Looks like no one added any tags here yet for you.
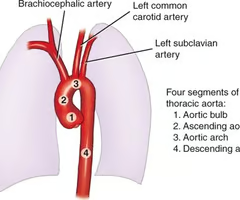
aortic root - root of valsalva
starts at level of aortic valve until sinotubular junction
ascending aorta
starts at level of sinotubular junction and ends at origin of brachiocephalic artery
aortic arch
starts at origin of brachiocephalic until just after left subclavian artery
descending aorta
starts after the origin of left subclavian artery and the diaphragm
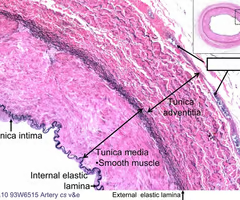
internal elastic lamina - layer that separates intima and media
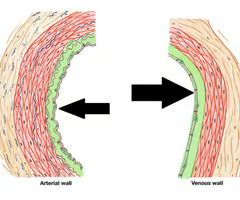
tunica intima - inner
tunica media - middle
tunica adventitia - outer
layer of endothelial cells
subendothelial layer = collagen and elastic fibres
separated from tunica media by internal elastic lamina
smooth muscle cells
secrete elastin in form of sheets/lamellae
thin connective tissue layer
collagen and elastic fibres
collagen prevents elastic tubes from stretching beyond their physiological limit during systole
hypertension
age
diabetes
hypercholesterolaemia
smoking
family history
male
stroke
MI
peripheral vascular disease
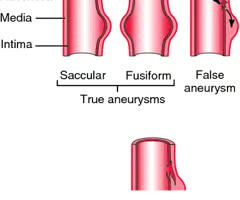
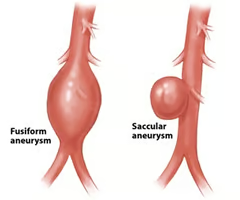
aneurysm
true aneurysm
fusiform
saccular
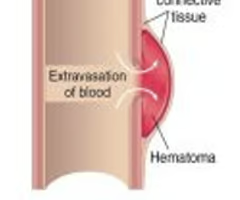
false aneurysm
weakness and dilation of vessel wall
involves all 3 layers
saccular one side - looks like a little sac
fusiform both sides
hypertension
atherosclerosis
smoking
bicuspid aortic valve
collagen abnormalities - MARFANS
infection
trauma
trauma
iatrogenic
inflammation - endocarditis with septal emboli
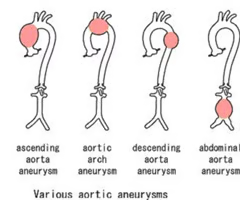
ascending aorta aneurysm
aortic arch aneurysm
descending aorta aneurysm
abdominal aorta aneurysm
mostly asymptomatic
but can have symptoms
SOB - associated aortic regurgitation
dysphagia and hoarseness
back pain
symptoms of dissection
palpable mass
sharp sudden pain radiating to back between shoulder blades
hypotension
CXR - widened mediastinum
echo - assess aortic root size and aortic valve
CT angiogram of aorta - diagnostic tool
MRI - diagnostic and follow up
tear in the inner wall of the aorta (media)
blood forces walls apart
can be acute which is a medical emergency
can be chronic dissection
hypertension
atherosclerosis
marfans
bicuspid aortic valve
trauma
cystic medial necrosis
replacement of media layer with muco-polysaccharide cysts which replace the smooth muscles in the elastin that is normally in the media layer
causes weakness and necrosis of the media making a tear in the artery more likely
DeBakey classification of aortic dissection
- type I
DeBakey classification of aortic dissection
- type II
DeBakey classification of aortic dissection
- type III
Stanford classification of aortic dissection
- type A
Stanford classification of aortic dissection
- type B
chest pain - inter scapular - severe and sudden
collapse due to tamponade, acute aortic regurgitation, external rupture
stroke - involvement of carotids
reduced or absent peripheral pulses
hyper or hypotension
BP mismatch between sides
soft early diastolic murmur (aortic regurg)
pulmonary oedema
signs of cerebral vascular accident
ECG - ST elevation/ischaemia indication of coronary involvement
CXR - widened mediastinum
transthoracic ECHO - examine aortic root
CT angiogram aorta - confirm diagnosis
BP control
beta blocker
IVI nitrate
CCB
IVI sodium nitroprusside
emergency surgery
BP control
beta blocker
IVI nitrate
CCB
IVI sodium nitroprusside - careful can cause cyanide poisoning
percutaneous (end-vascular) intervention (PCI)
bicuspid aortic valve
coarctation of aorta
marfans
leaflets of aortic valve have fused together
most common congenital abnormality
associated with coarctation of aorta
reduced tensile strength in aorta
pre-ductal
can be life threatening if severe narrowing
ductal
post-ductal
hypertension on upper extremities
weak pulses in lower limbs
associated with rib notching
cold legs
poor leg pulses
radio-radial delay - before left subclavian artery
right radial-femoral delay - before left subclavian artery
right AND left radial-femoral delay - after left subclavian artery
heart failure and failure to thrive in infants
hypertension and CV complication on adults
CT or MRI
CXR - rib notching
PCI
surgical correction