MGY378 27: oncolytic viruses (OV)
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
first OV approved for head and neck cancers
adenovirus, 1960s China
OV principles
target and destroy tumour cells w/o damaging healthy cells
direct lysing
activation of imm sys against tumour
unarmed: virus without added genes
armed: with added genes
engineered to deliver cytokines, antibodies, or other factors that are antitumour/ affect immunosuppressive tumour env
target tumour independent of TAA expression patterns - target tumour directly
antitumour effects
enhancing immunogenic cancer cell death
thru mutation of key genes in virus to make it replicate better in cancer cell
enhancing TC effector activity
for presentation of TAAs so imm sys can recognise it
enhancing APC functions
So TC come and destroy virus-infected cancer cell
reversing TC exhaustion
production of anti-TC exhaustion cytokines
immune response against cancer
ROS
from ER/ genotoxic stress
TAA uptake
CTL
NK cell
antiviral vs antitumour immunity
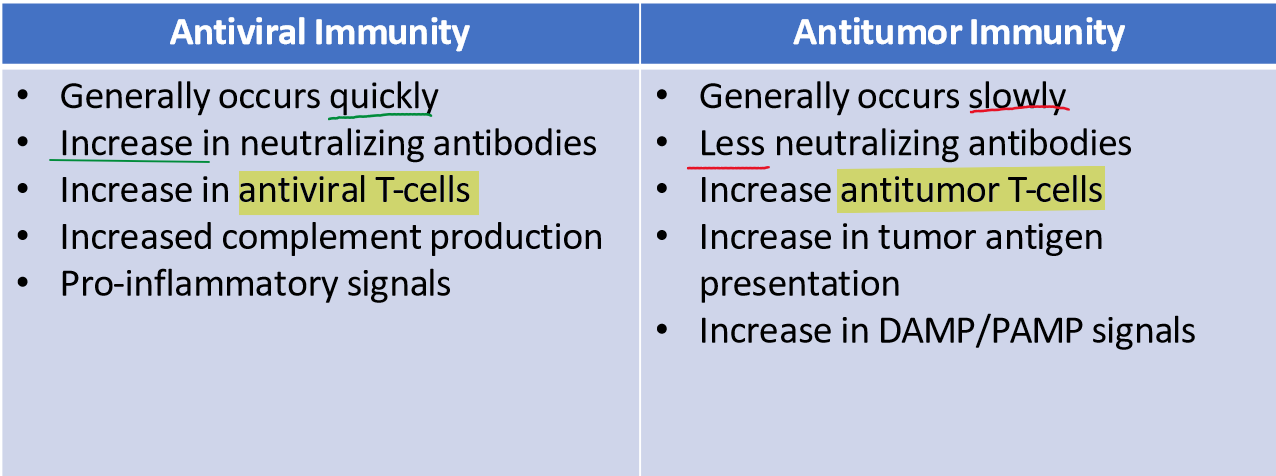
why is antitumour immunity slower than antiviral immunity?
cancer progresses slower
problems with imm resp and OVs
the virus is still a virus - imm sys can mount a response and get rid of it -- challenge
cannot repeat the dose - limits efficacy
delivery: trying to deliver tumour in a specific area
ex: gliablastoma. BBB poses a challenge to viral delivery there
u want a virus that can induce an imm response and kill tumour cells but it has to be attenuated
H101
adenoV OV
nasopharyngeal carcinoma
combo w/ chemo
ECHO-7
echovirus OV
unresectable stage IIIB-IV melanoma
teserpaturev
HSV1 OV
glioblastoma
following radiotherapy and temozolomide
nadofaragene firadenovec
adenoV OV
non-muscle invasive bladder cancer
T-Vec
HSV1 OV
recurrent melanoma
unresectable cutaneous & subcutaneous nodal lesions
local treatment
deleted y34.5 virulence gene → loss of ICP34.5
deleted US12 gene
eng to expr GM-CSF
Loss of ICP34.5 in T-vec
In HSV infection, the host cell response w antivirals to shut off translation (p-lates eIF2a)
ICP34 can overcome this by activating the phosphatase to remove the P from eIF2a so the virus can keep translating
solution = get rid of ICP34
Cannot replicate in healthy cells, which have intact eIF2α pathways.
Can replicate in tumour cells, which often lack proper antiviral signaling (e.g., dysfunctional PKR pathway).
Loss of US12 in T-vec
gene that blocks peptide presentation to MHC I so the virus doesn't show itself to imm sys
knock it out so viral ag and TAAs are both shown better to the imm sys > viral-infected tumour cells get killed
GM-CSF in T-vec
recruits antitumour immune cells
T-vec stats
if body has seen oncolytic virus before it will mount a response
works for both sero-ve and +ve, but sero+ve = more side effects
58% reduction compared to GM-CSF only (standard care)
melanoma makes it so u can inject virus directly into site of tumour
combo w/ PDL-1 inhibitor = checkpoint blockade → antitumour
RNA OVs
RNA viruses kill tumours faster
replicate in cytoplasm
but less tumour selective
immune sys must clear in healthy cells
enveloped viruses as OVs
less oncolytic
more likely to be cleared by imm resp before showing activity
virus size for OV
smaller viruses can diffuse thru tumour better
but larger viruses have more transgene carrying capacity
ONYX-015 OV
adenoV OV
deleted E1B55kd gene
cannot degrade p53 → replicates better in p53-deficient cells (tumour cells)
for head and neck cancers
added genes for cytokine delivery
GM-CSF
IFN
IL12
IL2
added genes for TAA presentation to imm sys
CEA
PSA
added immune checkpoint inhibitors
PDL-1
CTLA-4
added tumour suppressor genes
p53
added anti-angiogenesis component
anti-VEGF antibody
VSV & Newcastle Disease virus as OVs
animal viruses, rare pre-existing immunity
inducer of IFNs
safe
apoptosis/ necrosis of infected (tumour) cells release TAAs → antitumour TC activations
ARV-PB1
avian orthoreovirus
non-enveloped, dsRNA
10 segment genome
low pre-existing immunity (distinct from human orthoreoviruses)
syncytia formation (CPE) in infected (tumour) cells
ARV-PB1 gene segments:
S1
M1
L1
from avian orthoreoviruses:
S1: strain 128
M1: GX110058
L1: strain AVS-B
ARV-PB1 stats
lot of replication in cancer cell lines → spreads to other cells
expression of ISGs
causes apoptosis of infected (tumour) cells
injection didn’t kill healthy mice
no pathology in healthy hepatocytes
limitations of OVs
poor efficacy against solid tumours
physical barriers
poor vascular/ lymphatic access may limit delivery
pre-existing immunity
solid tumours secrete immunosuppressive TGF-beta and IL10 → reduce immune cell recruitment
solutions to limitations
prime-boost with different OVs to avoid nAbs against virus
combo with radiation/ chemo → solid tumour becomes more permeable to OV
can combo with surgical resection too
local delivery to solid tumours
combo T-vec & anti-PD1
for surgically unresectable stage IIIB and IV melanoma
response rate 68%
no dose-limiting toxicity
combo T-vec & anti-CTLA4
for stage IIIB and IV melanoma
combo therapy = 39% response rate
OV alone = 18%