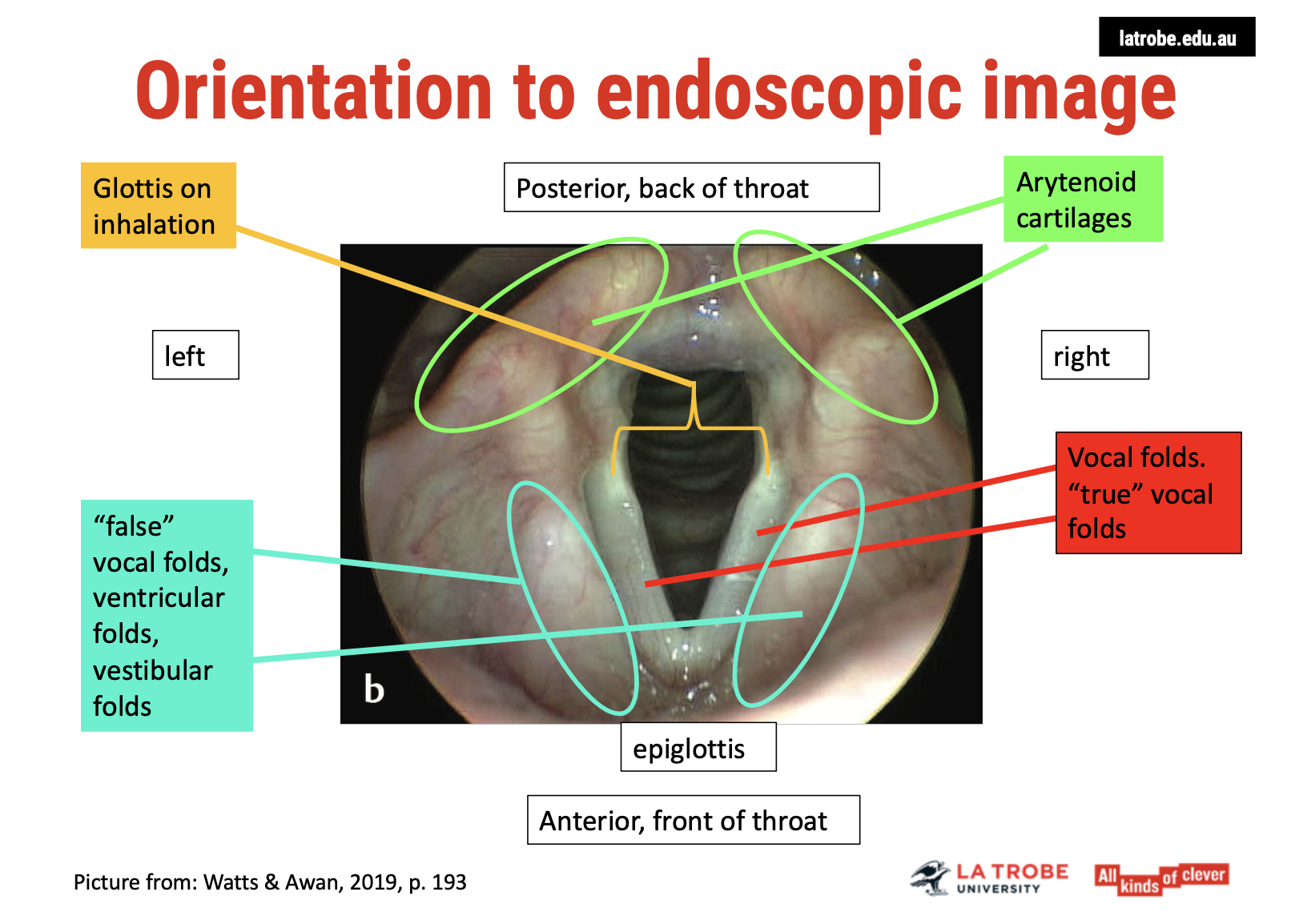
Visualisation of the larynx
1/9
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
10 Terms
Laryngeal Video Endoscopy & Stroboscopy: Standard of Care and Role of Speech Pathologists
1. Standard of Care for Clinical Voice Evaluation 🎯
2. Role of the Speech Pathologist in Endoscopy and Stroboscopy 🗣
While speech pathologists do not typically perform endoscopy or stroboscopy in most settings, they are essential in:
Identifying when stroboscopic evaluation is needed.
Referring patients for further assessment when necessary.
Speech Pathology Australia Guidelines:
Speech pathologists are not currently trained to perform these procedures unless they have received specific medical training and credentialing.
Endoscopy and stroboscopy may be conducted by speech pathologists only in approved medical settings, and they require additional training and institutional approval.
3. Training, Credentialing, and Limitations 📚
Credentialing and Training:
Speech pathologists must complete specific training courses or workplace credentialing programs to perform and interpret these procedures competently.
This training ensures competence in both the stroboscopy procedure and its interpretation.
Medical Benefits Scheme (MBS):
Even if a speech pathologist is trained to perform these procedures, MBS reimbursements are not available unless the procedure is performed by a medical practitioner.
Therefore, speech pathologists cannot charge MBS item numbers for stroboscopy procedures, even with appropriate training.
4. Key Takeaways for Entry-Level Graduates 🎓
Understanding:
As an entry-level graduate, it is essential to understand the role of laryngeal endoscopy and stroboscopy in voice assessment.
Familiarity with the advantages and limitations of these methods is necessary for making informed referrals.
Clinical Application:
While performing these evaluations and interpreting laryngeal images is not an entry-level skill, being aware of when to refer patients for such procedures is a critical part of the assessment process.
This approach helps ensure that voice assessments are conducted in a safe, ethical, and professionally supported manner while respecting the roles and responsibilities of different healthcare professionals.
Types of Endoscopes for Voice Assessment
1. Rigid vs. Flexible Endoscopes 🏥
Rigid Endoscope:
Inserted through the mouth.
Provides a larger, sharper image of the larynx.
Gag reflex can be a significant limitation in its use, making it uncomfortable for some patients.
Flexible Fibre Optic Endoscope:
Inserted through the nose (similar to the procedure used in Fibre Optic Endoscopic Evaluation of Swallowing or FEES).
Can be used with or without local anaesthetic (e.g., lidocaine), though anaesthetic is typically preferred to reduce discomfort, especially for nasal insertion.
Flexible scopes are generally more tolerable for patients, though the image quality is slightly less sharp compared to rigid endoscopes.
2. Endoscopic Equipment and Procedure 💻
Endoscope Attachment:
Both rigid and flexible endoscopes can be attached to a digital camera and monitor to provide a magnified view of the larynx and surrounding areas.
Local Anaesthetics:
Lidocaine (a common anaesthetic) is often sprayed into the nostrils for the flexible scope to reduce discomfort.
Decongestion of the nose may also be needed to improve visibility, especially if the patient’s nasal passages are congested.
3. Speech Pathology Australia Guidelines 📚
Position Statement:
Speech Pathology Australia has guidelines for the use of fibre optic endoscopes in clinical settings.
While speech pathologists can be involved in the assessment and interpretation of endoscopic evaluations, performing the procedure may require additional training and credentialing as per the national standards.
Image
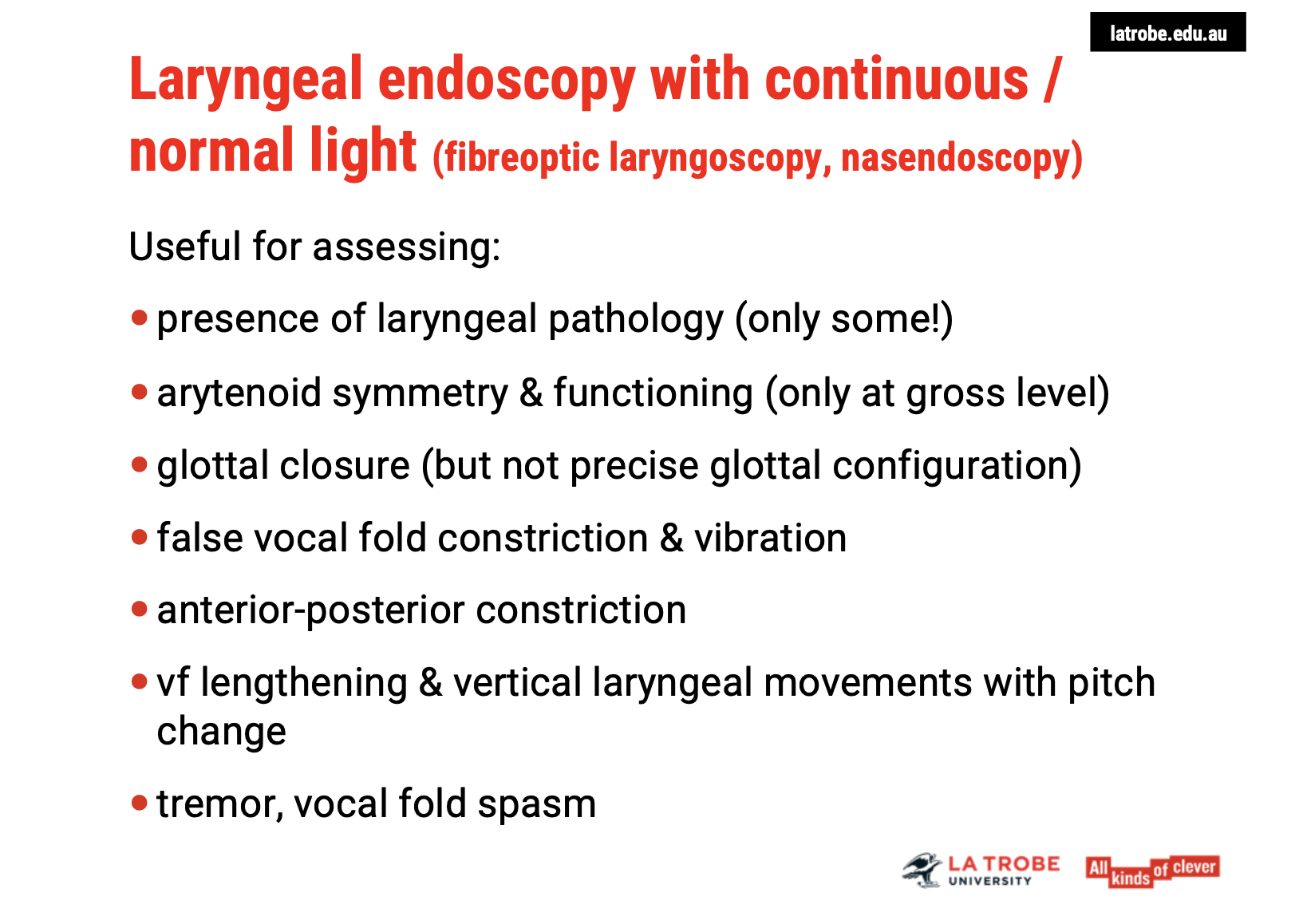
Uses of Endoscopy in Voice Assessment
1. Assessing Laryngeal Pathologies 🔍
Laryngeal Pathologies: Endoscopy helps identify the presence of laryngeal pathologies, such as growths, lesions, or inflammation in the vocal folds or surrounding areas.
Symmetry of the Arytenoids: It allows for the observation of symmetry in the arytenoid cartilages, which play a crucial role in voice production.
2. Evaluating Arytenoid Function 🔄
Gross Arytenoid Function: Endoscopy provides a general assessment of arytenoid functioning, which is essential for vocal fold movement and glottal closure during phonation.
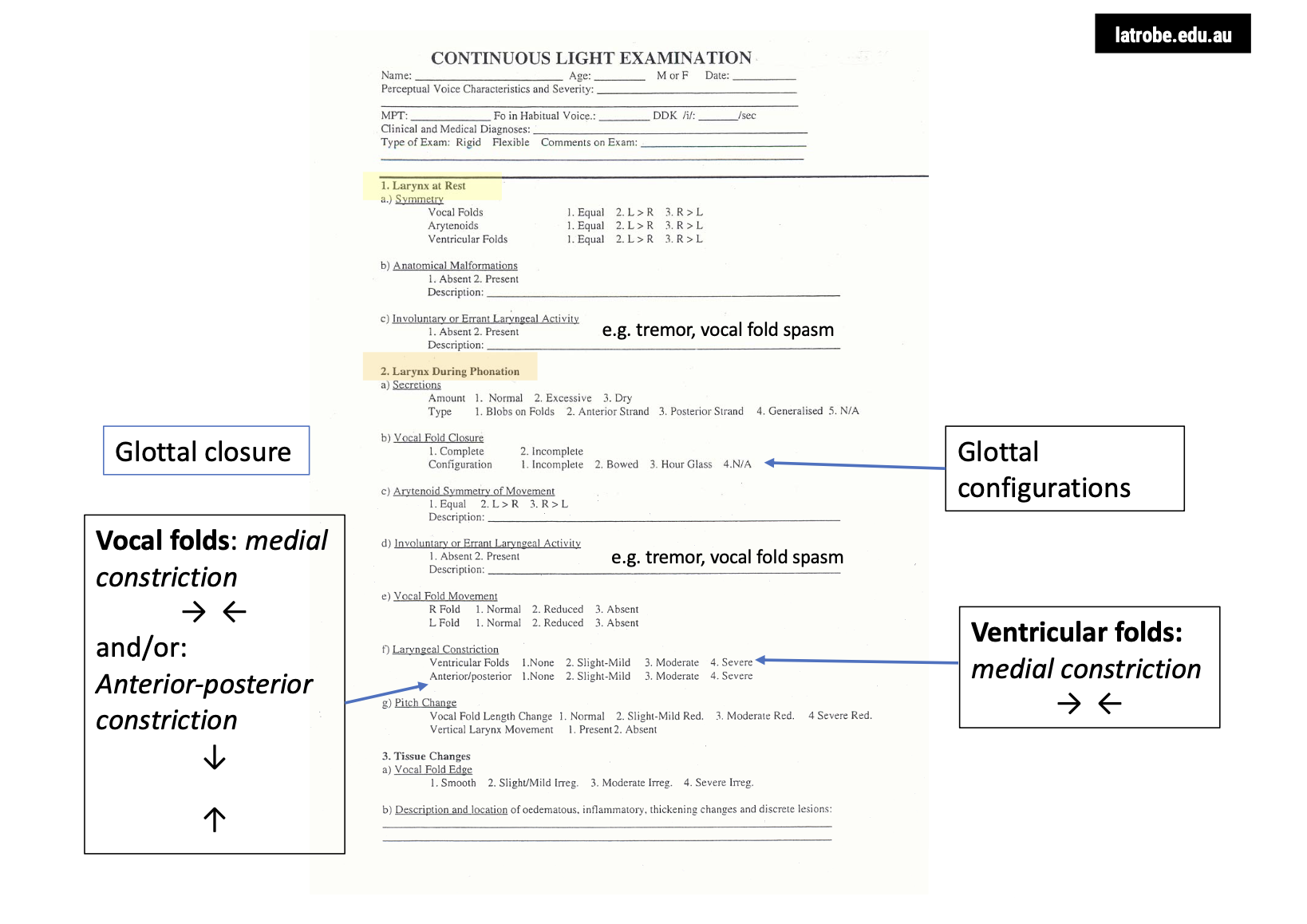
3. Glottal Closure and Configuration ⚖
Glottal Closure: Endoscopy allows observation of the glottal closure, which is critical for efficient voice production. However, it doesn't provide a precise glottal configuration.
4. False Vocal Fold Constriction 🎤
False Vocal Fold Constriction: It is possible to observe the false vocal folds (ventricular folds) during phonation, including any constriction or irregular vibration patterns that may affect voice quality.
5. Vertical Laryngeal Movements 🎶
Pitch Change: Endoscopy enables the observation of vocal fold lengthening and vertical laryngeal movements that occur with pitch changes.
6. Vocal Tremor and Spasm 🎶
Vocal Tremor: Endoscopy can reveal vocal tremors, which often manifest as irregular vibrations of the vocal folds.
Vocal Fold Spasm: It also helps detect vocal fold spasms, where the vocal folds may involuntarily tighten, affecting voice production.
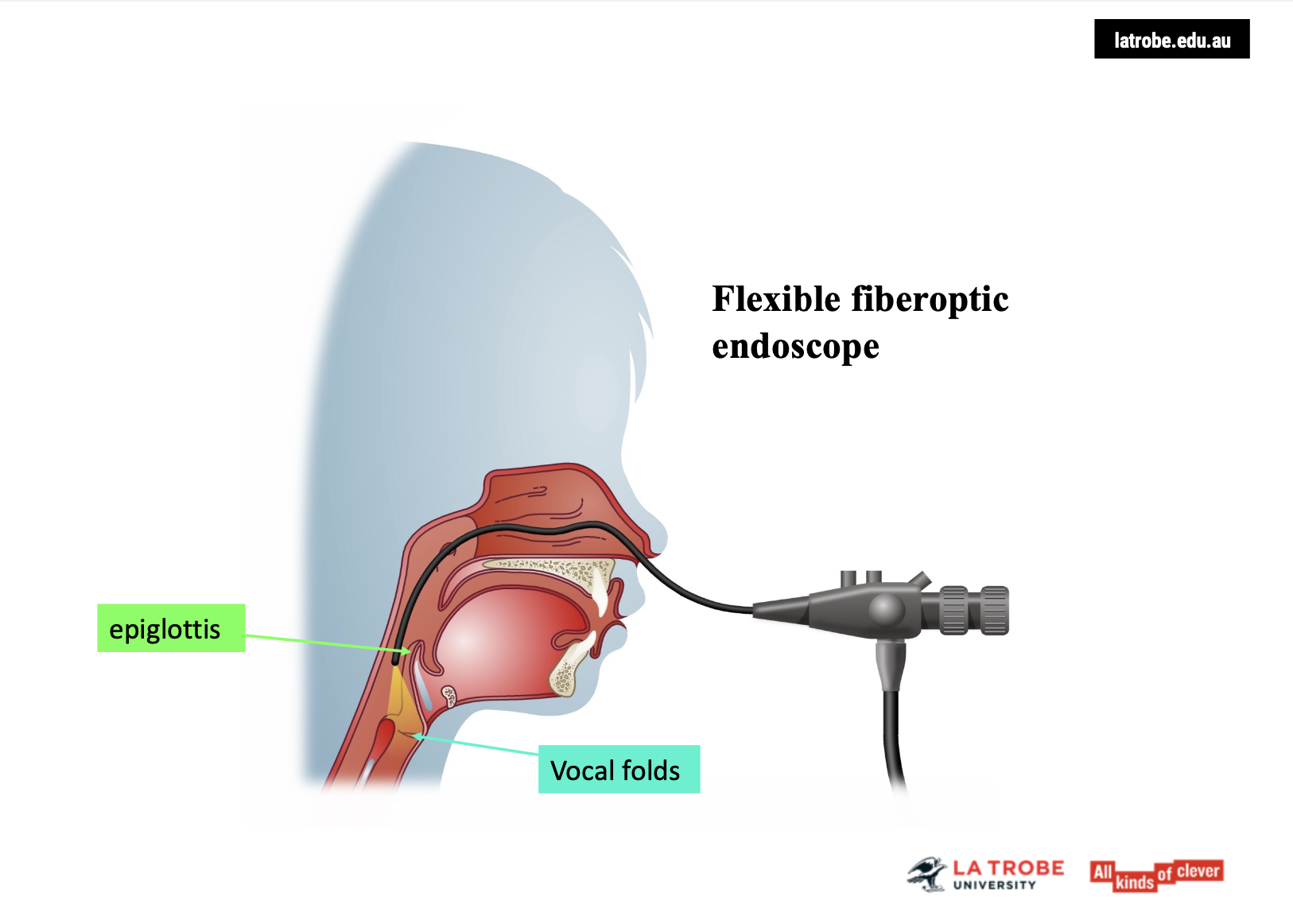
Flexible Fibre Optic Endoscope Overview
Insertion Process: The endoscope is inserted through the nostrils, navigating across the nasal floor into the nasopharynx. It can be advanced further towards the epiglottis and even deeper into the vocal tract, such as in trans-nasal esophagoscopy.
Patient Comfort: This procedure can be uncomfortable for the patient, particularly if the scope is inserted deeply.
Visualisation 👀
View of the Larynx: The endoscope provides a bird’s-eye view of the entire laryngeal area and surrounding structures, offering valuable insight into vocal fold movement, glottal closure, and any potential abnormalities.
Flexible fibre optic endoscopy is an important tool for visualising the larynx and assessing laryngeal function, especially in patients with vocal pathologies.
Endoscopy with Continuous Light vs. Stroboscopy
Continuous Light Endoscopy:
Provides a view of the larynx but does not capture the individual cycles of vocal fold vibration.
Limitations:
No detailed analysis of the periodicity or regularity of vocal fold vibrations.
Amplitude of vibration, phase of vibration, and mucosal wave cannot be clearly assessed.
Glottal closure can be difficult to judge accurately under continuous light.
Stroboscopy:
This technique uses a pulsed light to illuminate the vocal folds, allowing for a slow-motion view of the vibration cycles, which can be analysed in terms of regularity, amplitude, and mucosal wave.
Key Takeaway: Stroboscopy is crucial for a more precise analysis of vocal fold function, especially for observing vibration characteristics and glottal closure, which are not visible with continuous light endoscopy.
Stroboscopic Light and Vocal Fold Vibration
How Stroboscopic Light Works:
Rapid Pulses: Stroboscope emits pulses of light that flash at a rate either set by the examiner or controlled by the fundamental frequency of the client's voice.
Detection: The electroglottogram (EGG), using a contact microphone placed over the thyroid cartilage, detects the vocal fold vibration rate.
Synchronization:
When the pulse frequency of the strobe light matches the vocal fold vibration rate, the vocal folds appear to be motionless (unless there is irregular vibration).
If the emitted strobe frequency is slower than the vocal fold vibration rate (usually 2 Hz slower), an optical illusion occurs, making the vocal folds appear to vibrate in slow motion.
Key Takeaway: Stroboscopic light provides an optical slow-motion effect to observe vocal fold vibrations, helping to assess vocal fold function, including irregularities and vibration patterns that cannot be seen under normal light.

Stroboscopic Imaging and Its Role in Diagnosing Vocal Pathologies
Image Composition:
Composite Picture: The stroboscopic light doesn’t show a single cycle of vibration in full. Instead, it presents still images taken from multiple cycles, which are combined by the retina and brain into a continuous series.
Missed Vibratory Activity: As these images are snapshots from different cycles, some vibratory details are missed because it doesn't capture the entire vibration phase.
Diagnostic Value:
Despite this, stroboscopy provides invaluable insights into vocal pathologies.
It helps in detecting conditions that affect:
Mucosal wave
Phase symmetry
Glottal closure
These issues, often related to vocal pathologies like cysts, sulcus, and scars, are difficult to spot under normal light.
Identification of Subtle Vibratory Issues:
Stroboscopy is essential for identifying subtle vibratory impairments that might otherwise be misdiagnosed as muscle tension dysphonia (MTD).
Key Takeaway: While stroboscopic images don’t capture full vibration cycles, they are crucial for diagnosing vocal fold pathologies that affect vibratory patterns, offering insights that normal light cannot reveal.
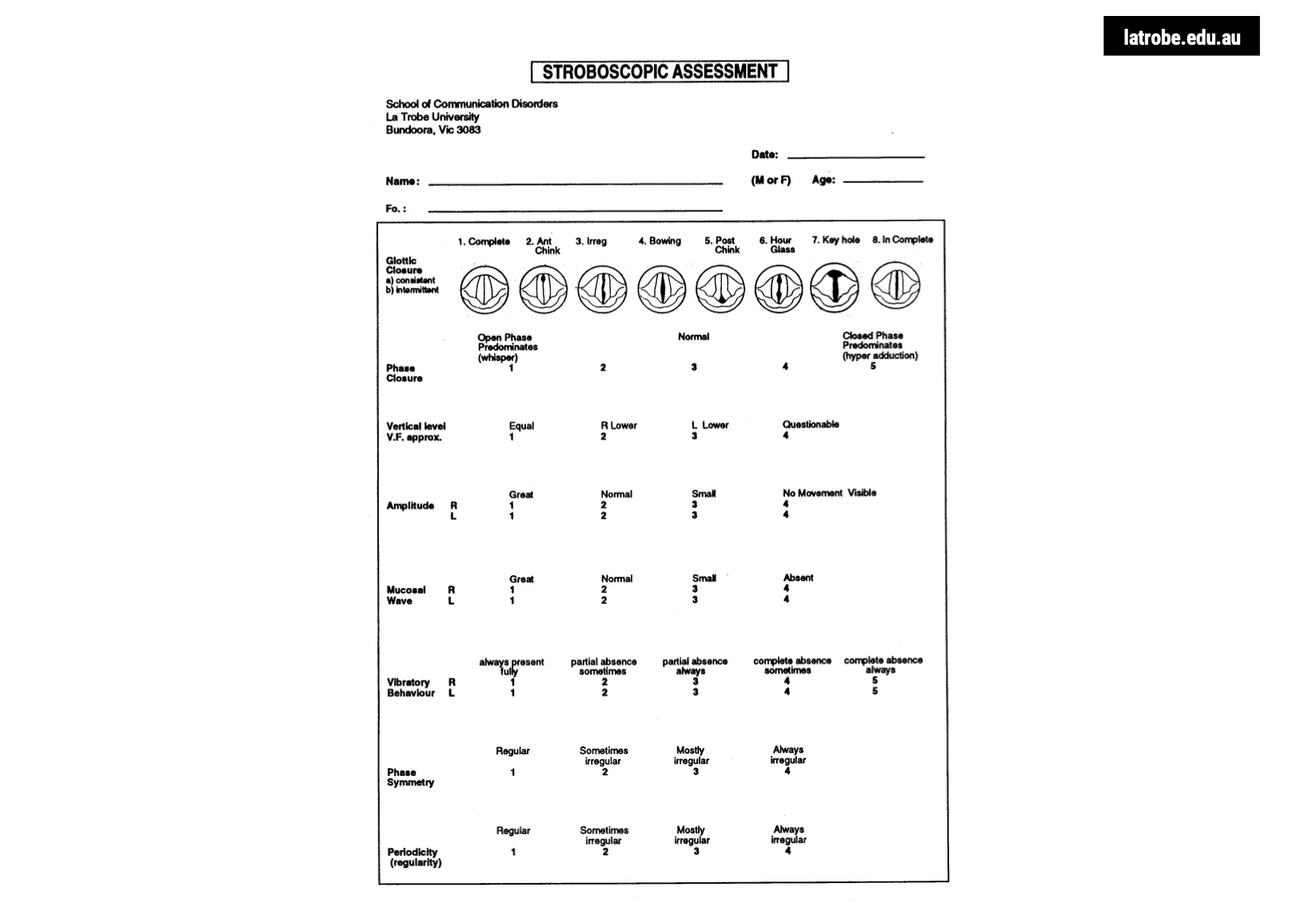
Key Features Assessed Under Stroboscopic Light
Glottal Configuration:
Refers to the pattern of glottal closure during vocal fold vibration.
Helps determine if the vocal folds come together evenly and symmetrically during phonation.
Mucosal Wave:
The wave-like lateral motion of the vocal fold cover.
Involves the epithelium and superficial layer of the lamina propria.
Provides insights into the health and movement of the vocal folds during vibration.
Amplitude of Vibration:
Refers to the extent of medial-lateral excursion of the vocal folds during vibration.
Measures how far the vocal folds move toward and away from each other.
Phase Symmetry:
Assesses how synchronously the vocal folds vibrate.
The folds should ideally be mirror images of each other.
The open and closed phases should be in a 1:1 ratio, meaning both vocal folds open and close at the same time.
Summary: Stroboscopic evaluation focuses on glottal configuration, mucosal wave, amplitude of vibration, and phase symmetry, providing detailed insights into the functioning and health of the vocal folds during phonation.
Additional Features Assessed Under Stroboscopic Light
Periodicity:
Refers to the regularity of the vocal fold vibratory cycles.
When the strobe light is synchronized with the vocal fold vibration:
Normal vibration: Vocal folds appear stationary.
Irregular vibration (e.g., rough voices): Vocal folds appear to flutter.
Phase Closure (Open/Closed Quotient):
The proportion of the open and closed phases during vocal fold vibration.
Ideal ratio: 40–60% open phase and closed phase, or a 1:1 ratio.
Vibratory Behaviour:
Observes the presence or absence of vibration in the entire vocal fold or specific segments.
Important for detecting localized issues or vibration abnormalities in the vocal folds.
Summary: Stroboscopic light allows assessment of periodicity, phase closure, and vibratory behaviour, providing valuable information on the regularity, symmetry, and functionality of vocal fold vibrations.