np 7 documentation
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
23 Terms
medical record is aka _
chart
purposes of documentation
written record of history, treatment, care & response of patient while under care
guide for reimbursement of costs of care
may serve as evidence in law
shows use of np
provides data for quality studies
shows progress toward expected outcomes
if you charted on the wrong patient,
one line cross it out & put initial
documentation & nursing process
written nursing care plan / interdisciplinary are plan is framework for documentation
charting is organize by nursing diagnosis / problem
implantation of each intervention is documented on flow sheet / nursing notes
the medical record
only hcp directly caring for patient or involved in research or teaching have access to chart
pt info should not be discussed w anyone not involved
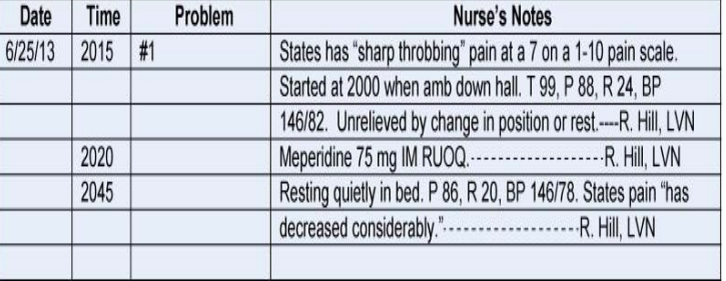
narrative / source charting
organized according to source of info
separate forms for nurses, physicians, dietitians, etc to document
requires documentation of patient care in chronologic order
pros and cons of narrative / source charting
pros: chronologic order. documents baseline condition for each shift. indicates aspects of all steps of np
cons: makes it difficult to separate important from irrelevant. discourages reading of everything. timely
problem-orientated medical record charting
POMR
focuses on patient status rather than medical / nursing care
5 basic parts
database (assessment)
problem list (found from database)
plan
progress notes
discharge summary
pros & cons of POMR
pros: focuses on problems, promotes problem-solving approach. relevant data in one place. easy auditing.
cons: loss of chronologic charting. more difficult to track trends in pt’s status. fragments of data bc more flow sheets required.
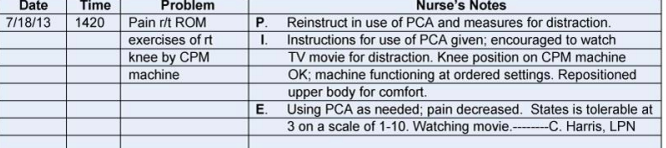
PIE charting
P: problem identification
I: interventions
E: evaluation
follows the nursing process and uses nursing diagnoses while placing the plan of care within the nurses’ progress notes
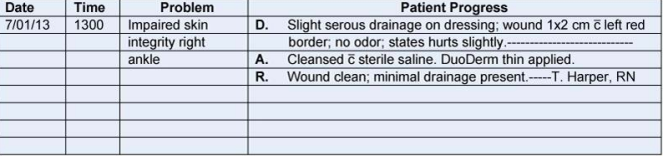
focus charting
directed at nursing diagnosis, patient problem, concern, sign, symptom, or event
Three components:
D: data, A: action, R: response (DAR)
D: data, A: action, E: evaluation
(DAE)
pros & cons of focus charting
pros: shortens charting time
cons: if database insufficient, pt problems are missed
charting by exception
based on the assumption that all standards of care are carried out & met with a normal / expected response. unless otherwise stated
longhand note only written when standard statement on form isn’t met
pros & cons charting by exception
pros: highlights abnormal data and trend. decreased narrative charting time. eliminated duplication charting
cons: requires detailed protocols & standards. requires staff to use unfamiliar methods.
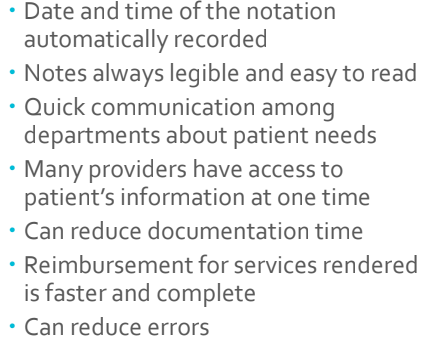
computer-assisted charting
electronic health record (CHE)
computerized record of pt history and care across all facilities & admissions
computerized provider order entry (CPOE)
efficient work flow
automatically routes orders to appropriate clinical areas
pros of computer-assisted charting
documentation can be done as implementations are preformed
cons of computer-assisted charting
case management system charting
method of organizing pt care through episode of illness
purpose: clinical outcomes achieved within an expected time frame & at a predictable cost
clinical pathway/ interdisciplinary care plan takes place of ncp
accuracy in charting
be specific & definite in words and phrases
words w ambiguous meanings / slang should not be used
observed, stated. not seems.
brevity in charting
sentences not necessary
using “pt” omitted. don’t have to use
abbreviations, acronyms, symbols can be used acceptable to agency
guidelines for documentations
location of s/s
quality & quantity
chronology (when it happened)
setting
aggravating & alleviating factors
triggers / manifestations
types of info to chart
admission note (ex arrived at 8:45 … completed …)
assessment (ex focused, daily, etc)
care
death
ADL function
tests & procedures
I&O
calls to PMD
changes in status
the kardex
quick reference for current information ab pt & ordered treatments. outdated
usually folded card for each pt that can be quickly flipped through pt & pt
not part of permeant medical record