MED SLP EXAM 1
0.0(0)
Studied by 20 peopleCard Sorting
1/71
Earn XP
Description and Tags
Last updated 8:15 PM on 3/14/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
1
New cards
Dental deviations include the following:
* Congenitally missing teeth
* Malrotated teeth
* Ectopic teeth (abnormally located)
* Supernumary or duplicated teeth (extra)
* Malrotated teeth
* Ectopic teeth (abnormally located)
* Supernumary or duplicated teeth (extra)
2
New cards
Malocclusions include the following:
* Overjet/overbite, often associated with Class II malocclusion (upper teeth protrude beyond lower teeth)
* Underjet/underbite, often associated with anterior crossbite or Class III malocclusion (lower teeth protrude beyond upper teeth)
* Open bite (teeth do not fully occlude)
* Lateral (buccal) crossbite (lower teeth buccal to upper teeth)
* Underjet/underbite, often associated with anterior crossbite or Class III malocclusion (lower teeth protrude beyond upper teeth)
* Open bite (teeth do not fully occlude)
* Lateral (buccal) crossbite (lower teeth buccal to upper teeth)
3
New cards
Speech and resonance assessment : Begins with an interview & a perceptual assessment
Parent concerns/observations, medical hx, diagnoses, surgical hx, dev hx, feeding hx, sleep concerns, therapy hx
4
New cards
Speech and resonance assessment: Depending on findings/results
\
\
instrumental assessment may be warranted.
5
New cards
Speech and resonance assessment: Goals of perceptual eval
* Determine dx and possible cause
* Obtain info to make recs/treatment plan
* Obtain info to make recs/treatment plan
6
New cards
Speech assessment
Single word articulation tests are not the only part for perceptual speech/VP assessments. Repetition of speech samples is fast, easy and representative.
7
New cards
Perceptual evaluation of Resonance: Need to determine TYPE of resonance
1. Normal resonance
2. Hypernasality
3. Hyponasality
4. Cul-de-Sac resonance
5. Mixed resonance
8
New cards
Perceptual evaluation of Resonance:
Determining severity
Determining severity
1. normal
2. mid
3. mild-moderate
4. moderate
5. moderate-severe
6. severe
Severity does not really matter. If the structure is abnormal, it requires treatment. What is MOST important is to determine TYPE of resonance
9
New cards
Error types for children with a history of clefts
* Obligatory
* Compensatory
* Compensatory
10
New cards
**Obligatory Errors**
* Correct placement
* Errors are just related to the structural or functional deficit
* Oral nasal fistula - get air leak through their nose
* May have high arched palate and very crowded jaws, skinny pointed maxilla – can't produce the /s/ due to lack of space
* Dental deviation malocclusion
* Can't have correction until the structure is fixed
* Hypernasality on vowels, liquids, and glides
* We do not fix them, structure is problem
* Errors are just related to the structural or functional deficit
* Oral nasal fistula - get air leak through their nose
* May have high arched palate and very crowded jaws, skinny pointed maxilla – can't produce the /s/ due to lack of space
* Dental deviation malocclusion
* Can't have correction until the structure is fixed
* Hypernasality on vowels, liquids, and glides
* We do not fix them, structure is problem
11
New cards
**Compensatory Errors (compensating)**
* errors in place of articulation or direction of airflow
* Placement is wrong ( I can't make a t k g so I through glottal stops as all stops because they can't get intra oral pressure all goes out nose )
* Build up and release air pressure in VF
* Air on intra oral pressure sounds
* Can't make intra oral pressure
* Can't match what they hear
* Hearing and cog challenges
* Try to change into obligatory
* Replace sounds with stops
* I can't do sound so I put it somewhere else and compensate
* Placement is wrong ( I can't make a t k g so I through glottal stops as all stops because they can't get intra oral pressure all goes out nose )
* Build up and release air pressure in VF
* Air on intra oral pressure sounds
* Can't make intra oral pressure
* Can't match what they hear
* Hearing and cog challenges
* Try to change into obligatory
* Replace sounds with stops
* I can't do sound so I put it somewhere else and compensate
12
New cards
General feeding considerations for infants with cleft lip and/or cleft palate: Mechanics of extraction
* Munching pattern/compression provides compression of nipple (bottle/breast)
* Not effective for efficient extraction
* Suction = negative pressure
* This allows for effective milk transfer from the bottle or breast
* Requires sealed oral cavity
* They cannot do this if they have a cleft lip/palate ^
* Unable to seal oral cavity
* Inability to create negative pressure (the suction force)
* Inefficiency w/ milk AKA extraction
* Poor extraction → reduced total intake + increased energy expenditure → failure to thrive
* Not effective for efficient extraction
* Suction = negative pressure
* This allows for effective milk transfer from the bottle or breast
* Requires sealed oral cavity
* They cannot do this if they have a cleft lip/palate ^
* Unable to seal oral cavity
* Inability to create negative pressure (the suction force)
* Inefficiency w/ milk AKA extraction
* Poor extraction → reduced total intake + increased energy expenditure → failure to thrive
13
New cards
General feeding considerations for infants with cleft lip and/or cleft palate: What you should do
* Feeding optimization
* Specialized bottles/parent education
* Positioning
* Caloric management
* Reflux management
* Specialized bottles/parent education
* Positioning
* Caloric management
* Reflux management
14
New cards
General feeding considerations for infants with cleft lip and/or cleft palate: Role for SLP
* typically evaluates and treats early feeding/swallowing issues
* Educate nurses, caretakers/parents regarding feeding recommendations including feeding position, appropriate nurses/nipples etc.
* Recommend further diagnostic testing as needed (MBS, FEES, etc.)
* role of an SLP from prenatal to adolescence in the care of children with clefts/craniofacial diagnosis
* Educate nurses, caretakers/parents regarding feeding recommendations including feeding position, appropriate nurses/nipples etc.
* Recommend further diagnostic testing as needed (MBS, FEES, etc.)
* role of an SLP from prenatal to adolescence in the care of children with clefts/craniofacial diagnosis
15
New cards
**Appropriate roles for SLPs include, but are not limited to:**
•counseling persons with cleft lip and palate and their families regarding communication- and feeding/swallowing-related issues and providing education aimed at preventing further complications relating to these conditions;
•educating other professionals about the needs of persons with cleft lip and palate and the role of SLPs in diagnosis and management;
•screening individuals who present with cleft lip and palate; determining the need for further assessment and/or referral for other services;
•conducting a comprehensive, culturally and linguistically appropriate assessment of speech, language, resonance, voice, or feeding problem associated with cleft lip and palate;
•diagnosing speech, language, resonance, voice, or feeding disorders associated with cleft lip and palate;
•referring to other professionals to rule out co-occurring conditions, determine etiology, and facilitate access to comprehensive services;
•making decisions about the management of speech, language, resonance, voice, and feeding/swallowing problems related to cleft lip and palate;
•developing treatment plans, providing treatment, documenting progress, and determining appropriate dismissal criteria;
•consulting and collaborating with other professionals, family members, caregivers, and others to facilitate program development and to provide supervision, evaluation, and/or expert testimony, as appropriate;
•remaining informed of research in the area of cleft lip and palate and helping advance the knowledge base related to the nature and treatment of these conditions;
•advocating for individuals with cleft lip and palate and their families at the local, state, and national levels
•serving as an integral member of an interdisciplinary team working with individuals who have cleft lip and palate and their families/caregivers; and
•providing quality control and risk management.
•educating other professionals about the needs of persons with cleft lip and palate and the role of SLPs in diagnosis and management;
•screening individuals who present with cleft lip and palate; determining the need for further assessment and/or referral for other services;
•conducting a comprehensive, culturally and linguistically appropriate assessment of speech, language, resonance, voice, or feeding problem associated with cleft lip and palate;
•diagnosing speech, language, resonance, voice, or feeding disorders associated with cleft lip and palate;
•referring to other professionals to rule out co-occurring conditions, determine etiology, and facilitate access to comprehensive services;
•making decisions about the management of speech, language, resonance, voice, and feeding/swallowing problems related to cleft lip and palate;
•developing treatment plans, providing treatment, documenting progress, and determining appropriate dismissal criteria;
•consulting and collaborating with other professionals, family members, caregivers, and others to facilitate program development and to provide supervision, evaluation, and/or expert testimony, as appropriate;
•remaining informed of research in the area of cleft lip and palate and helping advance the knowledge base related to the nature and treatment of these conditions;
•advocating for individuals with cleft lip and palate and their families at the local, state, and national levels
•serving as an integral member of an interdisciplinary team working with individuals who have cleft lip and palate and their families/caregivers; and
•providing quality control and risk management.
16
New cards
What is a cleft?
* Abnormal opening in an anatomical structure
* Usually a congenital malformation due to abnormal fusion during fetal development
* Usually a congenital malformation due to abnormal fusion during fetal development
17
New cards
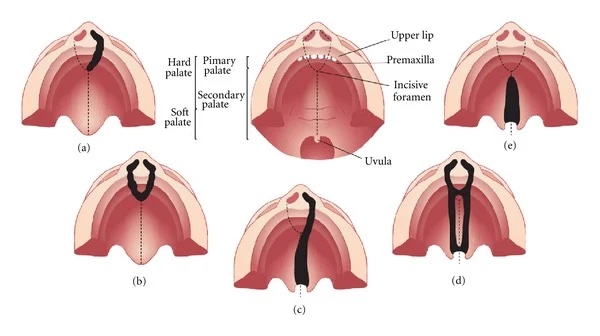
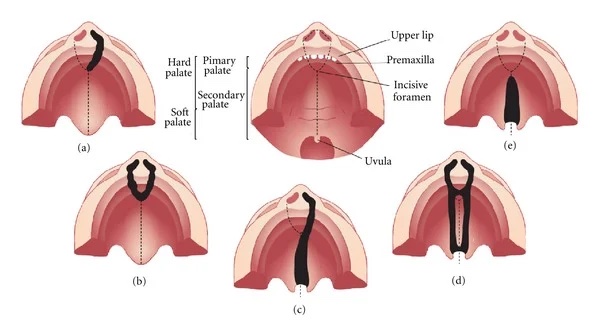
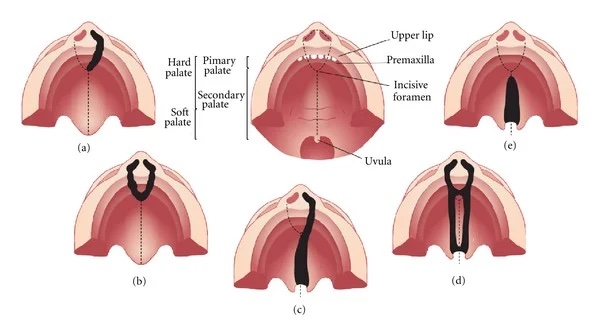
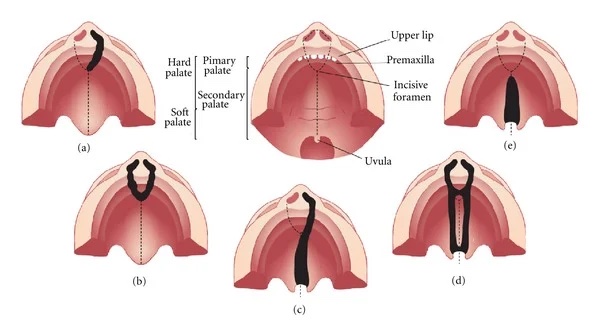
What are the different types of Cleft Palates
* unilateral
* bilateral
* complete
* incomplete
* bilateral
* complete
* incomplete
18
New cards
unilateral cleft
one sided cleft
19
New cards
bilateral cleft
both sides have cleft
20
New cards
complete cleft
cleft that extends through the lip, nostril sill, alveolar ridge, & incisive foramen
21
New cards
Incomplete cleft
* cleft that does not extend all the way to incisive foramen
* microform is one type
* microform is one type
22
New cards
different types of atypical resonance
* **Hypernasality**
* **Hyponasality**
* **Cul-de-Sac resonance**
* **Mixed resonance**
* **Hyponasality**
* **Cul-de-Sac resonance**
* **Mixed resonance**
23
New cards
**Hypernasality:**
Too much sound production in the nasal cavity while producing n, m, and ng sounds. May cause a low volume due to the reduction of sound through the oral cavity and absorption of sound in the pharyngeal/nasal cavities
24
New cards
**Causes of Hypernasality:**
* Velopharyngeal opening
* Submucous cleft palate
* A large oronasal fistula
* Phoneme specific hypernasality due to mislearning
* Submucous cleft palate
* A large oronasal fistula
* Phoneme specific hypernasality due to mislearning
25
New cards
**Hyponasality**:
A reduced amount of nasal resonance when speaking, specifically on n, m, and ng sounds.
26
New cards
**Causes of Hyponasality**:
* Caused by blockage in nasopharynx or nasal cavity due to:
* allergies
* common cold
* adenoid hypertrophy
* hypertrophic tonsils
* allergies
* common cold
* adenoid hypertrophy
* hypertrophic tonsils
27
New cards
**Cul-de-Sac resonance**:
occurs when sound resonates in a cavity (oral, nasal, or pharyngeal) but is “trapped” and cannot exit because of an obstruction (sound is muffled)
* Acoustic energy is blocked from exiting at a cavity’s normal outlet
* Sound cannot be released, so it stays in the cavity and is muffled
* Sound is absorbed by soft tissues
* Low volume
* Acoustic energy is blocked from exiting at a cavity’s normal outlet
* Sound cannot be released, so it stays in the cavity and is muffled
* Sound is absorbed by soft tissues
* Low volume
28
New cards
**Causes of Cul-de-Sac resonance**:
* microstomia (small mouth)
* ‘mumbling’: speaking without opening the mouth completely
* ‘mumbling’: speaking without opening the mouth completely
29
New cards
**Mixed resonance:**
elements of inconsistent hypernasality, hyponasality, and/or cul-de-sac resonance in connected speech
30
New cards
Failure of fusion during fetal development caused by:
* Environmental teratogens
* Mechanical factors
* Chromosomal abnormalities
* Genetic syndromes
* Mechanical factors
* Chromosomal abnormalities
* Genetic syndromes
31
New cards
Environmental teratogens: __**Teratogen**__
* Chemical agents that can interfere with embryonic development, causing a malformation
32
New cards
Environmental teratogens: Environment
lead, radiation, pollution
33
New cards
Environmental teratogens: Drugs and ingested substances
* phenytoin (Dilantin), valium, corticosteroids, smoking, alcohol
34
New cards
Environmental teratogens: Viruses
* rubella, influenza
35
New cards
Environmental teratogens: __**Maternal nutrition**__
nutritional deficiencies or obesity with diabetes
36
New cards
Environmental teratogens: __**Physical interference**__
Crowling in utero that restricts mandibular growth
37
New cards
Week 4-9 of Embryonic development
* primary palate formation
* frontonasal prominence (FNP)- forms forehead, nose dorsum, and apex
* nasal placodes develop later bilaterally, pushed medially
* paired maxillary prominences- form upper cheek and upper lip
* paired mandibular prominences- form lower cheek, chin and lower lip
* frontonasal prominence (FNP)- forms forehead, nose dorsum, and apex
* nasal placodes develop later bilaterally, pushed medially
* paired maxillary prominences- form upper cheek and upper lip
* paired mandibular prominences- form lower cheek, chin and lower lip
38
New cards
Week 4 of Embryonic development
pharyngeal arch (come out of crest cells) formation: first pharyngeal arch contributes mandible and maxilla
39
New cards
Week 7 of Embryonic development
primary palate formation: lip, maxillary processes and frontonasal prominence (nose)
40
New cards
Week 9 of Embryonic development
* secondary palate
* fusion occurs in the human embryo in week 9 of gestation
* this requires the early palatal shelves growth, elevation, and fusion
* many fusion events are occuring during this period between each palatal shelf, to the primary palate, and also to the nasal septum
* fusion occurs in the human embryo in week 9 of gestation
* this requires the early palatal shelves growth, elevation, and fusion
* many fusion events are occuring during this period between each palatal shelf, to the primary palate, and also to the nasal septum
41
New cards
__**Sequence of development**__
•Before the palate forms, the tongue is in a **superior/posterior (up and back)** position in the nasopharynx
•Palatal shelves of the maxilla are in a **vertical** position on each side of the tongue
•Mandible migrates **down & forward**
•Tongue drops **down & forward** with the mandible growth
•Palatal shelves move from **vertical to horizontal** position, starting with the incisive foramen and moving backward
•The median palatal suture closes from the incisive foramen to the end of the maxilla
•The velum is fused in **midline** toward the uvula
•The oral surface forms **before** the nasal surface of the hard palate and velum
•Palatal shelves of the maxilla are in a **vertical** position on each side of the tongue
•Mandible migrates **down & forward**
•Tongue drops **down & forward** with the mandible growth
•Palatal shelves move from **vertical to horizontal** position, starting with the incisive foramen and moving backward
•The median palatal suture closes from the incisive foramen to the end of the maxilla
•The velum is fused in **midline** toward the uvula
•The oral surface forms **before** the nasal surface of the hard palate and velum
42
New cards
Vital Signs: Body Temperature
measures body temperature
43
New cards
Vital Signs: Pulse Rate
measures the number or heart beats per minute
44
New cards
Vital Signs: Respiration rate
measures the number or breaths per minute
45
New cards
Vital Signs: Blood pressure
Is not considered a vital sign, but is often measured along with the vital signs. This measures the force on the walls of your arteries
46
New cards
Vital Signs: SPO2: Oxygen Level
Measures the amount of oxygen in ones blood
47
New cards
**Nasogastric tube**
* Placed for those who cannot eat by mouth
* Reasons can vary
* We don’t place them, but we work with many patients across the lifespan that have them
* Feeds the stomach directly
* Feedings can be:
* continuous (drips a small amount into the stomach all day)
* Bolus (entire amount given over 30 minutes)
* Reasons can vary
* We don’t place them, but we work with many patients across the lifespan that have them
* Feeds the stomach directly
* Feedings can be:
* continuous (drips a small amount into the stomach all day)
* Bolus (entire amount given over 30 minutes)
48
New cards
**ND tubes**
similar to NG-tubes, but they go through the stomach and end in the first portion of the small intestine (duodenum)
49
New cards
**Nasojejunal Tube**
* Nose through stomach and into the jejunum of small intestine (further than ND)
* Can’t do bolus or more meal-like feeding
* Can’t do bolus or more meal-like feeding
50
New cards
**Gastronomy tube**
* Usually more permanent that “n” tubes
* Directly into the stomach
* Directly into the stomach
51
New cards
**GJ tube**
* Tube into the stomach is the G tube
* The J portion is the jejunostomy tube going into the jejunum
* The J portion is the jejunostomy tube going into the jejunum
52
New cards
**TPN**
* way to provide nutrients by bypassing digestive system
* feeding intravenously (through a vein)
* feeding intravenously (through a vein)
53
New cards
Red blood cell count (RBC):
The blood’s ability to carry O2 and Nutrientst hrough the body. Reduction in red blood cell populations and hemoglobin transport may occur due to reduced production or due to early death or loss of red blood cells, as is often seen in gastrointestinal (GI) bleeds
54
New cards
Hematocrit (HCT):
Percentage of red blood cells in total blood volume
55
New cards
Hemoglobin (Hgb):
Percentage of red blood cells in total volume of blood Hemoglobin attached to and transported by the red blood cells is responsible for transporting oxygen molecules throughout all parts of the organism Measures the blood’s capacity to carry oxygen. Can indicate blood loss
56
New cards
Contact
* Prevent transmission of infectious agents that are spread by direct or indirect contact with the patient or the patient’s environment
* Also used when a wound is draining, incontinence or other bodily discharge
* Also used when a wound is draining, incontinence or other bodily discharge
57
New cards
Droplet
To protect from droplets that are infected and produced from an individual during coughing, sneezing, talking or certain procedures such as suctioning.
58
New cards
Airborne
Used for patients infected with illness that are transmitted via the airborne route
59
New cards
general importance of an SLP's understanding of lab values and why we should care
* Help to determine a patient’s overall health
* Used for screening (1)
* Give information about medical stability of a patient
* Used to assess readiness for mobility interventions (2)
* Important in clinical decision-making
* Increased number of patients with complex care needs
* Used for screening (1)
* Give information about medical stability of a patient
* Used to assess readiness for mobility interventions (2)
* Important in clinical decision-making
* Increased number of patients with complex care needs
60
New cards
Different levels of student to fully autonomous doctor.
Med student, intern, resident, fellow, attending
61
New cards
ICU
there are different ICUs for different things e.g., C(V)ICU, NICU, TICU
62
New cards
Stepdown
* people usually go here when they leave the ICU
* Transitional floor, also known as intermediate care, telemetry or tele
* Transitional floor, also known as intermediate care, telemetry or tele
63
New cards
General Floor
* Sometimes referred to “the floor(s)” when talking about leaving ICU and being “transferred to the floor”
* Can still be dx specific care (on the floor under GI attending, on the floor under cardiology attending)
* Can still be dx specific care (on the floor under GI attending, on the floor under cardiology attending)
64
New cards
Observation
we don’t feel comfortable sending you home but you're not too sick to be admitted. They monitor to see if you get worse enough to be admitted or if you get better to leave
65
New cards
define and understand the different code statuses
Full Code
* Patient/family wants aggressive,
life-sustaining measures
* CPR (ACLS/BLS), intubation,
medications
DNR/DNI
Comfort measures only
* CMO or “Comfort care”
* Patient/family wants aggressive,
life-sustaining measures
* CPR (ACLS/BLS), intubation,
medications
DNR/DNI
Comfort measures only
* CMO or “Comfort care”
66
New cards
Chronic
develops gradually, lasts for extended period of time (months-years); may worsen
67
New cards
Acute
develops suddenly, lasts for fairly short time
68
New cards
Degenerative
Worsens gradually over time
69
New cards
how SLPS positively contribute to patients care in acute care/medical settings
* Swallowing treatment and assessments
* Voice treatment and assessment
* Counseling related to comm disorders
* Voice treatment and assessment
* Counseling related to comm disorders
70
New cards
parts of a chart (where to find relevant information)
* order
* History and physical
* Lab and diagnostics
* Vitals signs
* Medications
* Reports
* At the top there is usually alerts
* History and physical
* Lab and diagnostics
* Vitals signs
* Medications
* Reports
* At the top there is usually alerts
71
New cards
Causes of VPI
* History of cleft palate: 20-30% have VPI despite surgery
* Submucous cleft palate (overt/occult): anterior orientation of the levator veli palatini muscles
* Deep pharynx: PPW sits on cervical spine/cranial base anomalies cause deep pharynx; velum may be normal but can’t reach PPW d/t depth
* Adenoid atrophy: begins at age 6, can increase the depth of the pharynx (risk is greatest w/ hx of cleft or SMCP)
* Irregular adenoids: (marked indentation/protrusion) prevents a tight seal causing nasal emission
If a child has **moderate to severe** resonance issues and they have surgery, YOU MUST WAIT FOR SURGERY to clear you for compensatory strategies. VPI, no speech until CLEARANCE
* Submucous cleft palate (overt/occult): anterior orientation of the levator veli palatini muscles
* Deep pharynx: PPW sits on cervical spine/cranial base anomalies cause deep pharynx; velum may be normal but can’t reach PPW d/t depth
* Adenoid atrophy: begins at age 6, can increase the depth of the pharynx (risk is greatest w/ hx of cleft or SMCP)
* Irregular adenoids: (marked indentation/protrusion) prevents a tight seal causing nasal emission
If a child has **moderate to severe** resonance issues and they have surgery, YOU MUST WAIT FOR SURGERY to clear you for compensatory strategies. VPI, no speech until CLEARANCE
72
New cards
if a child has a mod to serve VPI
* they need surgery, pin port of the soft palate to pharyngeal wall
* can not start targeting them until the surgeon clears it for us
* can not start targeting them until the surgeon clears it for us