PSYC 444 - Final - Hypnosis and dissociation
1/176
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
177 Terms
hypnotizability
responsiveness to suggestions usually administered in a hypnotic context (stable, life-long ability)
What does NOT correlate with hypnotizabilty?
- Personality measures: no relation was ever found with traditional personality measure (nothing with Big 5, MMPI, etc)
- Intelligence, gender, age, race (past teenage years, there is not relation with age)
- Acquiescence (compliance), gullibility, social desirability: no relation
- Attention, perception, and cognitive styles: Yes but only small to medium correlations
Cognitive shift: Cognitive styles positively related to hypnotizability
1) Absorption - mixed results (seems related to testing context, i.e. higher in hypnosis study than unrelated)
2) Demand hypothesis - demands of experimental context affects response to scale
3) Construct Ambiguity hypothesis - scale questions subject to different interpretations, intensity (related) vs. freq. (unrelated)
4) Imagery and image thinking - not related to hypnotizability per se but needed for responses (needed for hypnotic suggestion so necessary but not sufficient)
5) fantasy proneness, paranormal experiences, dream control, dissociation
Absorption
open to absorbing and self-altering experience,
Parts of the attentional system
Alert, orient, select
alerting
refers to a change in a person's internal state in preparation for perceiving a stimulus
orienting
directs the person's point of reference to sensory objects
Selecting
choosing among conflicting actions
Areas of the Frontal Lobe
Lateral prefrontal cortex, ventromedial PFC and anterior cingulate
- all three subcategories are part of a massive network that links the brain's motor, perceptual and limbic regions
Direct measures of attentional processes
automaticity: attentional processes that are fast and require minimal attentional resources
Examples of automaticity
1) Greater stroop interference priming
2) Faster processing at the level of frontal loves (ERPs - Event related protential)
3) Superior performance on explicit memory tasks (conscious recall)
4) Lower working memory capacity and process
5) Greater optimizing of attentional strategies: > automaticity
6) More vulnerability to memory distortions and memory creations
High hypnotizables seem to process info differently than lows
Stroop Effect for hypnotizability
Highs show more interference than low hypnotizable.
- effect varies when strategy involved e.g. aware of proportion of incongruent trials, post hypnotic suggestion
Social-cognitive shift: Can measures of beliefs, attitudes, expectations and motivation be related?
1) Beliefs +
2) Expectations +
3) Motivation +
4) Attitudes +
Correlate positively with hypnotizability and with each other
Do cognitive and socio-cognitive factors change?
Immune to change
Genetics of hypnotizability: Twins
Correlation of .63 for Monozygotic (MZ) twins & .08 for dizygotic (DZ) twins
vs.
Another study: MZ = .52, DZ = .18
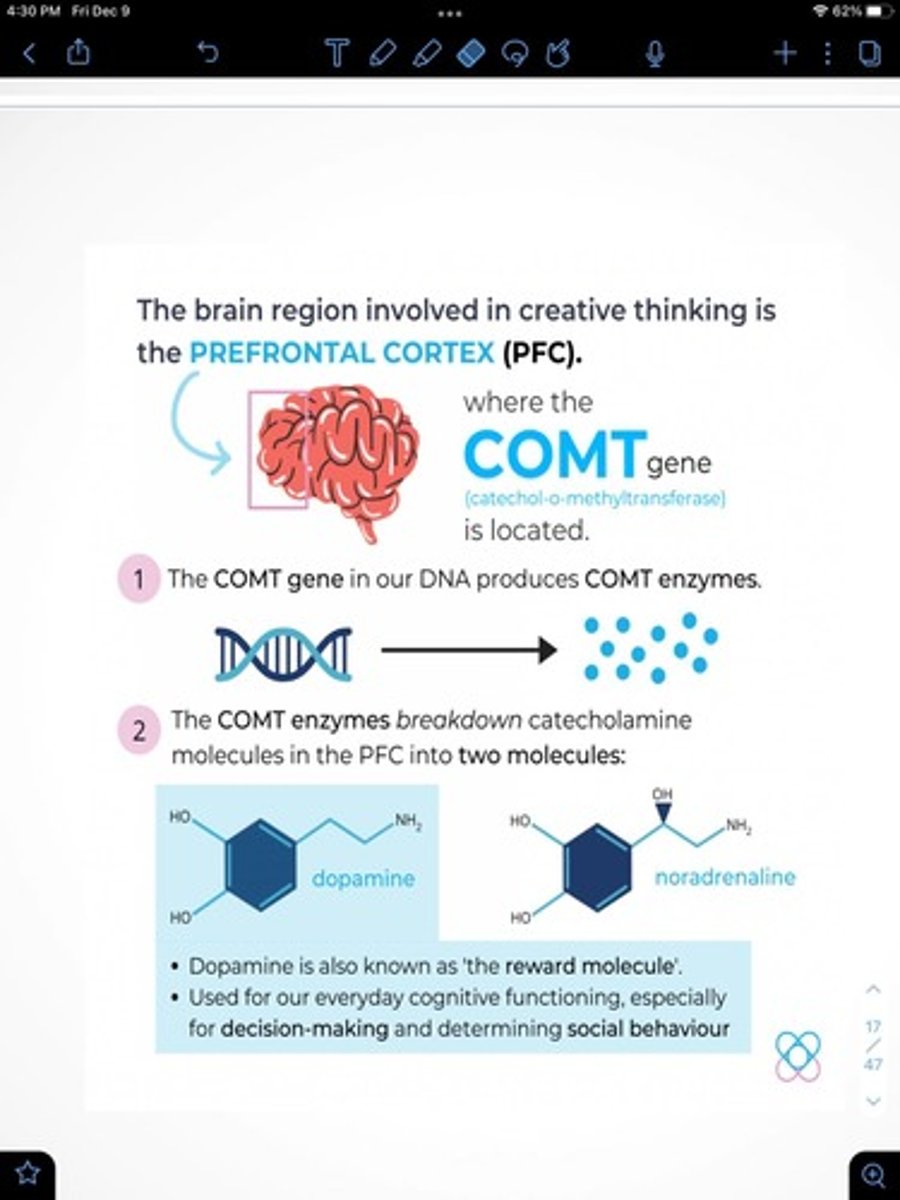
COMT gene
- influences performance on prefrontal executive cognition and working memory tasks
- would relate to hypnotizability through its role in executive functions
Executive function role in hypnotizability
Outside of the hypnotic context, highs people process words more automatically than do lows
- However: implies a significant deviation in baseline efficiency of the executive attention network in highs by increasing errors of attention
What are the 3 main competing explanations for how hypnosis works?
1) Dissociation theories (state hypothesis): Your conscious state is altered
2) Social cognitive theories (non-state hypothesis): Your conscious state is not altered
3) Synergistic model (integrative) (non-state hypothesis): Your conscious state is not altered
"State" theme hypnosis theories:
1) Neo-dissociation theory (Ernest Hilgard)
2) Dissociated control theory (Bowers and Woody)
"Social" theme hypnosis theories:
1) Social-cognitive theory (Nick Spanos)
2) Socio-cognitive theory (Kirsch and Lynn)
Integrative hypnosis theories:
1) Synergistic-model (Laurence: Lynn, Laurence & Kirsch)
4 Facts of state theories of hypnosis:
1) Hypnotic inductions produce an altered state of consciousness
2) Hypnotic 'trace' is associated with an altered state of brain function
3) Responses to hypnotic suggestions are a result of special processes such as dissociation or other altered states of consciousness
4) Hypnotizability is stable over long periods
4 Facts of non-state theories of hypnosis:
1) Participants respond to suggestion almost as well without hypnosis
2) Participants in hypnosis experiments are actively engaged (you're part of the process)
3) Responses to suggestions are a product of normal psychological processes such as attitudes, expectancies and motivation
4) Suggestibility can be modified with drugs or psychological procedures
Dissociation theories of hypnosis
hypnosis = altered state of consciousness
Neo-dissociation theory (Ernest Hilgard) view on cognition
cognition involves multiple systems of control which are not all conscious at the same time (access things not in person's awareness)
- systems controlled and motivated by central "executive ego" (executive functioning = control system)
Neo-dissociation theory: Hierarchy of control
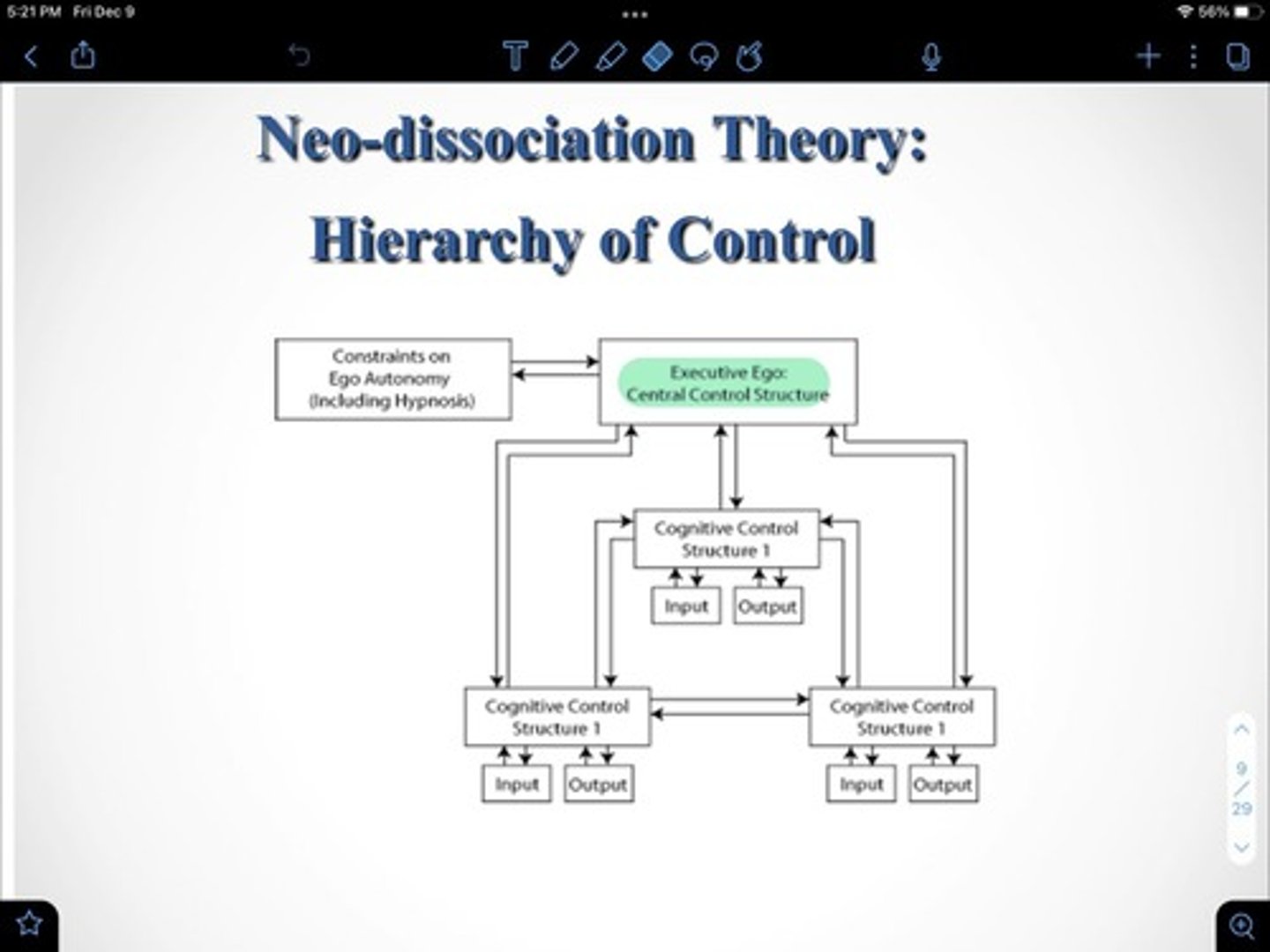
Neo dissociation theory structure
Hypnosis dissociates (or isolates) the Executive Ego, so that part of it is under direct control of hypnotic instructions
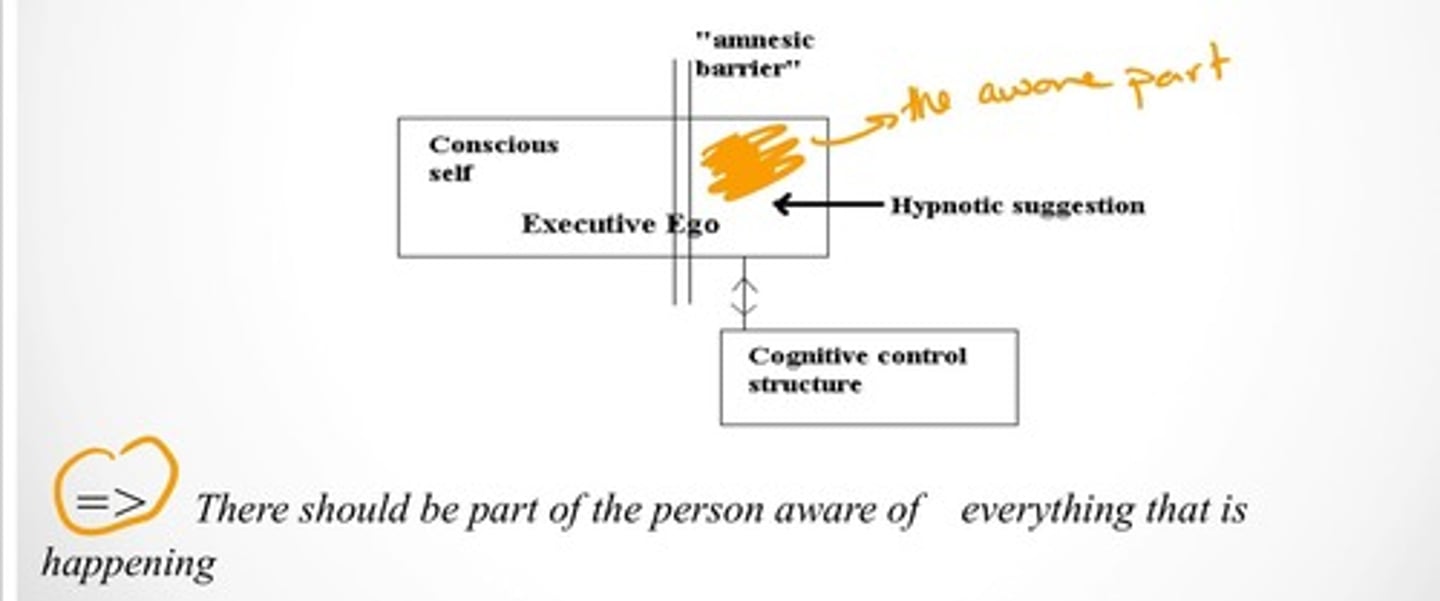
Neo-dissociation theory: Arguments
1) during hypnosis the hypnotist gains control of the executive ego, and therefore has access to the various subsidiary control systems (which P may not have conscious access to)
2) hypnosis creates a division of awareness in which a person simultaneously experiences two streams of consciousness that are cut off from one another
3) One stream responds to the hypnotists suggestions while the second stream remains a hidden observer of everything that occurs
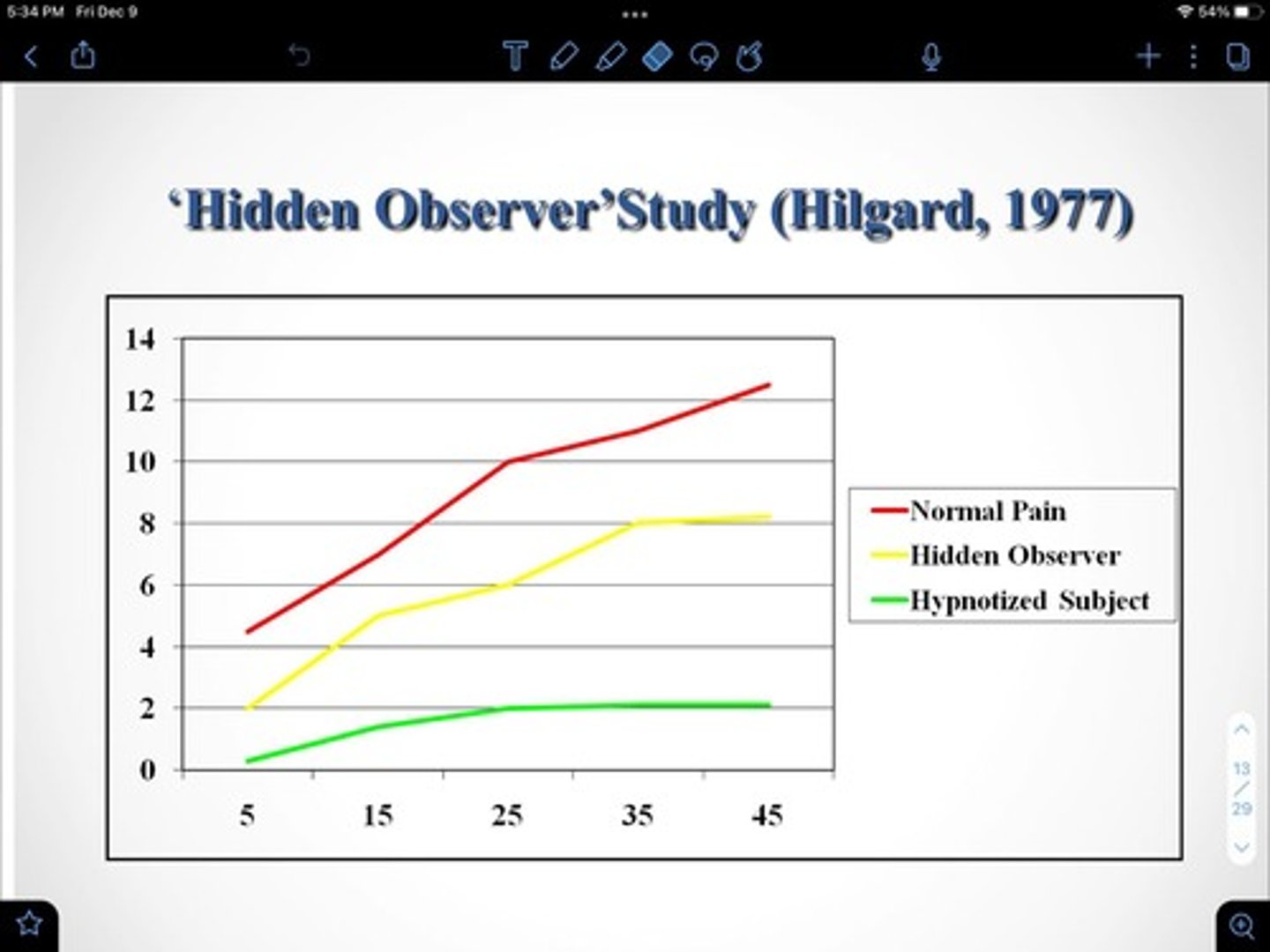
hidden observer study and phenomenon:
Hilgard: Ps hypnotized, told they won't feel pain, put arm in ice cold water for 45 seconds and report pain level
"Perhaps there is another part of you that is more aware than your hypnotized part. If so, would that part of you report the amount of pain"
Hidden observer argument:
dissociation between streams of consciousness accounts for why hypnosis appears to produce involuntary actions: invoke the feeling of involuntariness
- the subject intentionally carries out the actions, but only the 'hidden observer' is aware of this
Problems with neo-hypnosis/hidden observer theory:
1) Only 50% of highs demonstrate the H.O. effect
2) simulators (lows told to imitate hypnosis) also gave evidence of H.Os: Simulators pick up their cues from the hypnotist
dissociated control theory
Hypnotic induction weakens the Executive Ego (a state theory) so that the control structures are directly affected by hypnotic suggestions
- no amnesic split, no part the hypnotist controls
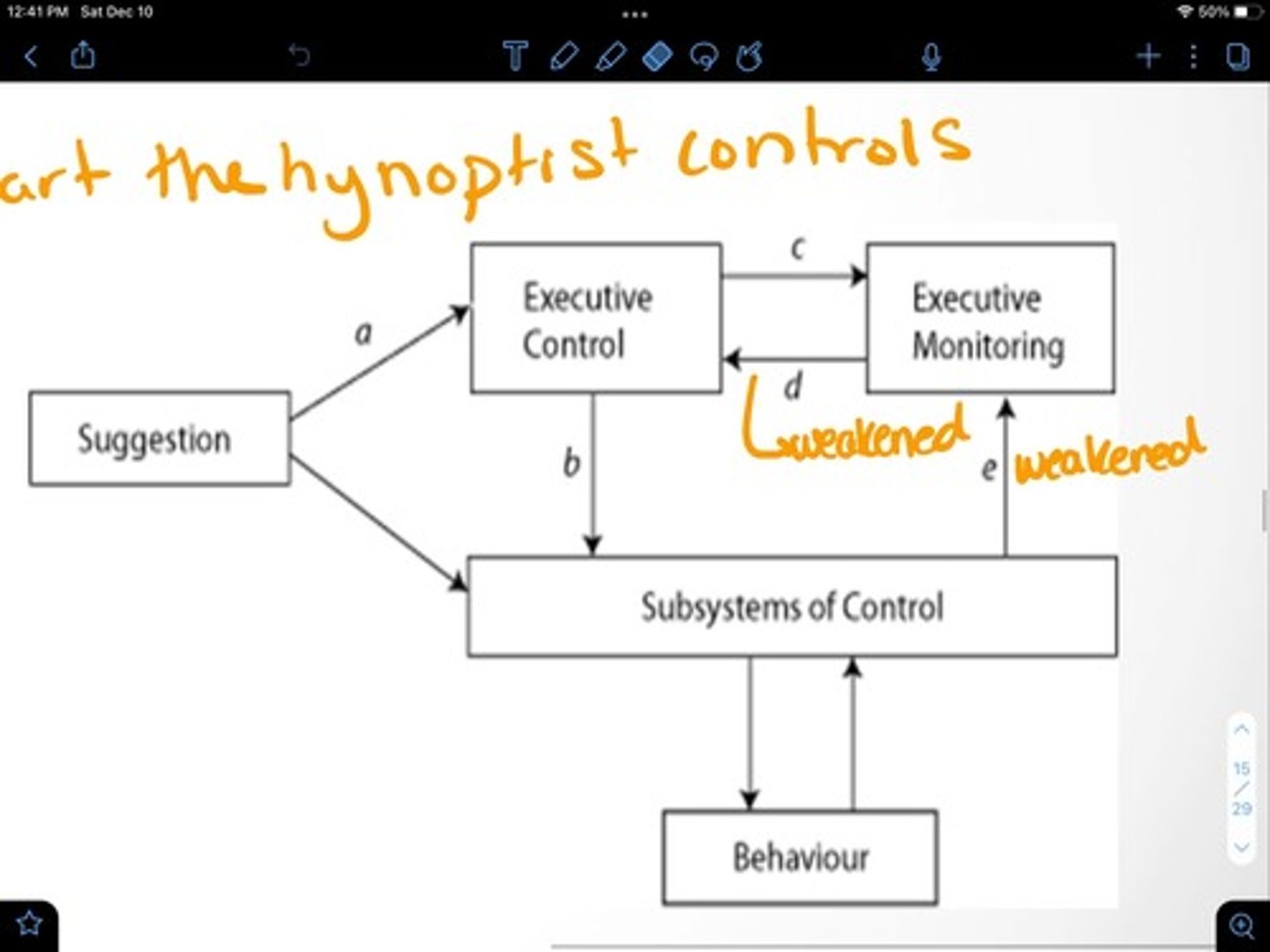
What pathways are weakened in the dissociated control theory and what does this result in?
Path A: suggestion to executive control
Path B: Executive control to subsystems of control
Path D: Executive monitoring to executive control
Path E: Subsystems of control to Executive monitoring
= the person's sense of agency is weakened
Why is the dissociated control theory good?
1) Testable
2) Emphasizes executive functions, memory and attention
How do contemporary state theories view hypnotizability?
1) As a malfunction or as hypnosis triggering some form of malfunction
2) Have a hard time explaining hypnotizability: stable over time, normal ability, unrelated to hypnosis
What do social cognitive theories of hypnosis argue?
1) deny that hypnosis produces an altered state of consciousness, no distinct state of hypnosis
2) hypnotic experiences result from belief and expectations of ppl motivated to take on the role of "hypnotized" (which explains the small increase in responsiveness)
3) Subjects develop a perpetual set (What are you walking in with?): a readiness to respond to suggestions and to perceive hypnotic experiences as real and involuntary
What is missing from social cognitive theories?
What if someone is motivated/believes/etc but hypnosis doesn't work?
What proof is there for this theory?
Orne (1959): subjects told that arm levitation is a common feature of a trance
- 55% spontaneously raised their arm, none of the control group did this
What do social cognitive theories NOT claim?
That people are pretending or faking to be hypnotized: expectations can influence behaviour without conscious awareness
How is hypnosis a social influence situation according to social cognitive theorists?
1) We mis-attribute our actions to hypnosis: not the social demands per se or even ourselves
= feeling of involuntariness
= NO special state of hypnosis, nor any special process involved in hypnotic responding
2) Subjects act as they believe a good subject should perform
- subjects are not just complying, role enactment = believed in imagining (believe in it while in it)
What intention do the subjects walk in with according to socio-cognitive theories?
They intend that their cognitive control structures will be triggered by the hypnotist's suggestions
- once this intention is formed: some actions will be triggered without executive ego involvement
How do socio-cognitive theories explain feelings of volition?
they are just interpretations and attributions
- when control structures are triggered by hypnotist, even where there is involvement by the executive ego, the effects are attributed as involuntary, in line with expectations
What is the synergistic model by Laurence?
1) a Neuro-cognitive contextual model
2) Emphasis on hypnotizability, hypnosis as context
3) Behaviours and experiences are shaped by contexts and abilities
4) Involuntariness is a consequence of automaticity of processing, and expectations and beliefs
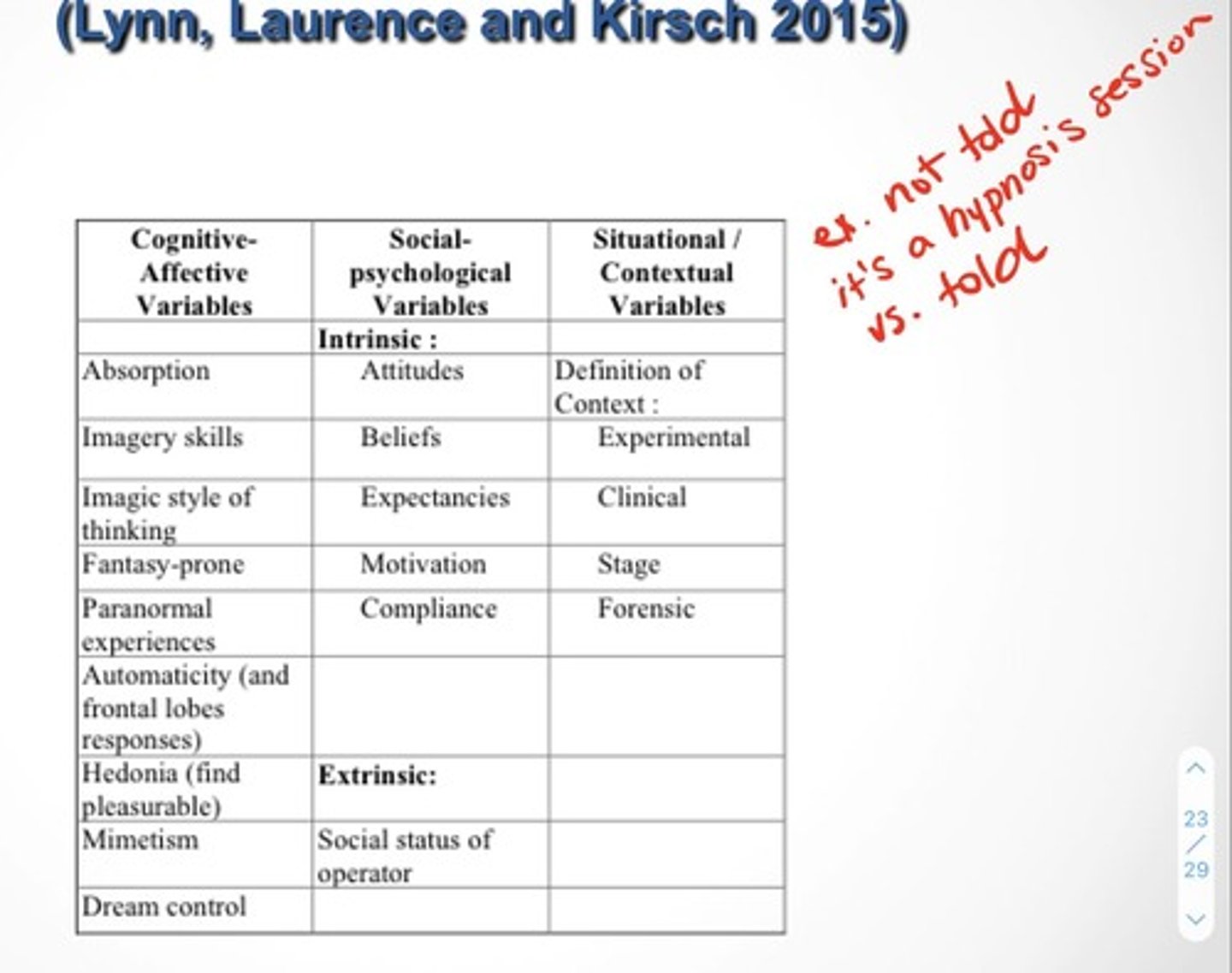
Variables for the synergistic Model (integrative model)
Explain the role of simulators and what they do:
1) lows asked to fool the hypnotist into believing they are highs
2) Simulator's behaviour = demand characteristics while
Reals' behaviour = demand characteristics + geniune hypnotic effects
3) Simulators will overplay their role compared to real subjects, they respond in line with that which they believe a good hypnotic subject would do
How do dissociation theories explain hypnotized ppl subjectively believing their actions to be involuntary?
Divided streams of consciousness
How do Social Cognitive theories explain hypnotized ppl subjectively believing their actions to be involuntary?
attribute it to subject's expectation as to what effect hypnosis will have on them
How do Synergistic Model theories explain hypnotized ppl subjectively believing their actions to be involuntary?
both abilities and context play an interactive role
What is the most promising theory for hypnosis?
Synergistic
What is dissociation?
The splitting or separation of "normal" mental, emotional and/or behavioral functioning
- Awareness of self, memory (past/present), perception of reality (time, yourself, world), and attention shifts, splits or is compromised
Is dissociation normal?
Yes, normal and/or pathological: continuum of ability to dissociate
- starts normal can become pathological
What are the current assumptions about dissociation?
Capability, Non-Uniqueness, Diversification, Ownership, Accessibility
What is the capability assumption about dissociation?
At least some are able to do it - likely on a continuum similar to hypnosis
What is the Non-Uniqueness assumption about dissociation?
It's similar to other human capacities - likely shares features of other cognitive capacities (e.g. absorption), can share components, not stand alone
What is the diversification assumption about dissociation?
It comes in a variety of forms, affects broad range of states (current, dispositional), along various continua: frequency, completeness, reversibility, degree of functional isolation (like DID alters: no memory of the part coming forward)
What is the ownership assumption about dissociation?
What is dissociated from someone is always their own states
e.g. sensory, cognitive, volition (the angry part of you is you for ex.)
What is the accessibility assumption about dissociation?
Theoretically reversible i.e. potentially knowable in conscious awareness (bc its part of you)
What psychopathologies can dissociation manifest in and effect several functions of?
1) Affect regulation (depression, social anxiety disorder)
2) Disruption of identity (Splitting - failure to integrate positive and negative aspects, or Fragmentation of self
3) Auto-hypnotic (Trance, time distortions)
4) Behaviour (Poor impulse control, self harm)
5) Memory (Fugue, amnesia)
6) Revitalization of past trauma (flashbacks, hallucinations)
What is fragmentation of self?
When one is developing their personality from infancy (personality - normally becomes cohesive, all connected) but development can be compromised so then personality is disconnected
What is fugue?
lose all memory of selves, no memory of identity, leave and start a new life elsewhere
What did Janet think caused dissociation?
The environment - constitution interacts with extreme environment causing cognitive/affective disintegration
What did Freud think caused dissociation?
The environment - Environment interacts with psychological processes, trauma results in defense to manage anxiety and avoid re-traumatization.
What is the contemporary explanation for dissociation?
Defense pattern in entrenched and becomes automatic and uncontrolled response to stress (situation brings about the need to use defense mechanism, doesn't cause them)
What is the object relations explanation for dissociation?
trauma necessitates premature maturation of 'false' self used in survival of trauma
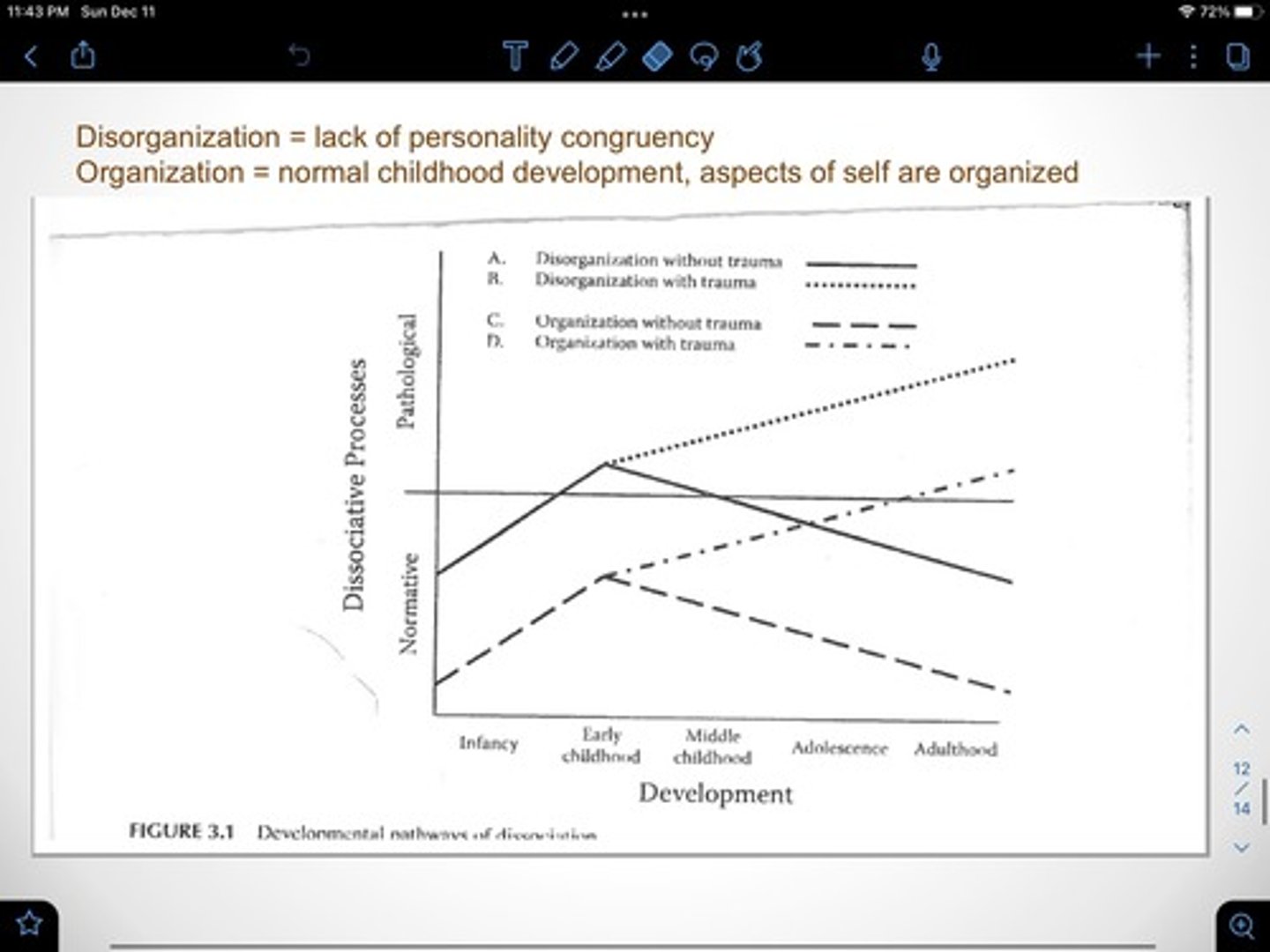
What is normal use of dissociation?
- can be seen as part of the normative process of developing self (ex. fantasy proneness)
- normal decline of use with age (from child to adult - difference in cognitive ability to recognize discontinuity in behaviour and/or sense of awareness
- if continues into adulthood, might be a sign of pathological use
How does the self develop?
Series of qualitative re-organizations:
- earlier adaptation is framework, is transformed by later adaptations
- Older adaptations change to newer forms via integration of various domains of functioning related to developmental stage/issues
- Positive adaptation - flexible, integration of all domains (behavioural, emotional, cognitive, etc)
What is needed for proper development of self?
1) Organization: inner organization of attitudes, feelings, meaning, etc, through different adaptions and integrations
2) Emotional regulation (core of early development)
3) Caregivers for emotional regulation: primary relationship, requires limit setting, monitoring, etc. Availability = important
4) Range of emotional experience (pos and neg): caregiver promotes closeness in realtionships
What are relational distortions?
- Emotions fail to achieve purpose
- Emotions are activated but expression is blocked/punished
- distortion of emotional regulation due to distorted care
Psychopathological distortions
Represents distortion of core self - adaptive processes can result in healthy integration vs. dissociation
What happens if development occurs without integration?
- children with higher capabilities may use dissociation as defence strategy
- If trauma, distortion of care, etc occurs = development proceeds using alternate path
- dissociation may be used as substitute to organize experiences
How does the self develop in middle childhood/adolescence without integration?
Cognitive development may aid in adaptive integration, or have normal development using dissociation (ex. adolescence use of persona i.e. friend, teacher, etc)
or, pathological development of more severe forms of dissociation
- cog dev = more complex = more complex dissociative expressions
Possible developmental pathways with dissociation
What are the dimensions of dissociation?
1) Type
2) Level
3) Timing
What is the Type dimension of dissociation?
Quality of experience ex. amnesia (pathological) vs. absorption normal
What is the Level dimension of dissociation?
A continuum
absorption --------> DID
What is the Timing dimension of dissociation?
Peritraumatic vs. postraumatic: disorder is not that dissociation is experienced as protective response, but that severe dissociation continues in absence of such conditions
What is a peritraumatic dissociation?
Dissociation at the time of trauma
- may predispose to PTSD
- Generally regarded as normal (ex. OOB experience, temporary decrease in pain awareness, Shock: perceptual disturbances, brief amnesia after trauma)
How is normal vs. pathological dissociation related to defense?
Dissociation can be seen as process operating through allocation of attention :
- Absorption (focus on one experience, other aspects blocked/avoided, not processed = poor recall)
- vs. Pathological dissociation (experience more processed, blocked by defense)
How is normal vs. pathological dissociation related to frequency?
how different are the frequency of experiences as compared to base rates
How is normal vs. pathological dissociation related to purpose?
Relates to purpose of dissociation in situation - function can be healthy, or high-jacked to serve unhealthy purpose
ex. numbing normal in combat, not normal if not in crisis.
What is self-alienation?
Need for survival includes the need for the sense of self to psychologically distance from ongoing trauma
- Disowning the 'wounded child'/'Bad child'
- Disowning the trauma by disowning traumatized part of us (parts w/ shame, anger, vengeful, needy, etc)
Why is disowning the 'wounded child'/'bad child' survival?
1) Preserves self-esteem
2) Preserves ability to carry on as the 'good child' e.g. go to school, homework, etc.
Why is it adaptive to disown vulnerability?
1) Disown needs that can't be met
2) Disown feeling that are 'unacceptable'
3) Alienation and fragmentation helps maintain attachment to family, at the expense of self-acceptance
4) Due to parental failure of mirroring, environment negates internalizing a coherent sense of self
What is the secure attachment style?
As a child:
1) can express their feelings, needs, etc.
2) Easily soothed by caregiver
As an adult:
1) Feel good about themselves, accept self 'as is'
2) Understand that mistakes get made, theyre not perfect, etc.
What is the ambivalent/preoccupied attachment style?
As a child:
1) anxiously clings to caregiver and cannot be soothed
2) Separation interferes with feeling safe
As an adult:
1) So blended with vulnerable parts that they can't be there for themselves
2) Need someone else to there for them
What is the avoidant/dismissive attachment style?
As a child:
1) Precociously autonomous but disconnected from self and others
As an adult:
1) Disconnected from emotions and don't acknowledge them
2) Not connected to self
What is the disorganized attachment style?
As a child:
1) Two opposite drives: one to be close to caregiver, and one to defend against caregiver
2) Associated with abuse and neglect
As an adult:
1) Cannot accept selves
2) Locked in internal conflict between self-acceptance and self-rejection
How does self-alienation manifest?
1) Self-esteem: Self-loathing, judge self, attack self esteem, can't incorporate info that goes against this
2) Terminal ambivalence: stuck, can't make decisions or commit, self-sabotage
3) Numbness: intellectualization, no emotion
4) Emotional: Overwhelmed, emotional outbursts, no self-soothing
5) Self-destructive behaviour: Acting out, addictions, eating disorders
6) Paradoxical behaviour: contradictory behaviour, mood shifts
7) Regressive or aggressive behaviour without ownership
8) Dissociative disorders
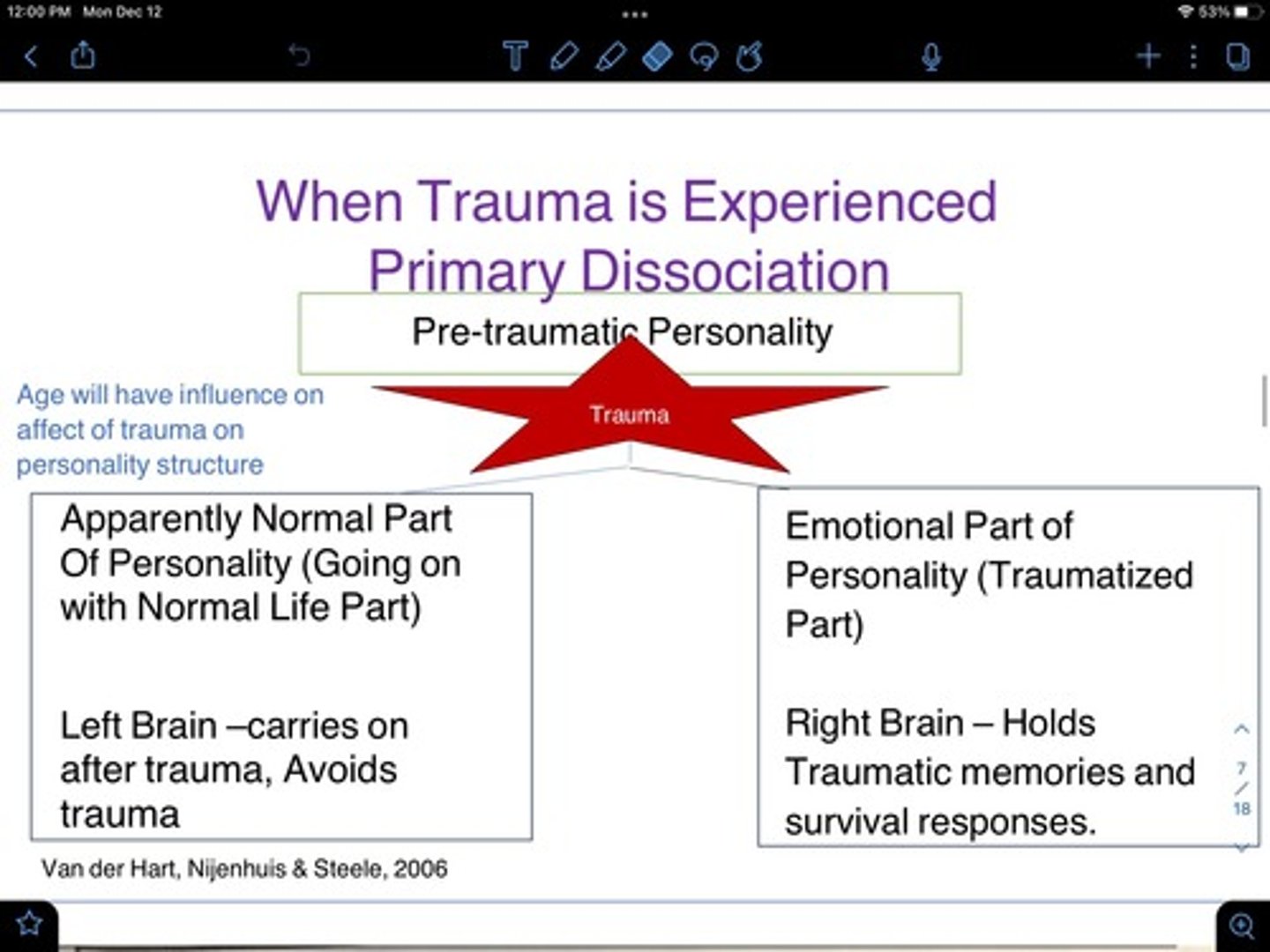
What is the left brain responsible for?
1) Reasons, plans, organizes, learns and makes meaning of new experiences.
2) Verbal, analytical
3) Manages right brain emotions, impulses
4) Carries on with daily life no matter what happens
What is the right brain responsible for?
1) Creative, playful, etc
2) Survival: holds emotional self
3) Lacks words but reads body language and facial expressions
What happens to the left and right brain after trauma?
Primary Dissociation
What does the sympathetic nervous system do when we are in danger?
Fight-flight response:
- body experiences an adrenaline rush to increase HR and breathing, causes muscles to tense & provides energy that prepares us for action, the thinking brain shuts down to increase RT
What does the parasympathetic nervous system do when we are in danger?
Freeze-submit response:
- chemical slow HR and breathing which = physical collapse, exhaustion, weakness, shaking, nausea/diarrhea & the survival response of freezing and total submission or playing dead
What happens when we remember a traumatic event?
1) Memory centers in the frontal lobes shut down and we get overwhelmed by feelings and impulses instead of recalling events
2) limbic system activates amygdala which responds like we're in danger now
3) reptilian brain reacts instinctively to amygadala alarm: increase HR, stop breathing/hyperventilate, speed up or shut down, muscles tense
What happens to left and right brain with multiple compound trauma?
Secondary Dissociation:
1) More avoidance and more preoccupation
2) Emotional part becomes compartmentalized: subparts evolve reflecting different survival strategies needed in a dangerous world
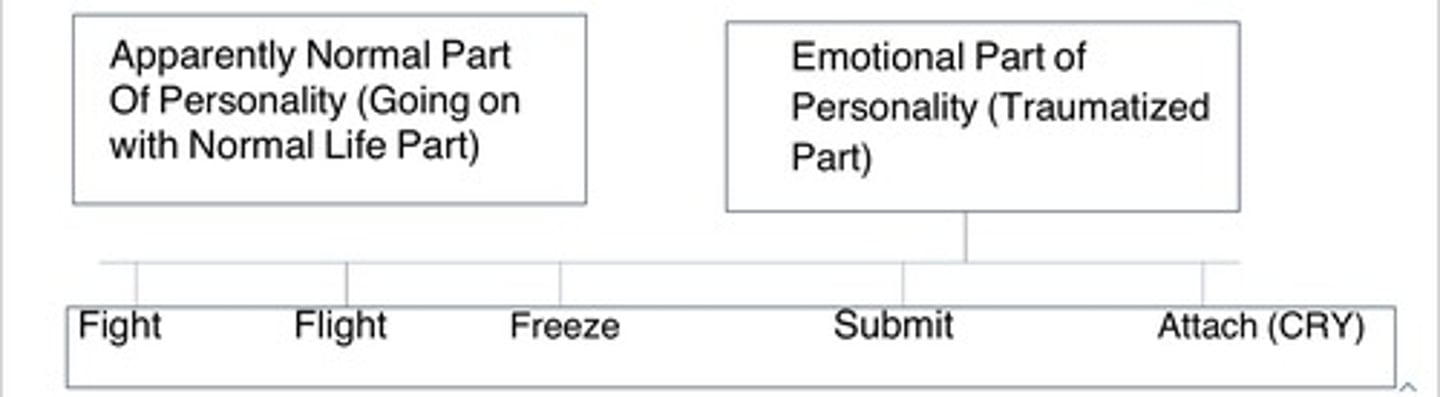
How does the fight defense strategy manifest?
Protector, anger, mistrust, hypervigilance, resistance, self-harm, suicidality
How does the flight defense strategy manifest?
Distancer, addictive behaviour to turn off body
How does the freeze defense strategy manifest?
Terrified, Triggers other parts to respond with alarm
How does the submit defense strategy manifest?
Ashamed, shame, self-loathing, passivity, feeds helplessness/hopelessness
How does the attach defense strategy manifest?
Needy, uses vulnerability and desperate help seeking to elicit protection