Med Imaging: Lungs Pt 2
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
Bronchiectasis
Definition: thickening of the walls of the bronchi due to inflammation or infection. Can be diffuse or focal
Cause: chronic or severe infection damaging the bronchial cartilage (irreversible)
Common Pathogens: Klebsiella, S Aureus, Mycobacterium TB, Mycoplasma pneumo, nonTB mycobacteria, measles, pertussis, influenza, RSV, HSV, adenovirus
Associated Conditions: cystic fibrosis, allergic bronchopulmonary aspergillosis
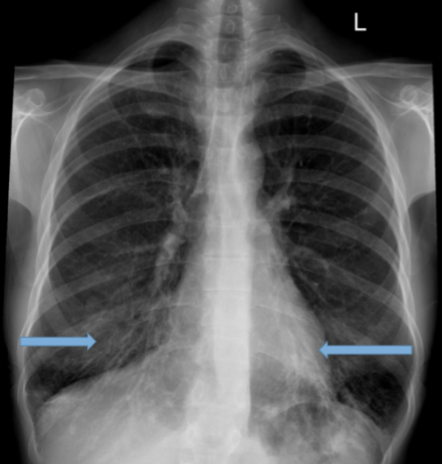
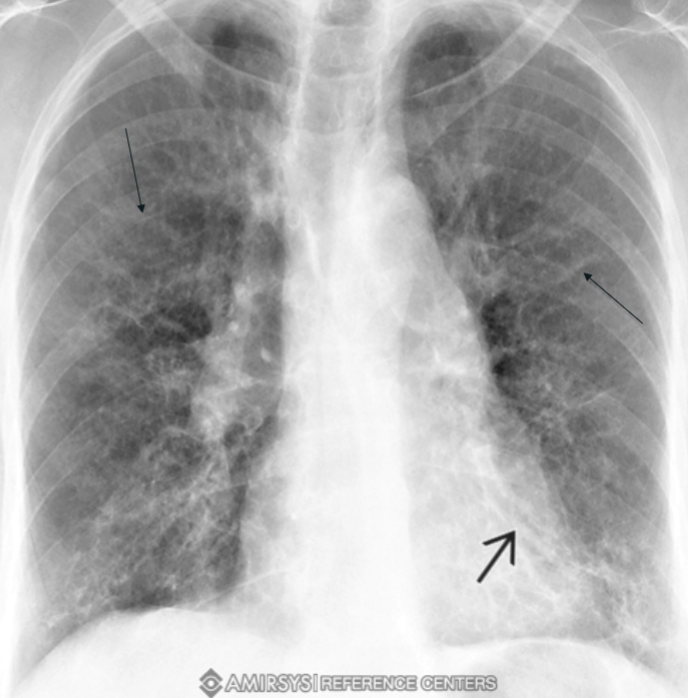
Bronchiectasis CXR
often normal or shows nonspecific findings. Later signs include tram-tracking and honeycomb infiltrates in the medial aspects of lower lobes
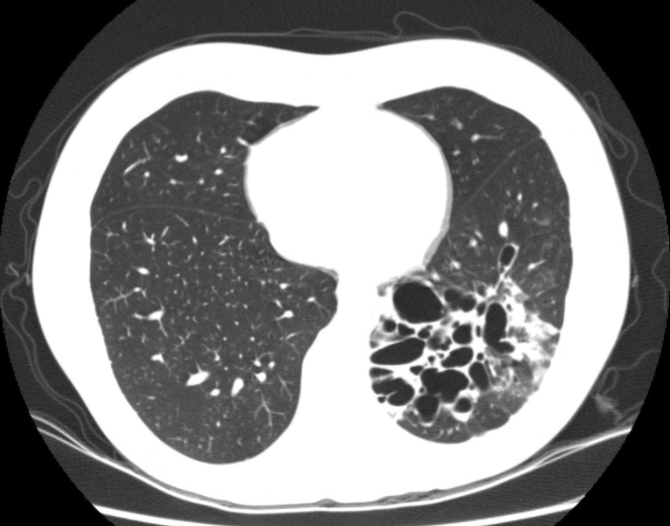
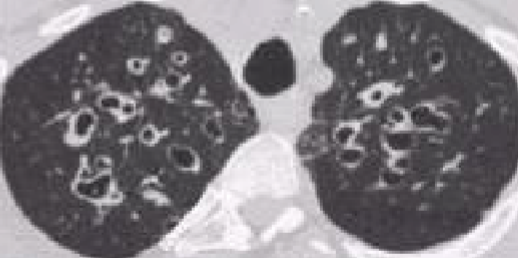
Bronchiectasis CT Scan
preferred method, clearly shows bronchiectasis
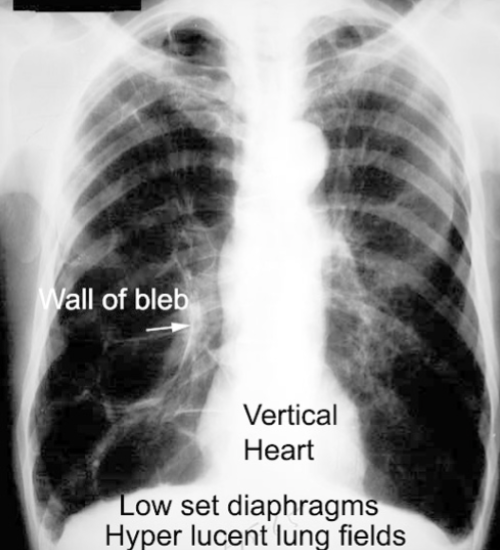
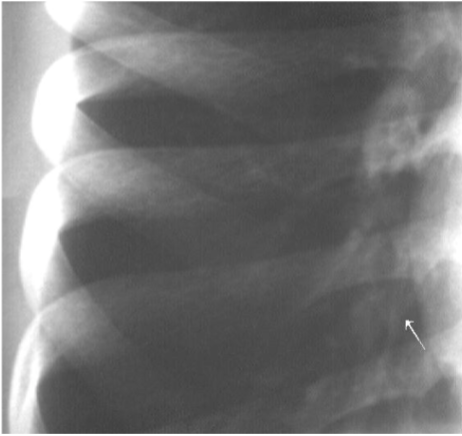
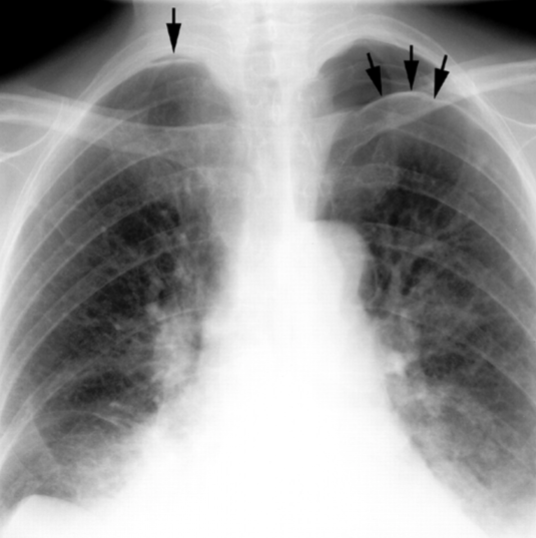
Blebs and Bullae
Definition: lung tissue w/ air space but no alveoli (non-functioning)
Bleb: < 1 cm in diameter
Bullae: > 1 cm, often much larger
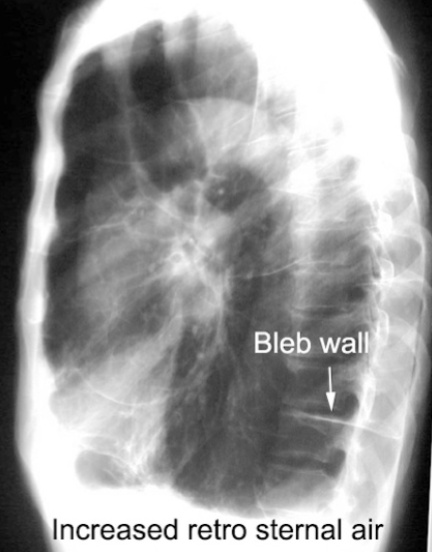
Blebs and Bullae: CXR
difficult to see, may appear as absence of pulmonary markings
Blebs and Bullae: CT Scan
easily seen
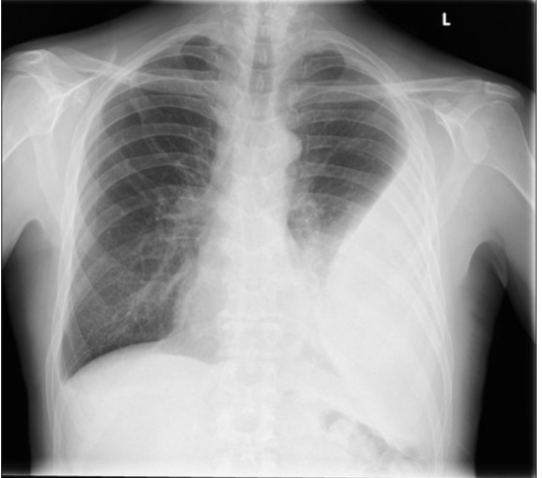
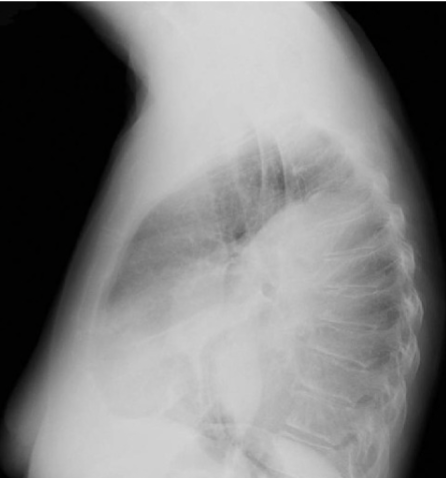
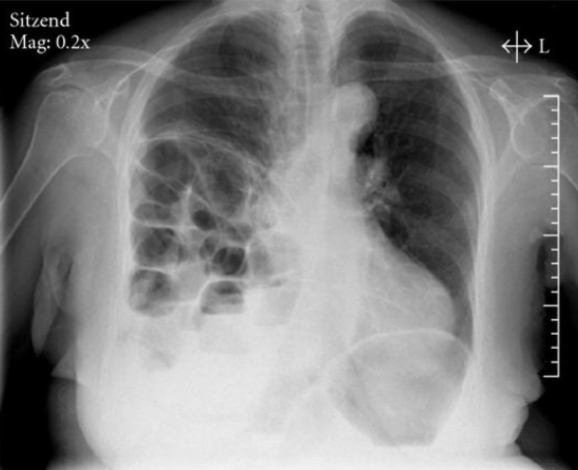
COPD/Emphysema
Definition: chronic obstructive pulmonary disease, a clinical dx

COPD/Emphysema: CXR
not indicated unless symptoms exacerbate. Normal in early stages, signs of hyperinflation in advanced stages
Signs: flattening of hemidiaphragms, blunting of costophrenic angles, inc AP diameter, presence of bullae or large air cavities
Atelectasis
Definition: complete or partial collapse of the lung or a lobe
Cause: no air reaching the alveoli due to obstruction, compression, fibrosis, or loss of surface tension
Types: liner (discoid or plate-like) - often seen post-op

Atelectasis: CXR
confirms atelectasis, differentiates from air-space opacification
Atelectasis: CT Scan
may be needed to determine the cause
Asthma: CXR
usually not indicated in acute exacerbations. Long-standing may show interstitial patterns due to scarring or mild bronchiectasis
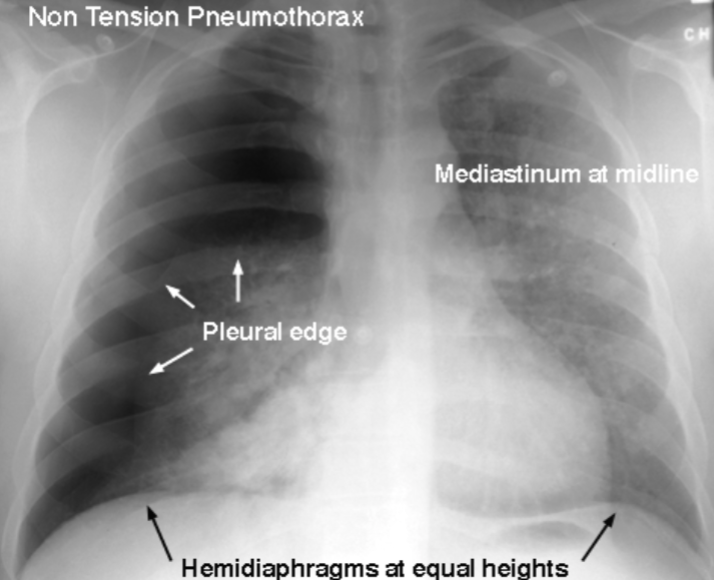
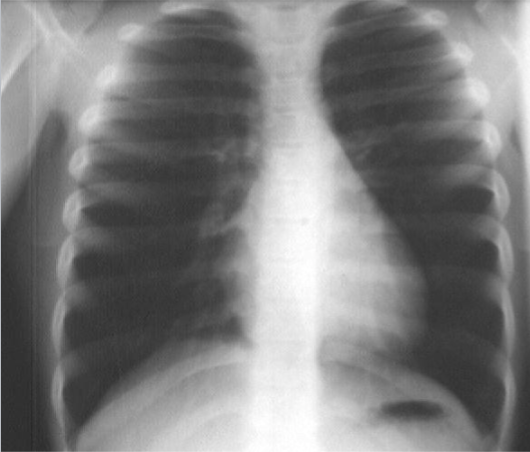
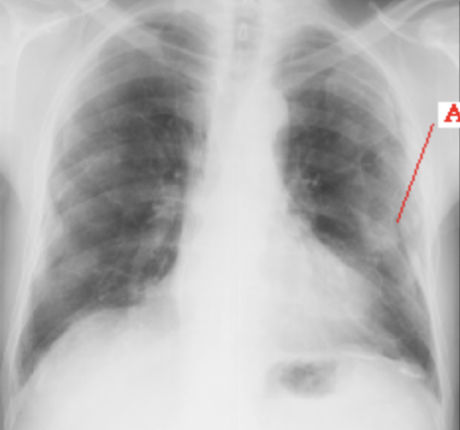
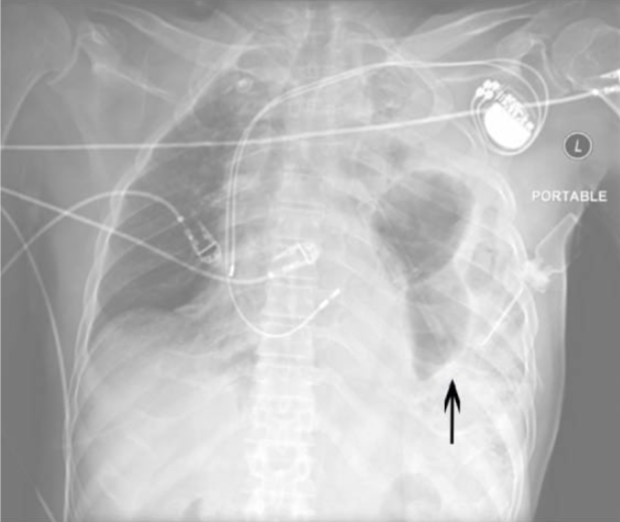
Pneumothorax
air in the pleural space causing lung collapse. Seen as an area of no vascularity and a thin white line on CXR
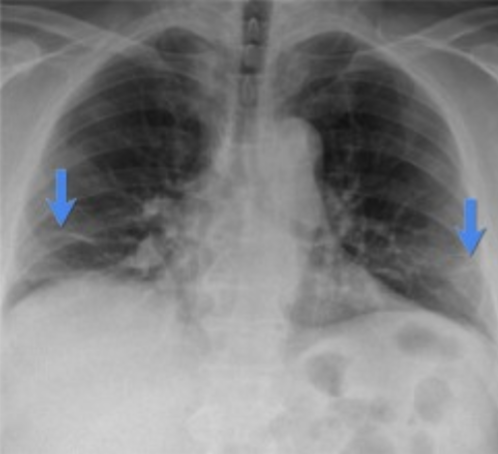
Pleural Effusion
fluid in the pleural space. Causes include CHF, pneumonia, pancreatitis, cirrhosis, malignancy

Pleural Effusion: CXR
upright shows costophrenic angle blunting, lateral decubitus shows fluid along the lateral chest wall

Pleural Effusion: CT Scan
indicated for suspect loculated effusion or empyema
Empyema
Pus in the pleural space. Appears elliptical and can be loculated. Best visualized w/ CT scan
Pleural Calcifications & Masses
result from old calcified empyema or asbestosis. Mesothelioma may appear as a focal pleural mass

Diaphragmatic Rupture
Cause: usually due to trauma, more common on the left side
Imaging: loops of bowel in the lower chest cavity, best seen on CXR
Hemoptysis
Coughing up blood. CXR indicated if true hemoptysis
Chest pain or Dyspnea
CXR indicated if exam is abnormal or pt is over 40 or at risk for CVD
Hypertension
CXR not needed for routine follow-up but may be useful in new onset w/ tobacco use Hx or symptomatic cases

CHF
CXR indicated for Dx and progression. Shows progressive changes from normal to pulmonary edema

Mediastinal Lesions
Definition: lesions in the mediastinum, can be focal or diffuse, anterior, middle, posterior
Imaging: CT scan or MRI w/ contrast is always indicated. MRI preferred for neurogenic lesions

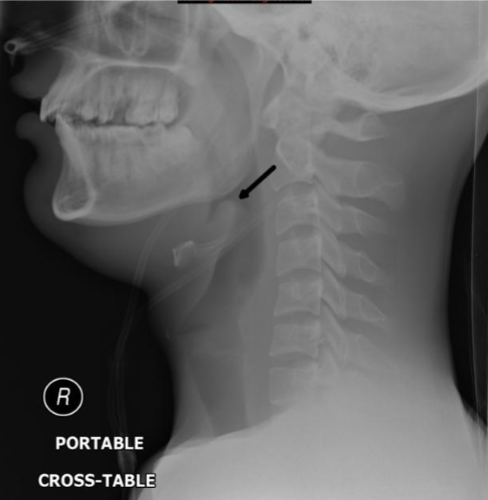
Epiglottis
Definition: inflammation of the epiglottis
Causes: infectious (H influenza type B, group A B-hemolytic Strep, TB) or inflammatory (sarcoidosis)
Anterior lesions
Thymoma, thyroid lesions, teratoma, T-cell lymphomas, lymphadenopathy
Middle lesions
Thoracic aortic aneurysms, hematomas, neoplasms, lymphadenopathy, esophageal lesions, diaphragmatic hernias
Posterior lesions
Neurogenic lesions, hiatal hernias, descending aortic aneurysm, neoplasms, hematomas