5- Impacted Cuspids (Dr. Salam)
1/102
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
103 Terms
True
T/F: Teeth tend to erupt in the same sequence in which they calcify

6124537
(1M, Ci, Li, 1PM, 2PM, C, 2M)
What is the most common (favorable) eruption pattern in the maxillary arch?

6124753
(1M, Ci, Li, 1PM, 2M, 2PM, C)
(2nd molar before the canine is bad; when we see 2nd molars erupting before the 2nd premolar it encroaches on the space of the 2nd premolar)
What is the MOST UNFAVORABLE pattern of eruption for the maxillary arch because it leaves no space for the canine??
True
T/F: Teeth generally erupt in pairs
0.92-2.2%
What is the prevalence of canine impaction in the population?
Females
Is canine impaction 2x more common in males or females?
8%
__% of all impacted canines are bilateral impactions
labially or within the alveolus
About 1/3 of impacted maxillary canines are positioned ________
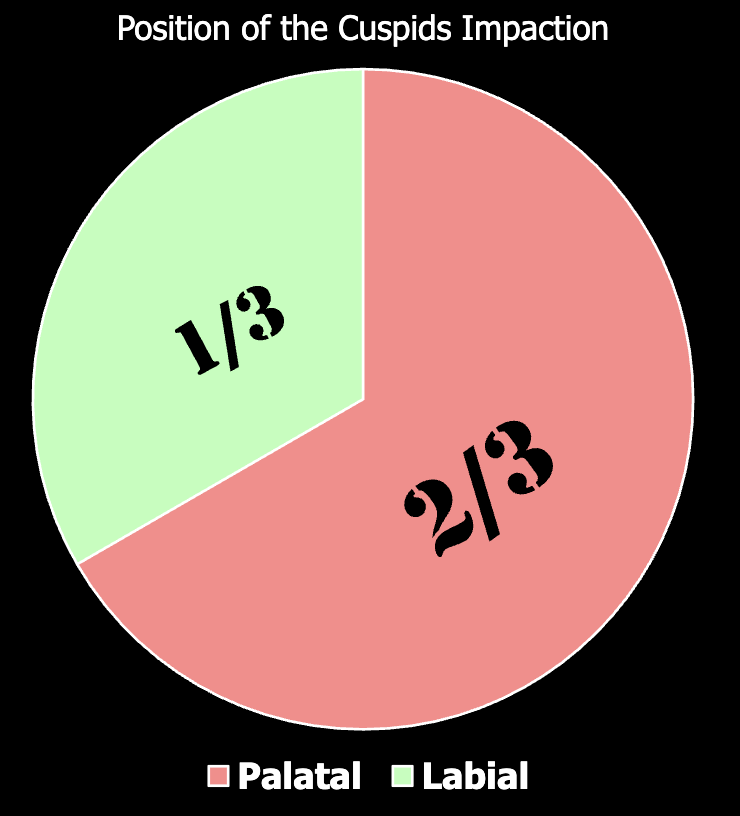
palatally
About 2/3 of impacted maxillary canines are positioned ______
Tooth size-arch length discrepancies
Failure of the primary canine root to resorb
Prolonged retention or early loss of the primary canine
Ankylosis of the permanent canine
Cyst or neoplasm
Dilaceration of the root
Absence of the maxillary lateral incisor
Variation in root size of the lateral incisor (that is, peg-shaped lateral incisor)
Variation in timing of lateral incisor root formation
latrogenic factors (failing to maintain space)
Idiopathic factors
What are the local etiologies for impacted canines?
ankylosis/impaction of the permanent canine
Ankylosis is a potential cause of prolonged retention of the primary canine, and prolonged retention may be a clinical sign suggesting __________
Congenital absence of the maxillary lateral incisor
Peg-shaped maxillary lateral incisor
Altered timing of lateral incisor root formation
A 12-year-old patient presents with an impacted maxillary canine. What are 3 abnormalities of the maxillary lateral incisor that have been associated with canine impaction?
Endocrine deficiencies (pituitary hypofunction & hypothyrodism)
Febrile diseases
Irradiation
What are the 3 systemic etiologies for impacted canines?
Hereditary
Malposed tooth germ
Presence of an alveolar cleft
What are the genetic etiologies for impacted canines?
2.5x
If a patient is missing their lateral incisor, what is the incidence of palatally impacted canines?
Maxillary canine loses eruption guidance owing to an absent lateral incisor
how come palatally impacted canines are more common when pts are missing their lateral incisor
proposes that the canine erupts along the root of the lateral incisor, which serves as a guide
what’s the guidance theory
genetic factors are a primary origin of palatally displaced maxillary canines and includes possibilities of other associated dental anomalies, such as missing or PEG-SHAPED lateral incisors.
what’s the genetic theory
True
T/F: It remains uncertain whether an anomalous lateral incisor is a local causal factor for palatally displaced canines or the displaced canines are the result of an associated genetic developmental influence.
Passed eruption time- especially if unilateral
Excessive distal flaring of the lateral incisors
Exaggerated labioversion of the laterals
What are 3 clinical signs that suggest a maxillary canine impaction?
8 years old
At what age should you start to palpate a buccal canine bulge between the lateral incisor and 1st premolar roots?
Palatal displaced cuspid
If a 10 year old patient has a lack of positive palpation of the canine buccal bulge and distal inclination of the laterals, what can you infer?
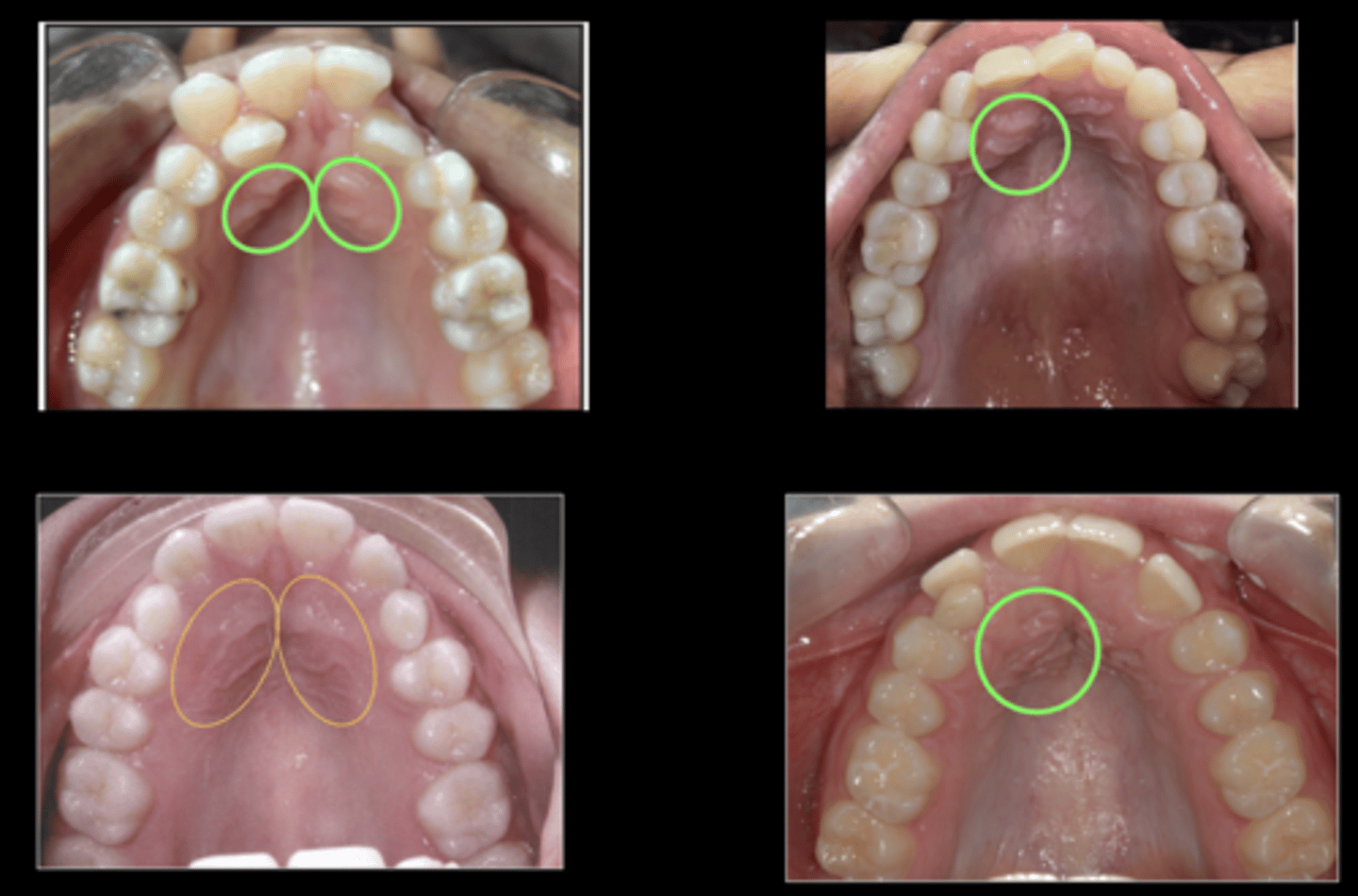
Lack of a distinctive cuspid bulge on the labial
Evidence of a palatal bulge
What are 2 clinical signs that suggest a palatally displaced maxillary canine?
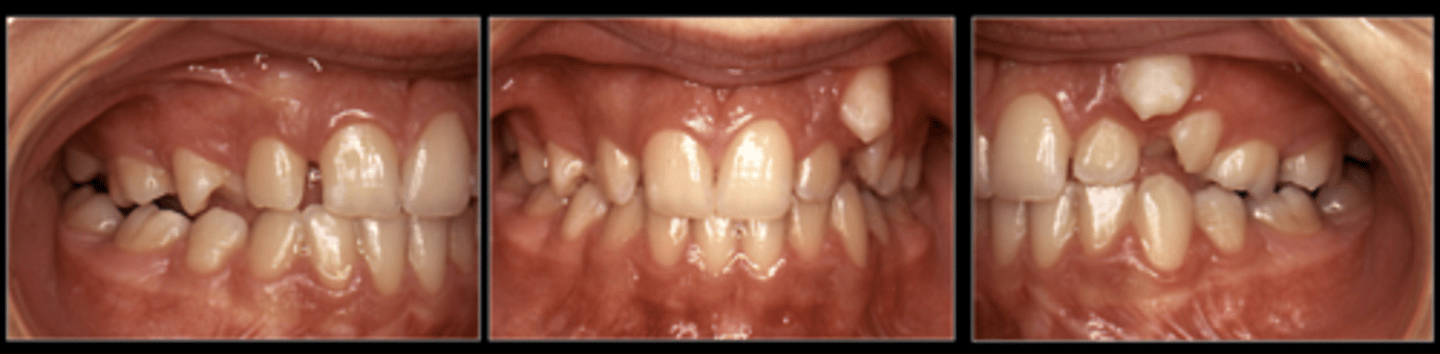
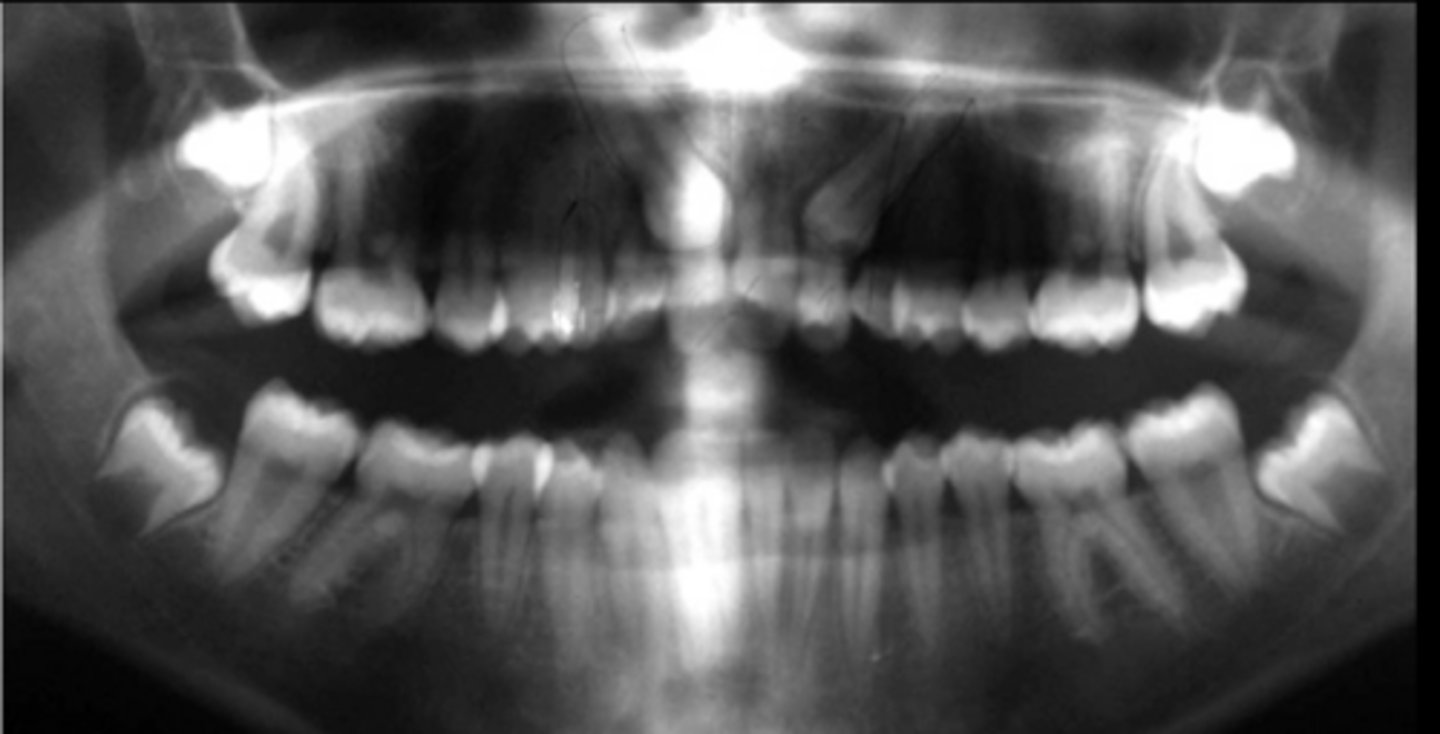
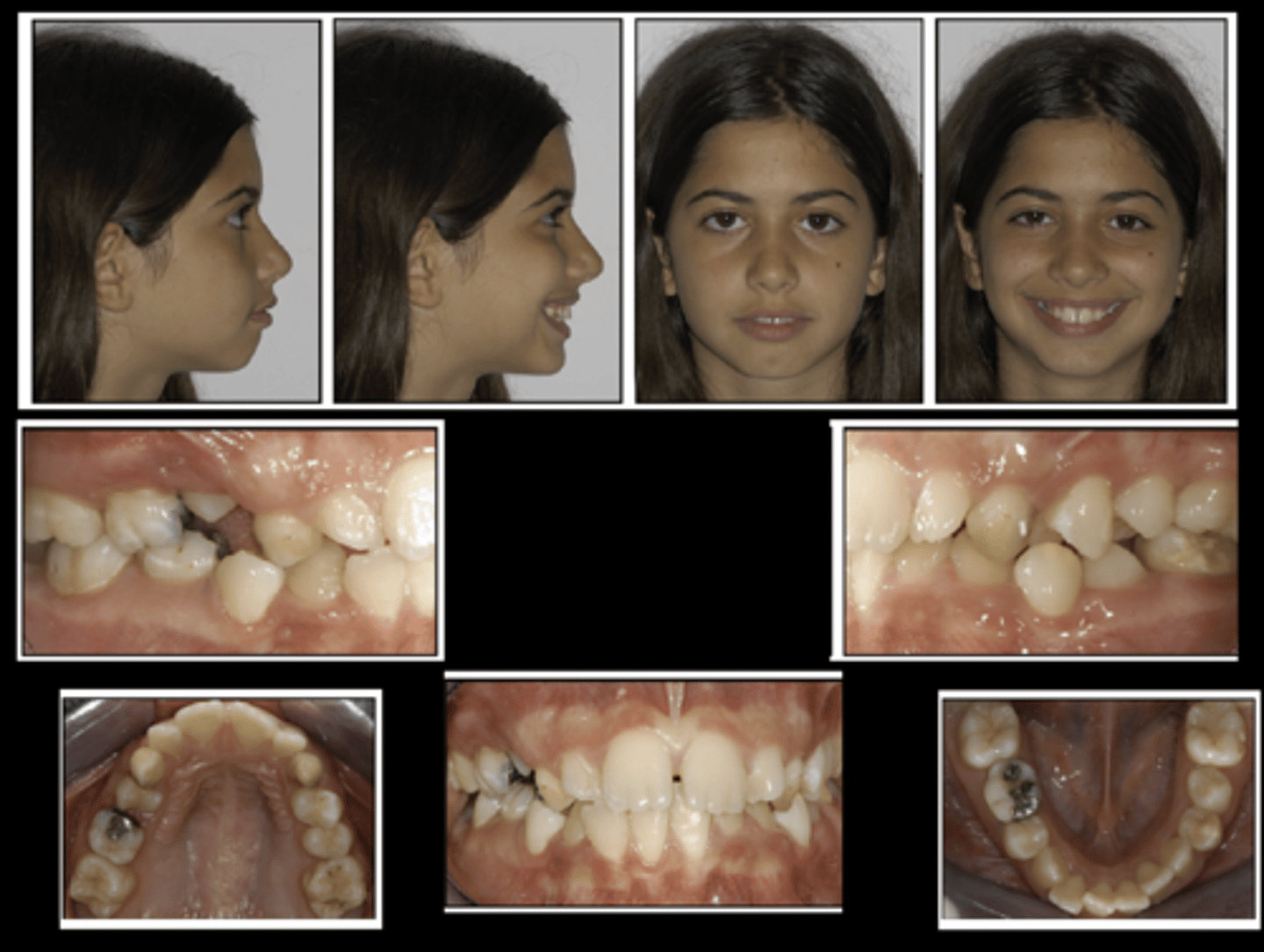
Labially displaced cuspids
What do these photos suggest?

- Left - Failed to erupt
- Right - Ectopically erupted
What is the difference between the image on the left and right?
Palatally (more radiopaque, sharper, and bigger)
This image shows bilaterally impacted canines. Do you think the patient's right canine is palatally or labially displaced?
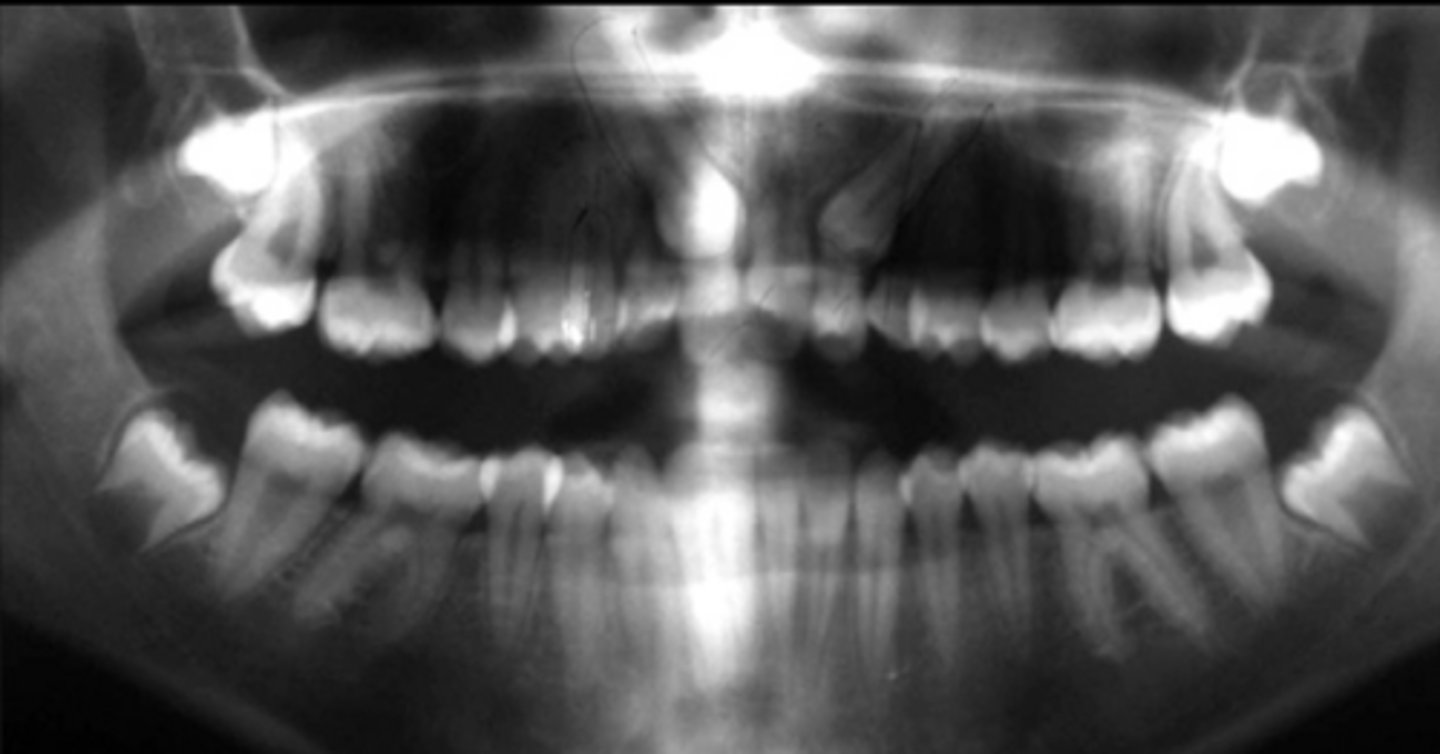
Labially (less radiopaque and smaller)
This image shows bilaterally impacted canines. Do you think the patient's left canine is palatally or labially displaced?
- Same Lingual
- Opposite Buccal
What is the SLOB rule?
Frontal and lateral cephalograms
What images can sometimes aid in the determination of the position of the impacted canine, particularly its relationship to other facial structures?
In general, it is challenging to distinguish structures based on conventional 2D radiographs, which often lead to misinterpretations.
CBCT
What images allow not only a detailed localization of impacted canines, but also their relation to adjacent teeth and THE SURROUNDING anatomical structures in the 3 Dimensions?
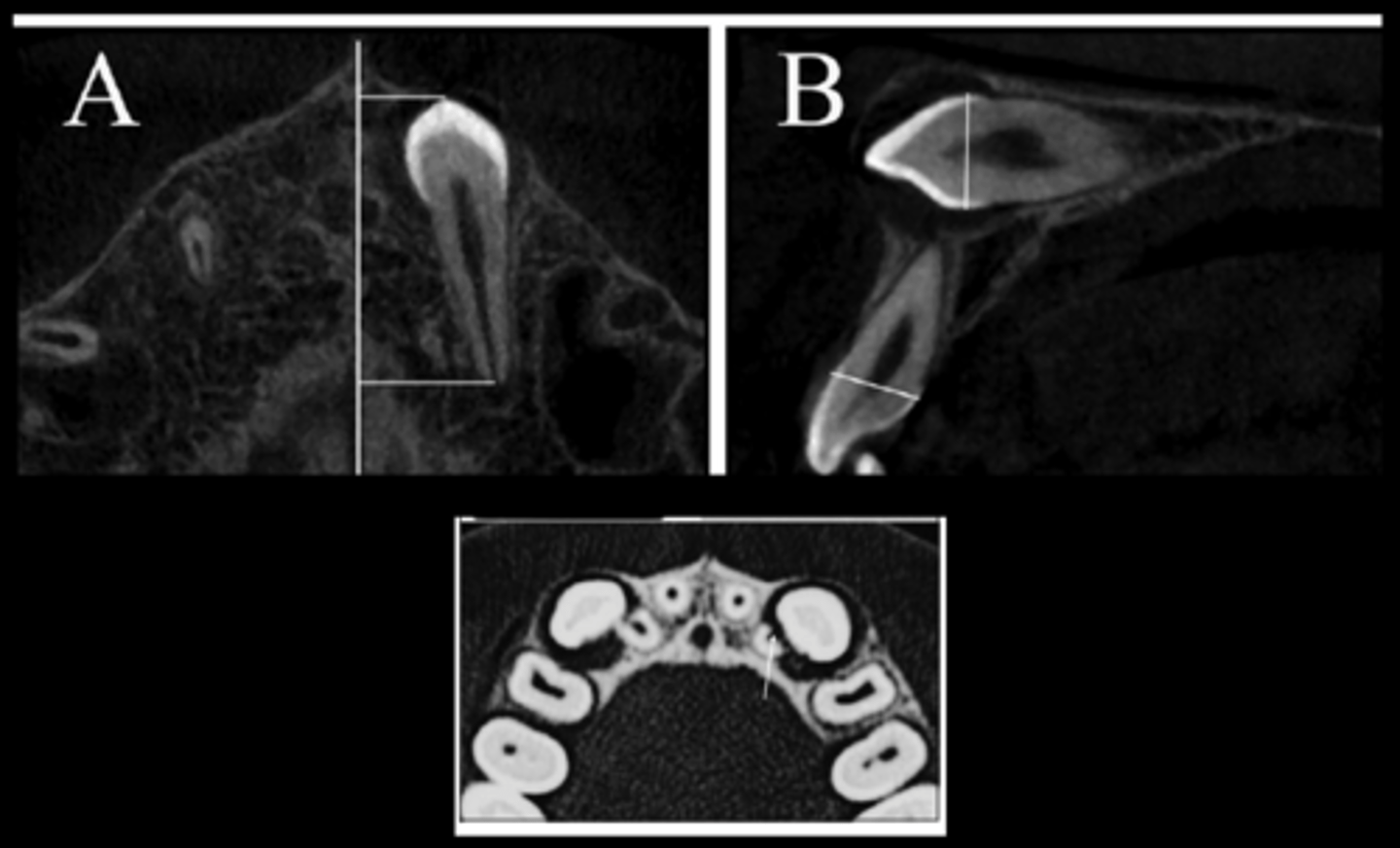
It is displaced totally horizontal
What do these images indicate about the canine?
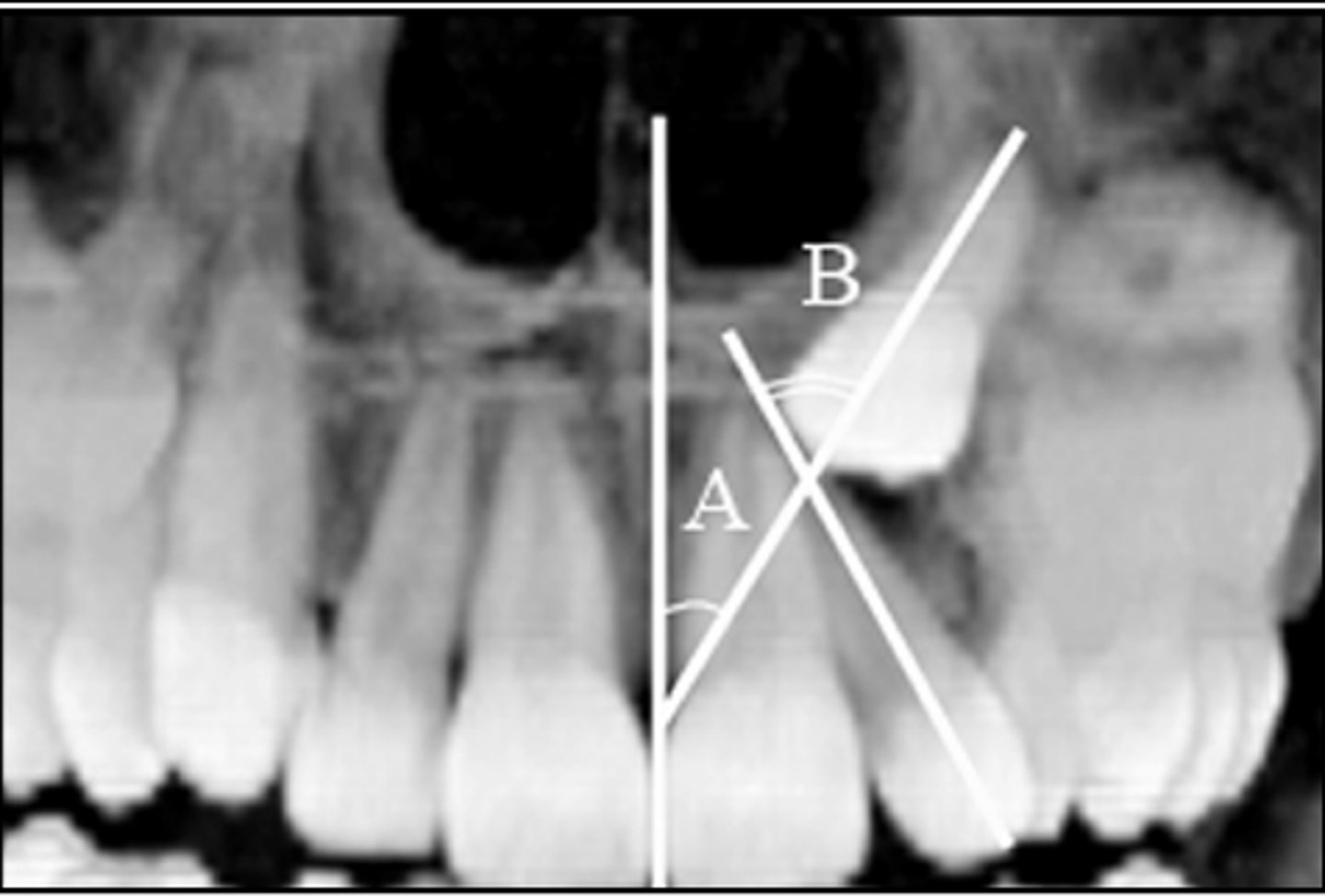
- A: Canine angulation to the midline
- B: Canine angulation to the lateral incisor
What do these images indicate about the canine?
1) Ankylosis of the canine(s)
2) External or internal resorption of the cuspid
3) Formation of follicular cysts
4) Displacement
5) Dilaceration of the cuspid root
6) Loss of vitality or resorption of the adjacent teeth
What is the sequelae of impacted canines if left untreated?
2-3mm
What is the normal space needed for a dental follicle for a tooth to erupt?
12%
Resorption of the roots of the adjacent permanent incisors occur in ___% of cases of ectopic eruption of the maxillary canines in the age range 10-13 years
lateral
Of the 12% incidence of resorption, distribution of resorbed teeth is 80% _____ incisors
8 or 9 years old
At what age might it be appropriate to selectively extract maxillary deciduous (primary) cuspids for an impacted permanent canine?
91% (distal to long axis = more successful)
If a permanent canine is distal to the long axis of the primary lateral incisor and is already growing ectopically, early removal of the primary canine can result in self correction and eruption of the permanent canine ___% of the time
64% (mesial to long axis = less successful)
If a permanent canine is mesial to the long axis of the primary lateral incisor and is already growing ectopically, early removal of the primary canine can result in self correction and eruption of the permanent canine ___% of the time
the proximity of the permanent canine to the midline of the lateral root
self correction + eruption of permanent canine rate of success after early removal of primary canine depends on
True
T/F: Extraction of the primary canine (along with RPE) may offer a possibility of (78%) correcting impacted canines path of eruption
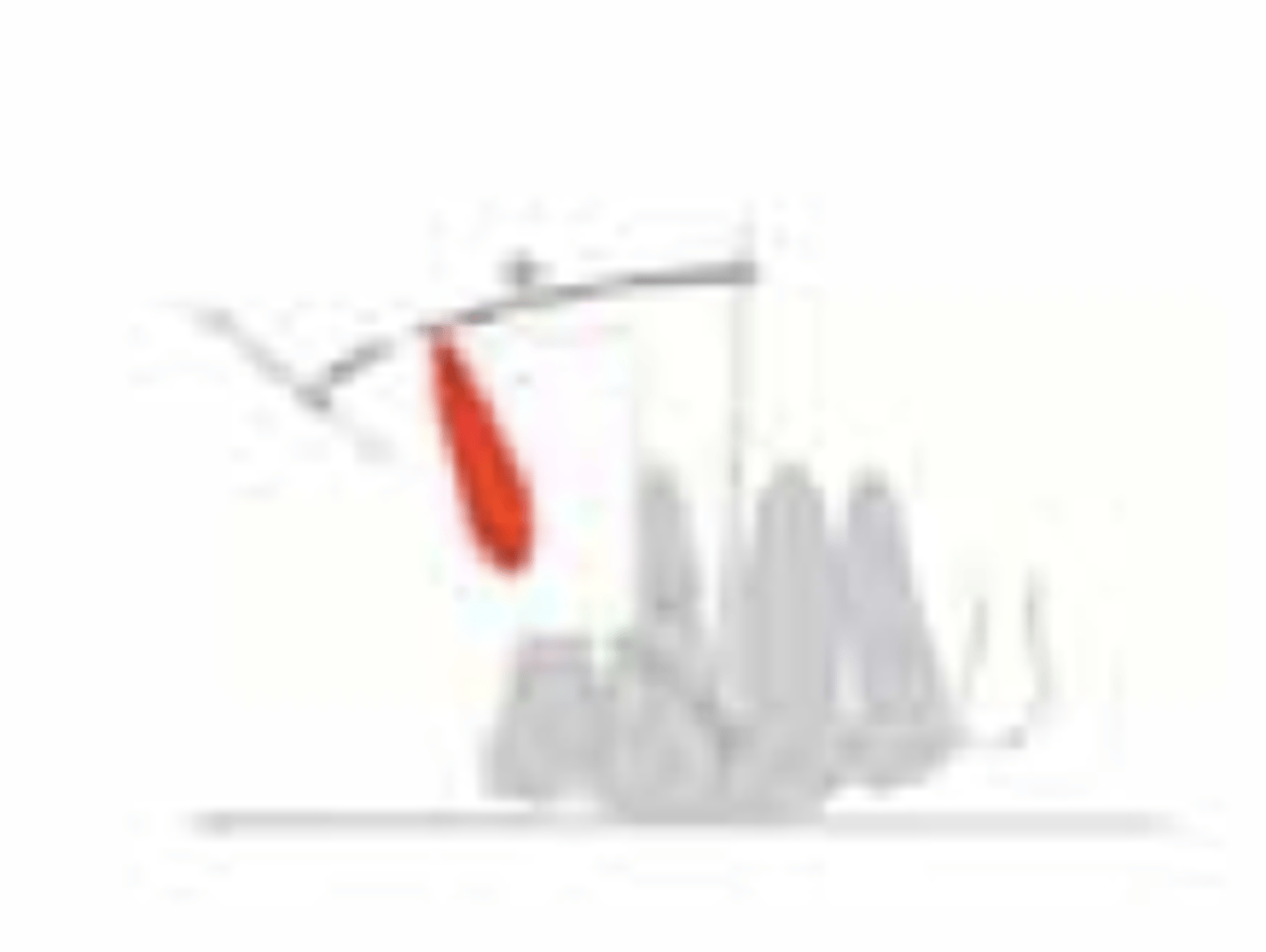
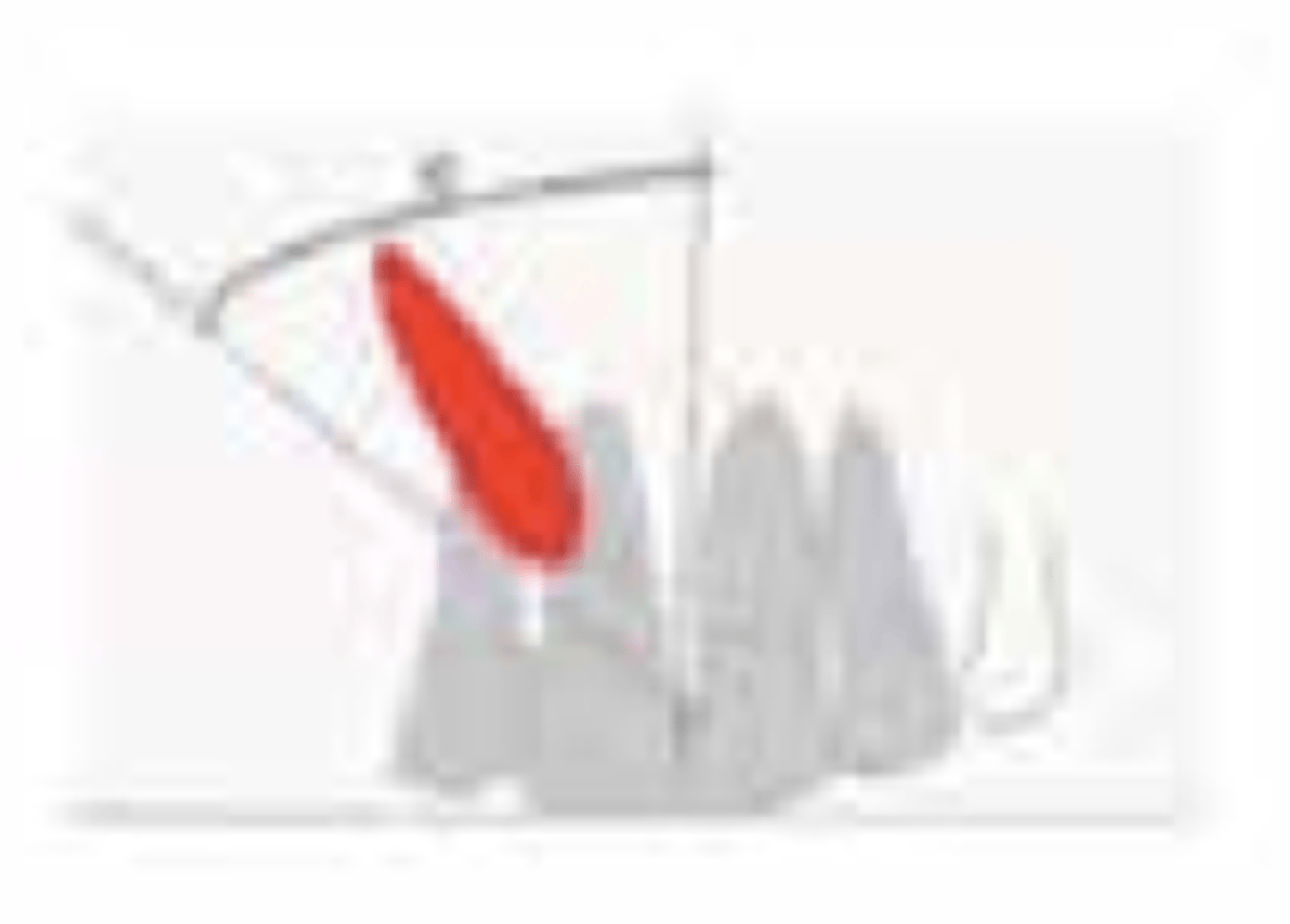
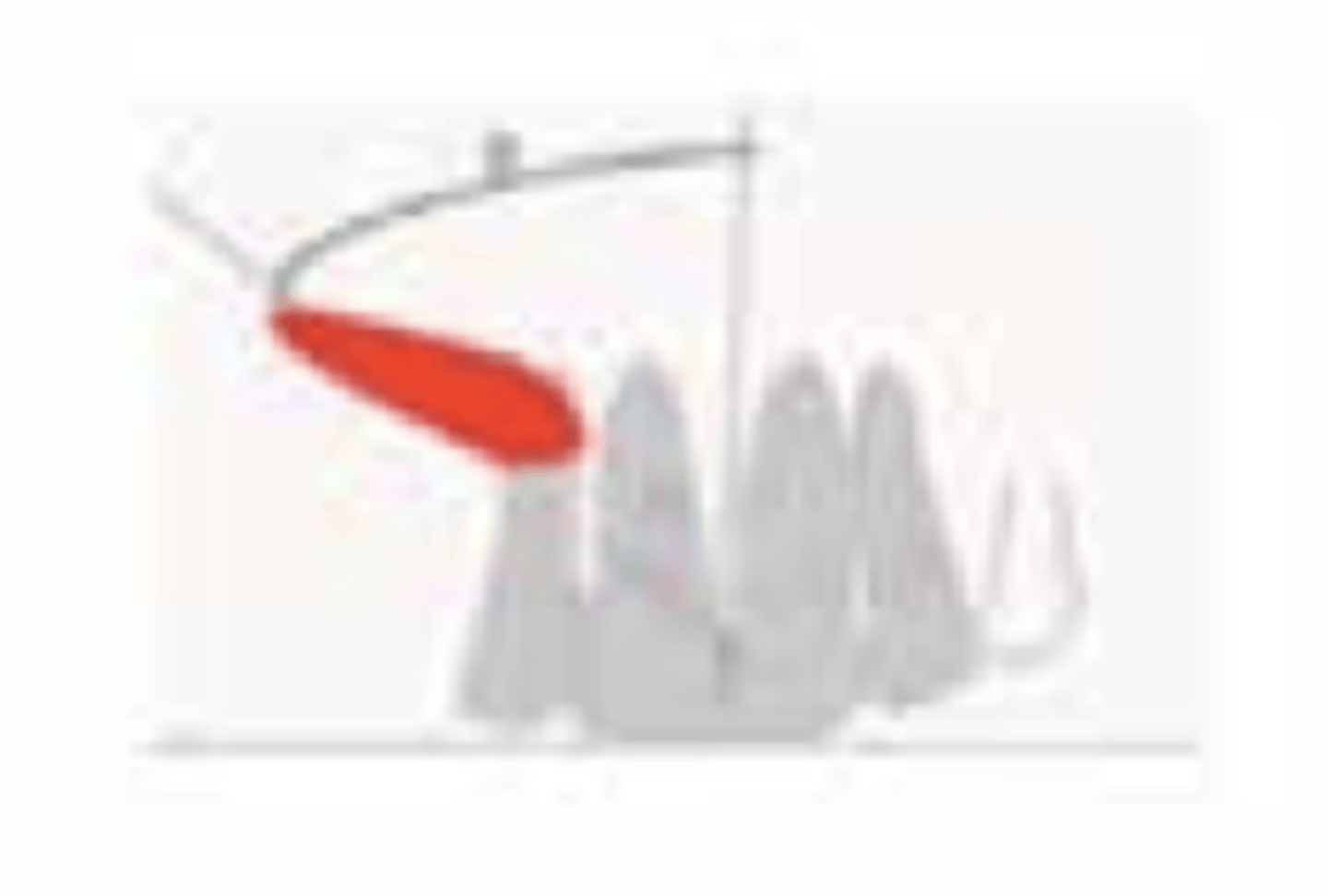
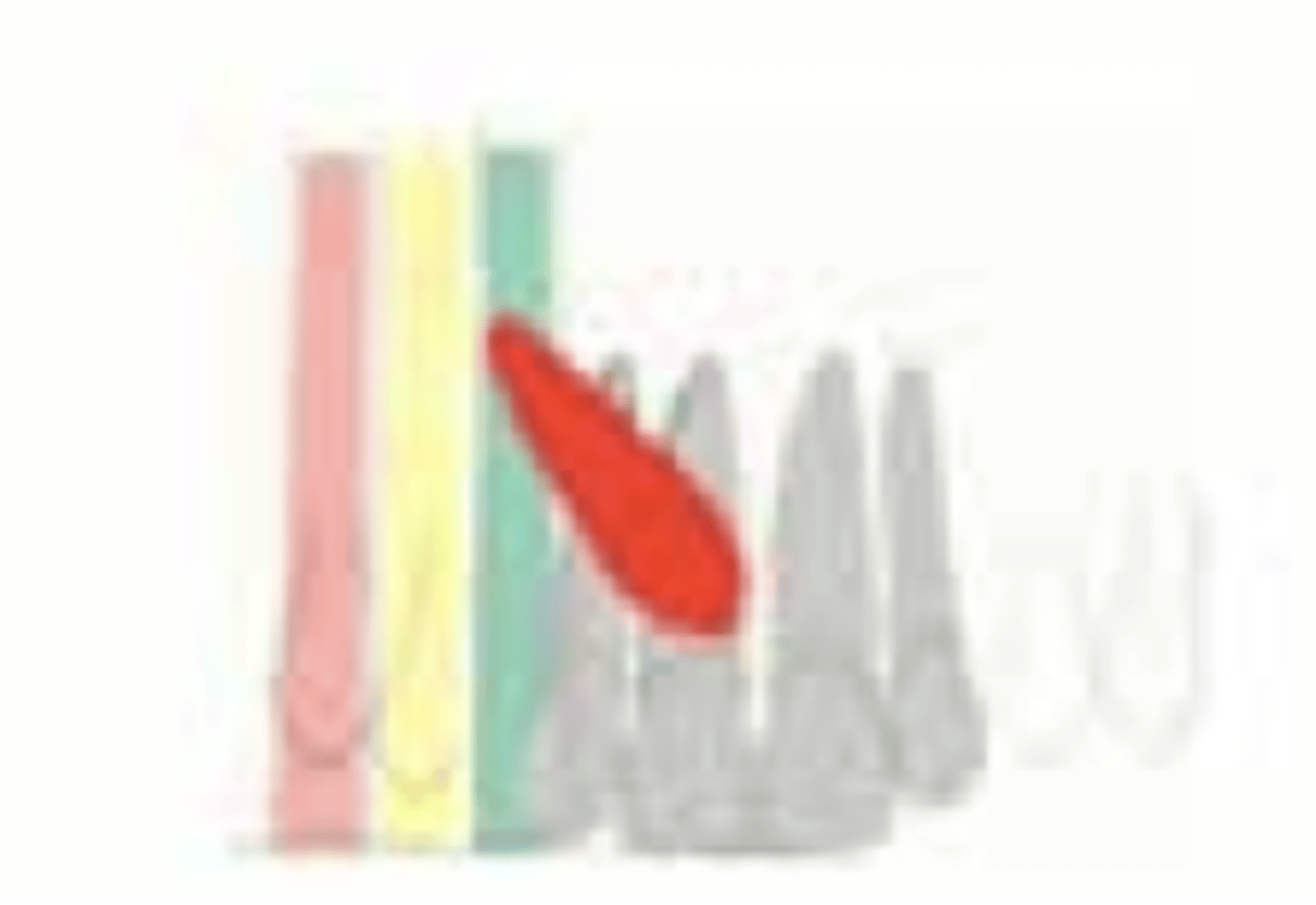
Decreased
Canine inclination (C.I.) to the midline, perpendicular distance (d) from the occlusal plane line, and zones (1-5) of the impacted canine crown. If canine angulation is more than 30 degree to the midline, the chances of spontaneous eruption after deciduous extraction are ___________
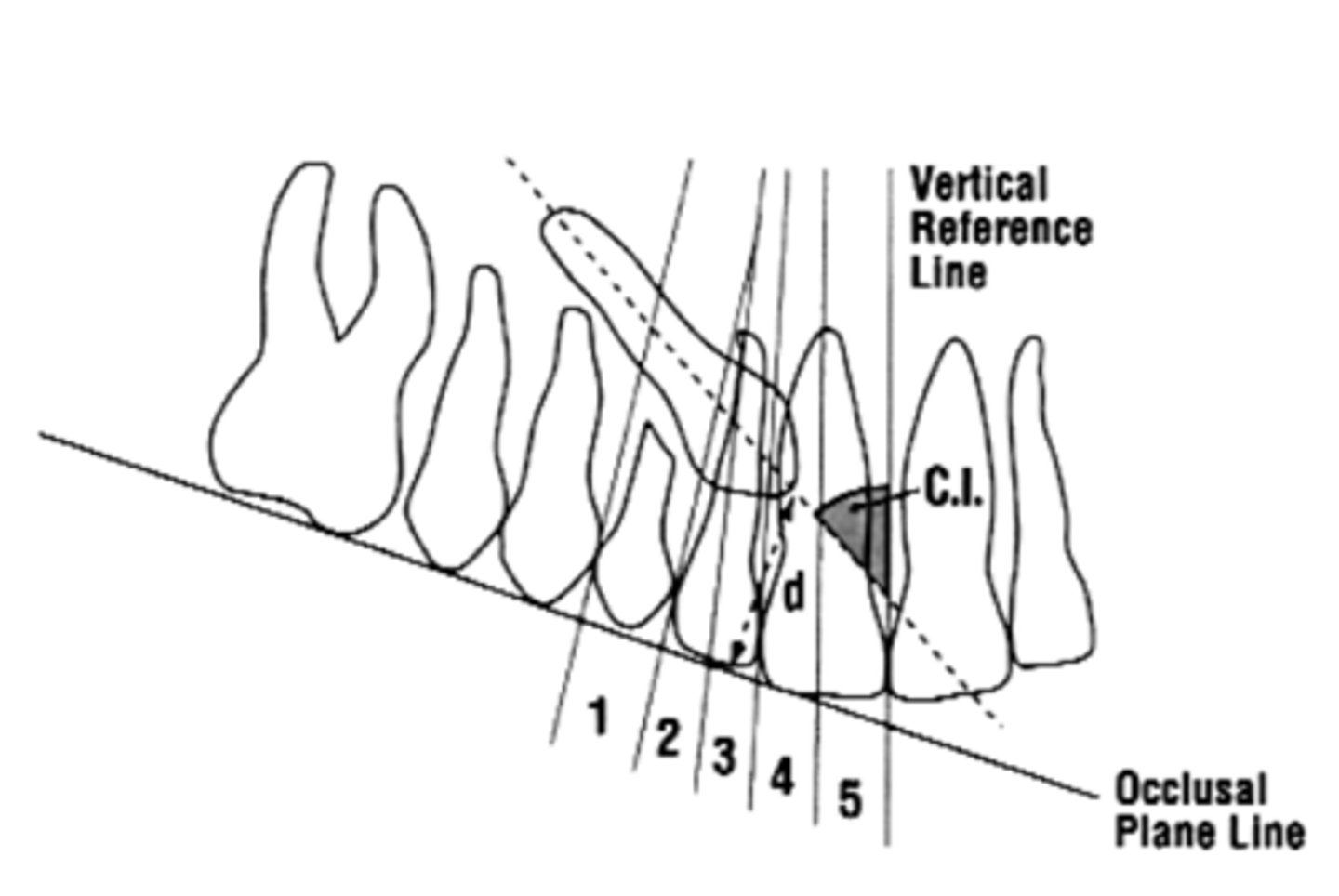
Labial impactions
(If given enough space; Palatal impactions are generally more horizontally inclined than are labial impactions and so Palatal impactions generally will not erupt on their own)
What is more likely to erupt on their own: labial or palatal impactions?
Palatal
What impaction is more horizontal: labial or palatal?
Good
What is the prognosis?
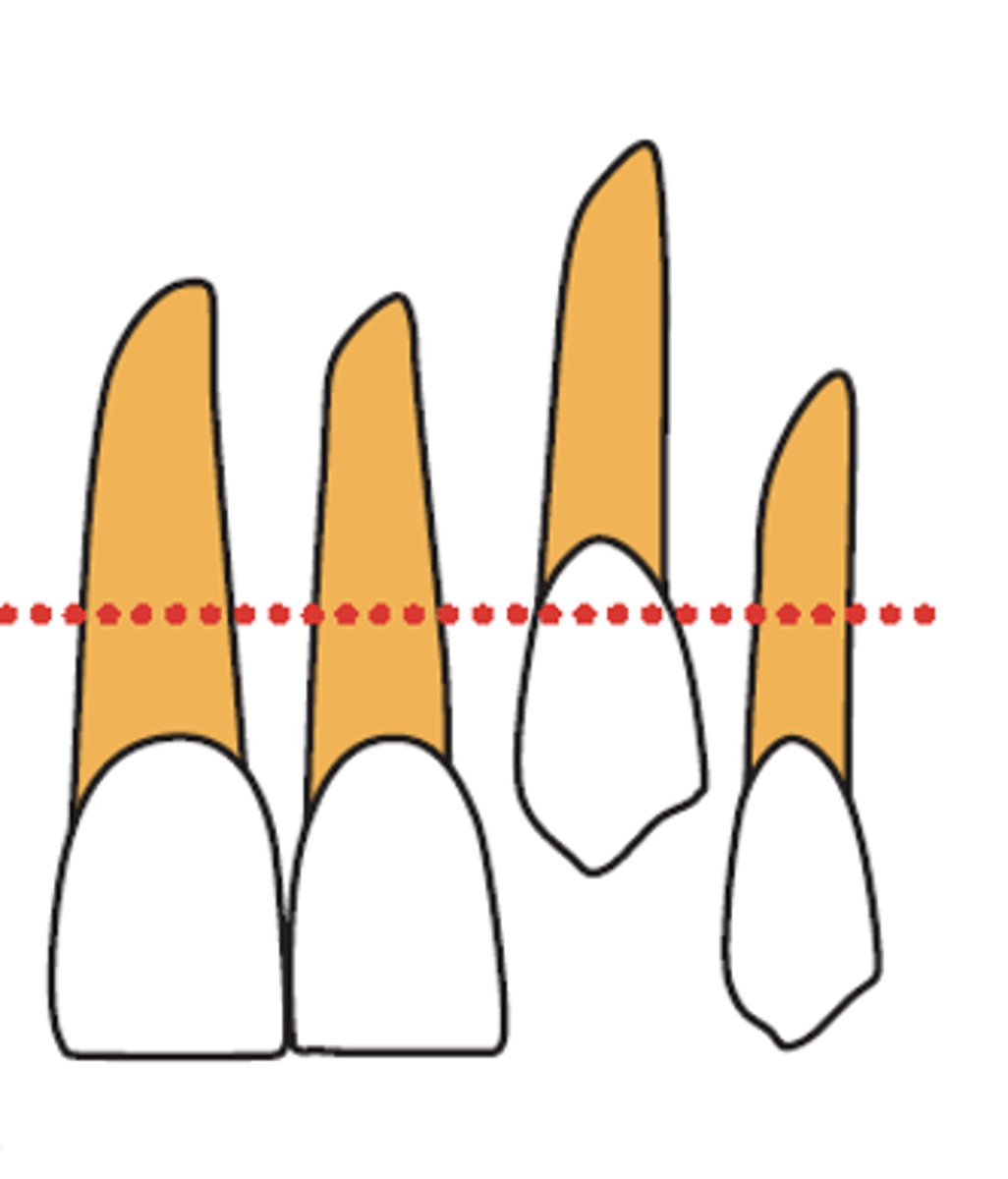
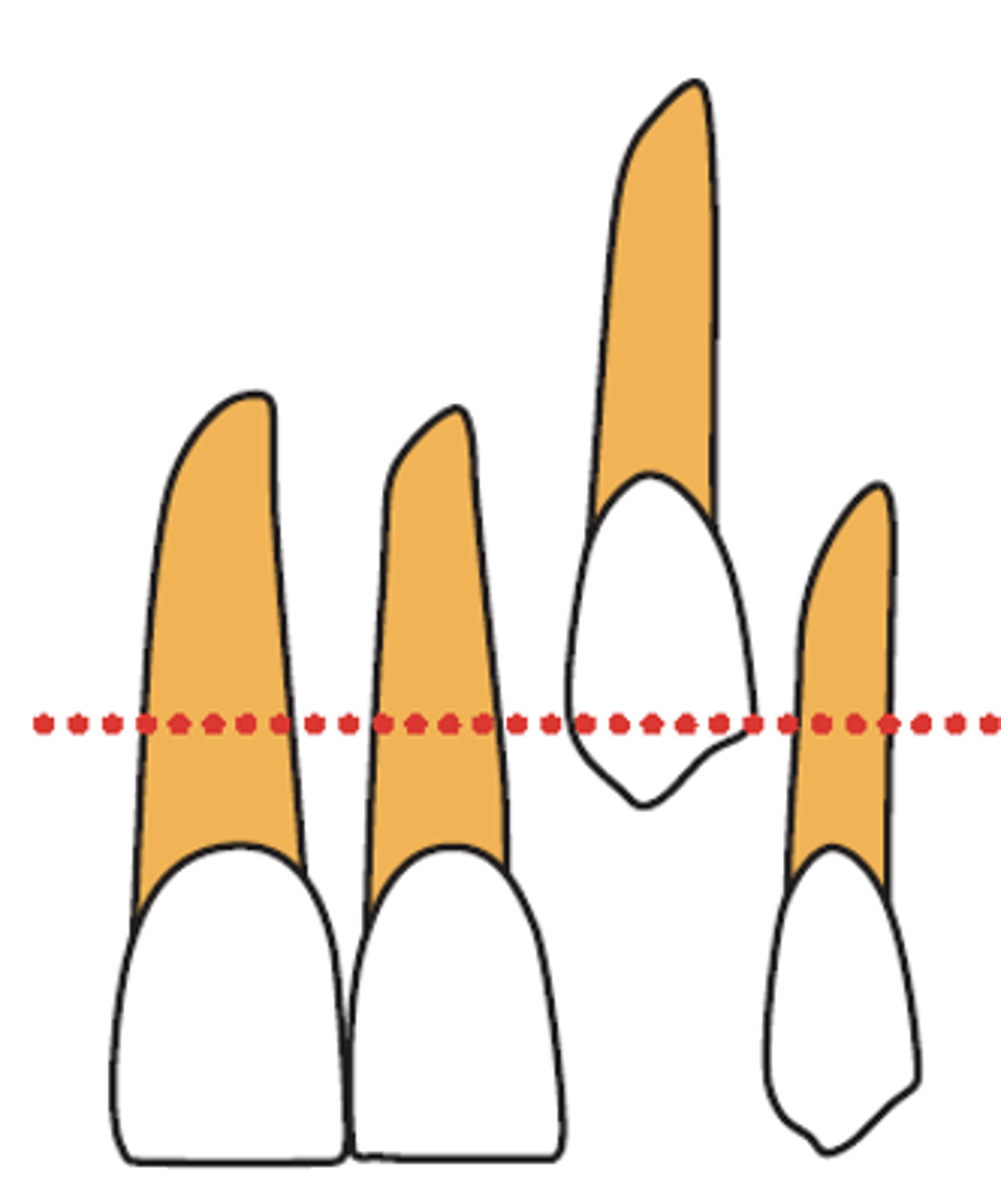
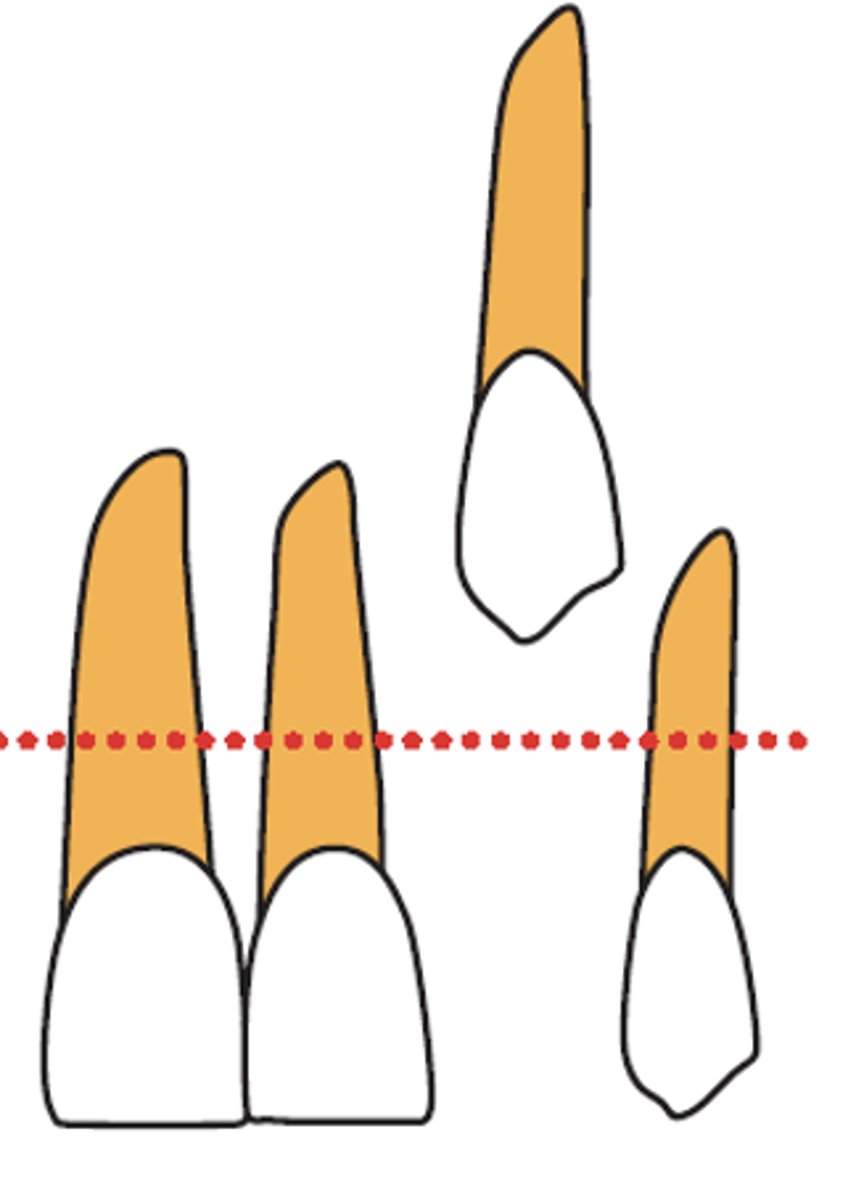
- No horizontal overlap of incisor

Average
What is the prognosis?
- Up to half root width overlap of incisor

Poor
What is the prognosis?
- Complete overlap of incisor
Good
What is the prognosis?
- Vertical Height: CEJ - halfway up root
Average
What is the prognosis?
- Vertical Height: >half
Poor
What is the prognosis?
- Vertical Height: >full root length
Good
What is the prognosis?
- Angulation: 0-15°
Average
What is the prognosis?
- Angulation: 16-30°
Poor
What is the prognosis?
- Angulation: >30°
Good
What is the prognosis?
- Position of apex: Above canine position
Average
What is the prognosis?
- Position of apex: Above 1st premolar
Poor
What is the prognosis?
- Position of apex: Above 2nd premolar
No treatment and periodic monitoring
Autotransplantation of the cuspid
Surgical exposure and orthodontic traction of the impacted cuspid into the occlusal plane (with or without extraction)
Extraction of the cuspid and space closure (substitute with first permanent premolar)
Extraction of the cuspid and leave the canine space for a prosthetic replacement (single implant)
What are treatment alternatives for impacted canines?

Autotransplantation
What procedure?
The atraumatic surgical removal and movement of the maxillary canine from the impaction site to the correct position within the alveolar crest
It can bring a severely impacted canine directly into the dental arch with a single surgical procedure, potentially shortening orthodontic tx time
What is an advantage of autotransplantation?
It is a complex procedure, and clinicians must consider the risks of pulpal necrosis, root resorption, and/or ankylosis
What is a disadvantage of autotransplantation?
90%
What is the success rate of autotransplantation when providers respect the protocol?
Functional adaptation
Preservation of the alveolar ridge
Might recover its proprioceptive function and normal periodontal support
Compared with restoration with implants, transplanted teeth have what 3 advantages?
The impacted canine is in favorable position
The impacted canine is not ankylosed
No resorption to any of the neighboring roots (?!)
What are the 3 indications for surgical exposure + orthodontic traction of the impacted cuspid into the occlusal plane (with or without extraction)?
This is not typically the treatment of choice except in the following instances:
1. Transposition
2. External or internal resorption
3. Ankylosis
4. Pathology
5. Severity of the impaction - depth, distance from normal position, horizontal orientation
6. When the occlusion is perfect and the first bicuspid is in the correct position. (Removal of an impacted tooth can be indicated when clinical assessment of the treatment feasibility leads practitioners to no choice but extraction of the displaced tooth)
What are 6 instances when you should extract the impacted cuspid?
1. Maintain a Class I dental relationship
2. Align the maxillary and mandibular dental arches
3. Reduce dentoalveolar protrusion during smiling
4. Improve lip competence
5. Reduce mentalis strain
What are some treatment objectives for this case?
1. CREATE SPACE
2. Removal of any physical obstructions (supernumerary, odontoma, bone, etc)
3. Surgical exposure followed by spontaneous eruption
4. Mechanical Traction of the surgically uncovered impacted cuspids
Before deciding which treatment options to select, what are 4 diagnostic factors to consider with palatally impacted cuspids?
closed
opened w/ full flap
open window
3 surgical techniques used for exposing palatally impacted canines
Advantages:
- Less aggressive
- Less vertical relapse
- Better esthetic outcomes
Disadvantages:
- Tooth is invisible
- Orthodontic force cannot be controlled during traction
- Patient discomfort
- Repeat procedure if attachment/chain breaks
advantages vs. disadvantages of closed surgical technique
opened w/ full flap
which surgical technique is indicated for palatal mucosa, periosteum, and bone removal then suturing coronal to the CEJ
closed
which surgical technique is indicated for deep impacted cases
Advantages:
- Better control of the direction of traction force
Disadvantages:
- Esthetics depend on the amount of attached gingiva
advantages vs. disadvantages of opened with full flap technique
open window
which surgical technique is indicated for not deeply displaced (removal of thick palatal mucosa, bone, and follicle down to CEJ
Advantages:
- Autonomous eruption
- No traction needed
Disadvantages:
- Poor periodontium due to excessive removal of bone and tissue down to the CEJ
- Regrowth of palatal tissue
advantages vs. disadvantages of open window
Tunnel technique
What surgical technique?
Traction of the impacted tooth downward through the socket of extracted deciduous canine. Elevation of all soft tissue layers including periosteum, exposing the underlying bone
- Increased pain
- Excessive tissue removal
- Improper healing
- Damage to the periodontal attachment
- Damage to tissues and/or teeth from bonding agents
What are potential risks during surgical exposure of Palatally Impacted Canines? (5)
cantilever system
temporary anchorage devices (TADs)
double-archwire mechanics
3 ortho techniques to treat + manage impacted max canines
Cantilever system
What orthodontic technique to treat and manage impacted maxillary canines?
Advantages:
- Predictable tooth movement
- Low load or deflection
- Less frequent reactivations
Disadvantages:
- Potential side effects should be identified on the anchor tooth
Temporary anchorage devices (TADs)
What orthodontic technique to treat and manage impacted maxillary canines?
Advantages:
- Could provide absolute anchorage for tooth movement
- Bonding of orthodontic brackets can be delayed until the canine is aligned
Disadvantages:
- Does not produce root movement
- Insertion and removal TADs
Double-archwire mechanics
What orthodontic technique to treat and manage impacted maxillary canines?
Advantages:
- Minimizes root resorption of the lateral incisors
- Allows horizontal tooth movement
Disadvantages:
- Insertion and removal of TADs
- Requires laboratory procedure
- Patient discomfort
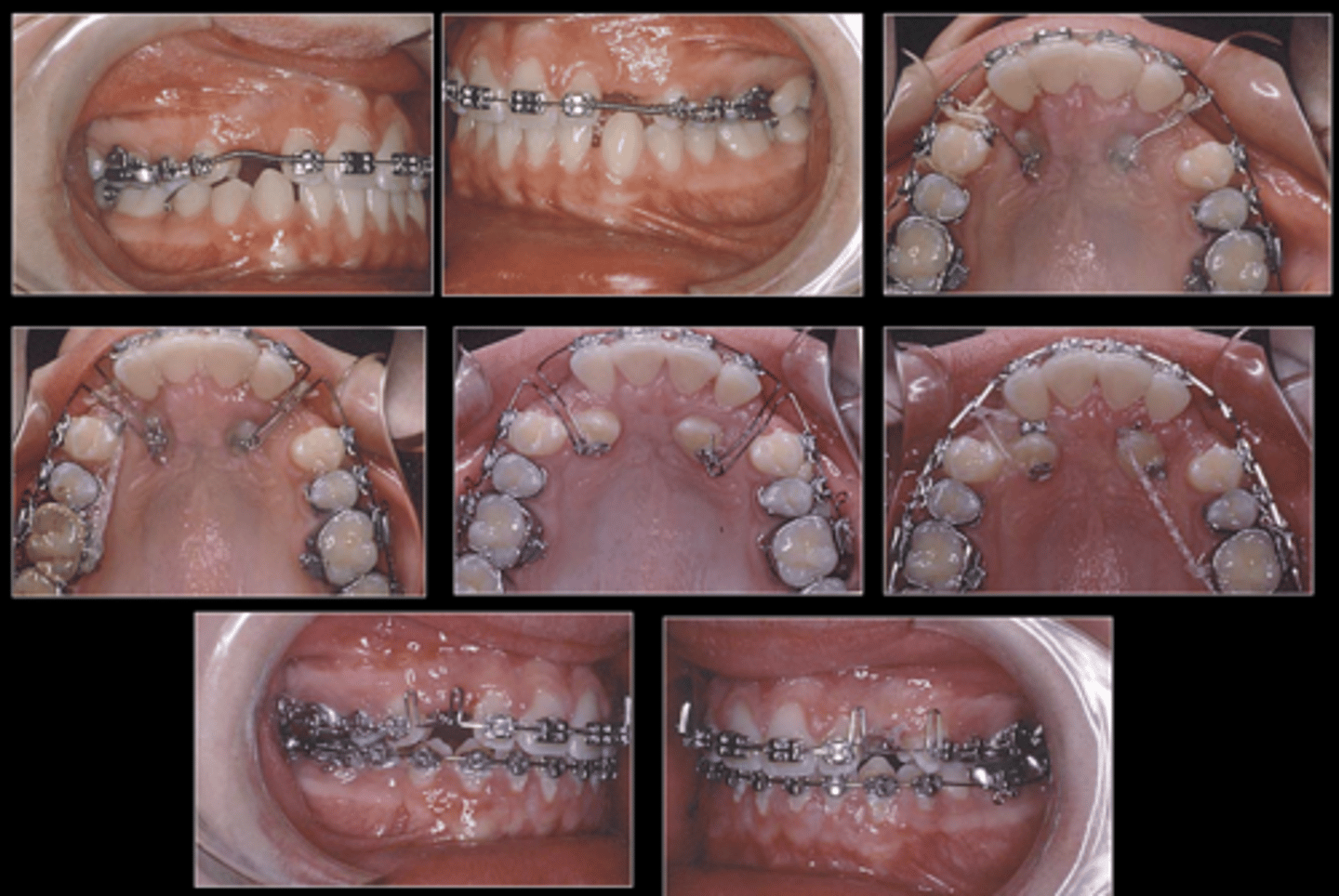
Ballista spring (allows tooth to move in three directions: occlusal, labial, distal)
This shows treatment of a maxillary impacted canine with what type of spring?
closed
open w/ apically positioned flap
gingivectomy
3 surgical techniques used to expose labially impacted canines
Closed
Which surgical technique to expose a labially impacted canine?
- Indications: Deep impacted cases, devicated from the normal position
Advantages:
- Less aggressive
- Less vertical relapse
- Less scar
- Better esthetic outcomes
Disadvantages:
- Tooth is invisible
- Orthodontic force cannot be controlled during traction
- Re-open if attachment/chain breaks
- Patient discomfort
advantages vs. disadvantages of closed technique for labially impacted canines
Open with apically positioned flap
Which surgical technique to expose a labially impacted canine?
Indications:
- Displaced above the level of the MGJ
- Either deeply impacted nor angulated proximally
Advantages:
- Preserve the keratinized tissue
- Controlled traction force direction
Disadvantages:
- Crown instability and re-intrusion of the tooth after Ortho. Tx
advantages vs. disadvantages of open w/ apically positioned flap technique for labially impacted canines
Gingivectomy
Which surgical technique to expose a labially impacted canine?
Indications:
- Palpable crown beneath attached gingiva
- Band of attached gingiva within which the incision is made, leaving a portion of the thicker tissue above the cut
Advantages:
- Easy procedure, no bone removal involved
Disadvantages:
- Clinical Attachment Loss (CAL)
- Gingival recession
advantages vs. disadvantages of gingivectomy technique for labially impacted canines
Gingivectomy
What surgical technique is recommended?
- Canine cusp is coronal to the mucogingival junction (MGJ)
Apically positioned flap
What surgical technique is recommended?
- Canine cusp is apical to the mucogingival junction (MGJ)
Closed eruption technique
What surgical technique is recommended?
- Canine cusp is significantly apical to the mucogingival junction (MGJ)
Tunnel technique
what surgical technique is used to expose midalveolar impacted canines
- Erupts the canine down through the evacuated socket of the extracted deciduous canine
- The labial part of the socket wall intact, proper attached gingiva and excellent esthetic results
describe the Tunnel technique
Damage to adjacent teeth
Improper healing
What are 2 treatment risks of surgery for impacted cuspids?
Damage to adjacent tissues and teeth with acid etch
Improper placement of attachment
Detachment of bracket
What are 3 treatment risks of bonding for impacted cuspids?
Deficient attached gingiva especially with labial cuspids
Gingival recession
Poor esthetics
Relapse
What are 4 treatment risks for the periodontium for impacted cuspids?
Greater, lower
An adequate zone of attached gingiva is thought to be associated with _______ ability to withstand gingival inflammation and _______ risk for developing gingival recession, while a healthy periodontium has been proposed as a key indicator of treatment success for impacted teeth
Rapid Palatal Expanders (RPE)
In children, how can you make space to allow a cuspid to erupt on its own?
For adult patients, the impacted tooth has lost its inherent eruption drive, so even if enough space is created for the impacted canine, the tooth does not erupt by itself and requires traction.
- An apically positioned flap is more predictable to increase the keratinized tissue width if there is insufficient gingiva (covering the CEJ and 2-3mm of the crown)
In adults, how can you allow a cuspid to erupt on its own?
1. Location of the impacted tooth and the distance it must travel
2. Extent of the surgical procedure required
3. Angulation of the impacted canine
4. Amount of available space in the dental arch
5. Age of the patient
6. Condition of the adjacent teeth
7. Light forces
8. The initial direction of force should be away from the roots of adjacent teeth
What are the 8 clinical considerations for impacted canines?
Light, away
When orthodontic traction is indicated, _______ forces should be used, and the initial force vector should direct the canine _______ from the roots of neighboring teeth to reduce the risk of root resorption and other complications