wilhelm n/v
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
which drugs may cause acute n/v
- chemo
- opioids
- digoxin (remember this also caused diarrhea!)
- abx
- anticholinergics (symp)
potential etiologies of acute n/v
- anything GI related (gastroenteritis, obstruction, surgery...etc)
- vestibular disorders
- metabolic (diabetic ketoacidosis, uremia)
- drugs (chemo, opioids, digoxin, abx, anticholinergics)
etiologies of chronic n/v
- obstruction (PUD, ulcer, carcinoma)
- motility disorders
- pregnancy
- neuro
stimuli: drugs, uremia, ketoacidosis [toxins that cross BBB]
mech/receptors:
CTZ: DA, 5HT3, NK1
(same as GI visceral afferents)
stimuli: obstruction, gastroparesis, visceral pain
mech/receptors:
GI visceral afferents: DA, 5HT3, NK1
(same as CTZ)
stimuli: motion sickness, vestibular inflammation [inner ear]
mech/receptors:
vestibular apparatus: muscarinic, NE, H1
stimuli: emotion, sight, smell, taste
mech/receptors:
cortical structures
-> use benzos. no direct receptor
summarize which receptors are targets for which n/v stimuli
drugs, ketoacidosis, uremia (BBB)-> DA, 5HT3, NK1
obstruction, gastroparesis, visceral pain-> DA, 5HT3, NK1
motion sickness, vestib, ear-> muscarinic, NE, H1
emotions, sight, smell-> cortical (use benzos)
fluid and electrolyte disturbances such as metabolic ______osis, _____natremia, and _______kalemia are common complications of vomiting
alkalosis
hyponatremia
hypokalemia
why would we want to use non-pharm methods for the tx of n/v in the following
pregnancy:
post operative:
motion sickness:
pregnancy: avoid teratogenic effects
post operative: avoid additive sedation
motion sickness: avoid sedation since moving
non-pharm diet for n/v tx
- frequent, small meals
- avoid spicy and fatty foods
- high protein snacks
- bland food, especially early morning
- starting prenatals at conception
other than diet, what other non-pharm tx are there for n/v
1. acupressure: P6 point in wrist (sea bands)
2. hypnosis/ psychotherapy
which phenothiazines are available for n/v?
moa?
prochlorperazine (Compazine)
promethazine (Phenergan)
chlorpromazine (Thorazine)
moa:
-blocks DA receptors in CTZ [so will work on drug-induced, toxins, BBB etc)
- some anticholinergic activity
what type of n/v do phenothiazines help with
blocks DA receptors so anything that affects CTZ [so will work on drug-induced, toxins, BBB etc)
phenothiazines ADEs
- sedation
- orthostatic hypotension (chlorpromazine)
- extra pyrimidal symptoms (prochlor)
- tissue necrosis and gangrene (if promethazine subQ or intra-arterially)
what can happen if promethazine is given subQ
tissue necrosis and gangrenes
what can be given to minimize EPS
diphenhydramine or benztropine (Cogentin)
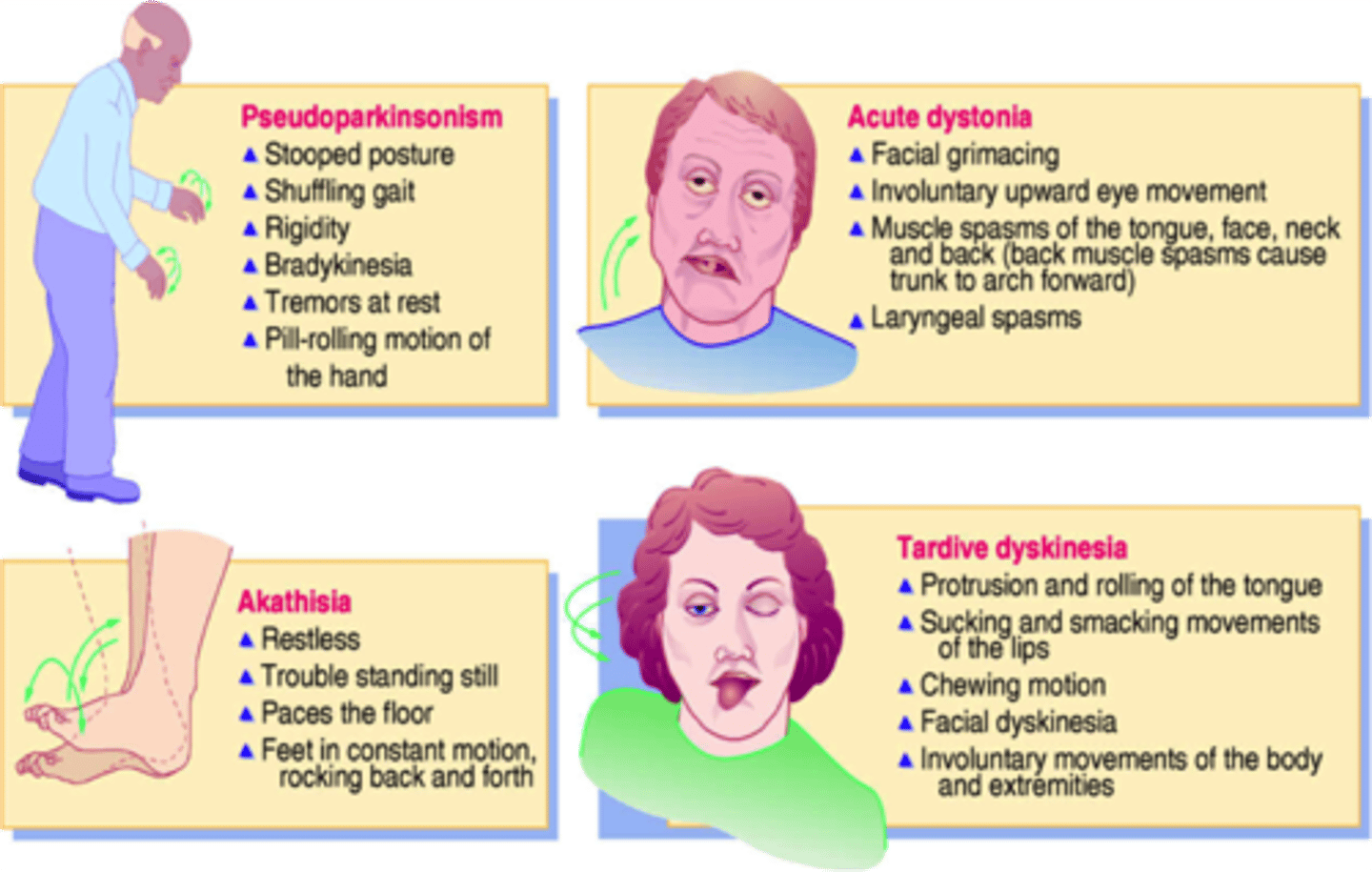
what are EPS
extra pyrmidal symptoms
1. dystonia: muscle contractions
2. tardive dyskinesia: involuntary movements; cogwheel motions (might become irreversible!!)
3. akathisia: motor restlessness/ anxiety
t/f: EPS may be a side effect of phenothiazines but are always reversible
false. tardive dyskinesia (involuntary muscle movements) seen in EPS may be irreversible
which causes of n/v respond well to antihistamines/anticholinergics
issues in inner ear/ motion sickness
remember receptors: muscarinic, NE, H1
examples of antihists/anticholinergics for n/v
moa?
diphenhydramine
meclizine
scopolamine
dimenhydrinate
hydroxyzine
MOA: CNS anticholinergic activity in VC and vestibular system
-> so for motion sickness or labyrinth induced symptoms
ADEs for antihists/ anticholinergics
drowsiness, confusion, blurred vision, dry mouth, urinary retention, tachycardia
precautions/CI for antihistamines/anticholinergics
narrow angle glaucoma
urinary retention
prostatic hypertrophy
asthma
examples of butyrophenones?
moa?
droperidol, haloperidol
MOA: block DA receptors in CNS
[so will work on CTZ: drug-induced, toxins, BBB etc]
t/f: butyrophenones such as haloperidol experience less EPS than phenothiazines such as prochlorperazine
true
what black box warning is seen with droperidol
QT prolongation
-> must have ECG before use
metoclopramide
brand:
moa:
Reglan (benzamide analog)
-blocks DA receptors in CTZ
- cholinergic activity in GI
- anti-serotonin at high doses
- prokinetic in UPPER GI (not used for constipation. used for gastroparesis)
metoclopramide ADEs
EPS, sedation!!, diarrhea, edema, HTN, hyperprolactinemia (increases milk production), impotence
metoclopramide CIs
intestinal obstruction or high risk for colonic rupture (bc not only for n/v but its also a prokinetic)
domperidone
benzamide analog/ dopamine antagonist like metoclopramide BUT
-does not cross BBB= less CNS ADRs
- not available in US
- may prolong QT interval
which n/v meds prolong QT interval
- domperidone
- droperidol
- serotonin antagonists (ondansetron)
which type of n/v are cannabinoids most often used for
chemo induced (CINV)
-moa unknown
what can prolonged use of cannabinoids for n/v lead to
cyclic vomiting syndrome
-heat may alleviate symptoms
corticosteroids for n/v
examples:
moa:
dexamethasone (Decadron)
methylprednisolone (Medrol)
moa: unknown
- inhibits PG synthesis in cortex
- decreased CNS serotonin turnover
- modulation of higher cortical pathways influencing VC
corticosteroids for n/v ADEs
short term: mood change, anxiety, insomnia, increased appetite, fluid retention, hyperglycemia, GI upset
long term: osteoporosis, cataracts, skin thinning, bruising, immunosuppression
benzodiazepines for n/v
examples:
moa:
used for?
lorazepam (Ativan), alprazolam (Xanax)
moa: unknown. suppression from higher brain to emetic center. lowers anxiety, amnesia, sedation
use: emotional triggers of N/V
benzos ADEs
sedation
prolonged amnesia
hypotension
perceptual disturbances
urinary incontinence
respiratory depression (no alcohol!!!)
serotonin antagonists for n/v
examples:
moa:
use:
"setrons"= ondansetron, granisetron, dolasetron, palonosetron
moa= block 5ht3 receptors in CTZ anddd vagal visceral fibers in GI
no anti motion sickness efficacy!!
use: CINV, PONV (chemo, post op)
5ht3 antagonists ADEs
"setrons"
mild headache, diarrhea, constipation, transient elevations in LFTs, asymptomatic ECG changes
t/f: serotonin antagonists such as ondansetron can be used for chemo, post op, and motion sickness
false.
motion sickness is muscarinic, NE, H1. no serotonin receptors
t/f: ondansetron requires ECG monitoring for pts at risk for QT changes
true
neurokinin receptor antagonists (NK1 antagonists)
examples:
moa:
uses:
aprepitant, fosaprepitant, netupitant/palonosetron, rolapitant
moa: blocks NK1 in CNS and GI
use: prevents CINV and PONV (aprepitant only)
aprepitant
moa?
use?
blocks NK1 receptors in brain
use: antiemetic for chemo (tripack) and post op (3hrs before) induced nausea and vomiting
aprepitant ADEs
- diarrhea OR constipation
- headache, dizziness
- hiccups
- transient elevation in LFTs and BUN
aprepitant DDIs
induces 2C9= warfarin, phenytoin, birth control
inhibits 3A4 (substrate)= steroids, benzos, chemo
- caution with 3a4 inhibitors and inducers
n/v in pregnancy most often occurs in the _______ trimester
first
hyperemesis gravidarum
severe nausea and vomiting in pregnancy that can cause severe dehydration in the mother and fetus (1-3%)
non pharm therapy for pregnant n/v
- modify diet
- acupressure/ acupuncture
- ginger
pharm tx for n/v in pregnancy
1. pyridoxine (B6)
2. H1 receptor antagonist= doxylamine, dimenhydrinate, meclizine, (B) diphenhydramine, hydroxyzine (C)
which of the following is the best tx approach for n/v in pregnancy
a. aprepitant
b. ondansetron
c. metoclopramide
d. Vit B6 + meclizine
d. Vit B6 + meclizine (h1 receptor antagonist)
note: for more severe NVP you can also use ondansetron, metoclopramide, prochlorperazine, corticosteroids (after 1st trimester)
if pregnant pt is not responding to B6/doxylamine, what other options are available?
ondansetron= best tolerated
metoclopramide= 2nd choice
prochlorperazine
corticosteroids (after 1st trimester)
Diclegis
brand of doxylamine/pyridoxine combo for pregnancy induced n/v
Bonjesta
doxylamine/pyridoxine indicated for nausea/vomiting in pregnancy
what is motion sickness caused by
stress in labyrinth (inner ear)
= motion, infection, neoplasm, idiopathic
receptors: muscarinic, histamine
non pharm tx for motion sickness
- minimize exposure to movement
- restrict visual activity
- distractions
- avoid alcohol, food overindulgence
- acupressure
- ginger
pharm approach for motion sickness
1. antihistamines
= diphenhydramine, dimenhydrinate, meclizine
2. anticholinergics
= scopolamine patch (for long term-> cruise_
MEDICATE PRIOR TO STIMULI!!
a pt comes in complaining of motion sickness. what would you recommend and what counseling would you give
antihistamine (diphenhydramine, dimenhydrinate, meclizine) or anticholinergic (longer time-> scopolamine patch)
- MEDICATE BEFORE YOU EXPERIENCE IT!!
what patient specific factors increase risk for post op n/v
female
motion sickness/ PONV hx
nonsmoking
use of post-op or intra-op opioids
obesity
what surgery-related factors increase risk for n/v
type= abdominal, gyne, ears nose throat
gas anesthetics= isoflurane, enflurane, NO
general anesthesia
long surgeries (>100min)
prevention for post op n/v
1. reduce risk factors
- opioid-sparing pain control
- regional, non volatile anesthesia
2. PONV prophylaxis (if 2+ risk factors OR history of PONV)
non-pharm tx for PONV
-acupressure, acustimulation
- ginger (if allowed to eat before/after surgery)
- aromatherapy (not rlllyyy proven. just take controlled breaths)
when is a pt eligible for PONV prophylaxis
1. if has 2+ risk factors:
-female
-motion sickness
-nonsmoking
-use of opioids during or after op
-obese
-ab/ears/nose/throat surgery
- volatile or non localized anesthesia
-long surgery
2. if has had PONV before
monotherapy prophylaxis options for PONV
- droperidol [qt prolongation]
- dexamethasone
- prochlorperazine [sedation risk]
- promethazine [gangrene]
- metoclopramide
- 5ht3 antagonist
(all valid options, no rank)
PONV dual therapy prophylaxis combos for higher risk pts
droperidol + 5ht3 antagonist
dexamethasone + 5ht3 antagonist
droperidol + dexamethasone
PONV triple therapy prophylaxis combo for highest risk pts
droperidol + dexamethasone + 5ht3 antagonist
what is the difference in treatment for a patient with PONV that has
1. received prophylaxis
2. has not received prophylaxis
received: choose an agent from different class
not received prophylaxis:
low dose 5ht3 antagonist
-granisetron, ondansetron, dolasetron
pt AB is going on a cruise and wants smtg for motion sickness. He has BPH, HTN, and an aspirin allergy. which is the best option
a. scopolamine patch
b. acupressure band
c. dimenhydrinate
d. aprepitant
b. acupressure band
a and c are correct mech but we dont want to give antihist/anticholinergic bc he has BPH. those will make his urination even worse. d is for NK receptor
which of the following are appropriate monitoring parameters for a pt receiving ondansetron + dexamethasone for post op n/v prophylaxis
a. hyperglycemia
b. EPS
c. ECG/EKG
d. sedation
a (diabetes and getting steroid) and c (ondansetron)
EPS-> thiazines
sedation-> antihist/anticholinergics/thiazines