L4: ABI Recovery & Neurologic Treatment Approaches
1/124
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
125 Terms
Recovery definition at ICF health condition level
Restoring function in neural tissue that was initially lost after injury
(may be seen as reactivation in brain areas previously inactivated)
Recovery definition at ICF body function/structure level
Restoring the ability to perform a movement in the same manner as it was performed before injury
Recovery definition at ICF activity level
Successful task accomplishment using limbs or end effectors typically used by nondisabled individuals
Compensation definition at ICF health condition level
Neural tissue acquires a function that it did not have prior to injury
Compensation definition at ICF body function/structure level
Performing an old movement in a new manner
Compensation definition at ICF activity level
Successful task accomplishment using alternate limbs or end effector
(opening chips with 1 hand and mouth)
Motor recovery definition
“Getting better”
Improvement in the strength, speed, or accuracy of arm and leg movements
Functional recovery definition
“Doing better”
Improvements in performance
Motor recovery assessments
MMT
ROM
Observational movement analysis
Coordination
9 hole peg test
Modified Ashworth Scale
Functional recovery assessments
Patient reports outcome measures
Stroke impact scale
10 MWT
6 MWT
Goal attainment scale
TUG
5x STS
AM-PAC (6 clicks)
Functional impairment measures
Every person will have a ________ recovery journey after ABI
Unique
Recovery after ABI depends on
Injury
Location
Timing (neuroplasticity)
Size
PLOF
Cognition
Compliance
Social determinants of health
Ability to access quality rehabilitation
Motor recovery concepts - deficit severity post stroke
Mild UE deficits = greater potential for full or near full recovery
Significant UE deficits = more variable trajectory
Stroke recovery timeline
0-24 hours = Hyperacute phase
1-7 days = Acute phase
1 week - 3 months = Early subacute
3-6 months = Late subacute
> 6 months = Chronic
When do the most significant motor improvements happen in stroke recovery?
During the first couple of weeks
What happens during the Hyperacute phase?
Spontaneous neurological recovery
Plasticity enhancing mechanisms lead to neuroplastic changes in the brain
New synapses, axonal sprouting, & dendritic growth
Will continue into subacute phase
Interhemispheric connectivity in the hyperacute phase initially ________?
Decreases
Connectivity drops significantly during first 2 weeks
Gradually recovers & parallels spontaenous motor recovery
What happens during the Acute phase?
Spontaneous neurological recovery continues
Neuroplastic changes and motor recovery are enhanced by specific, intensive rehabilitation
Sitting EOB
Bed mobility
Transfer training
Motor recovery is most rapid during the first ________ post-insult
3-6 months
On average, people will recover ________ previous function
70%
What happens for Physiologic Recovery during the Subacute phase?
Axonal sprouting, synaptogenesis, dendritic spine expansion
Synaptic effectiveness
Reperfusion
Diaschisis reversal
What happens for Motor Recovery during the Subacute phase?
Recovery shaped by experience
Focused on impairments to target deviations
Task-oriented
Specific
Axonal sprouting
New axons start growing
Synaptogenesis
New connections are made between previously unconnected areas
Dendritic spine expansion
Dendrites lengthen to connect to new, more remote areas
Synaptic effectiveness
Resolution of local edema
May continue for up to 8 weeks
Reperfusion
Return of adequate blood supply may lead to resumption of neural activity
Arteriolar collateral growth and new capillaries form in ischemic border (Penumbra)
Diaschisis
Loss of function within a region distant to the site of the lesion and results from deafferentation of neurons as a result of axon damage caused by stroke
The more severe the insult, the ________ and more severe diaschisis
Longer
Diaschisis commonly presents as neurological signs including
Impaired consciousness
Cognitive impairments, including dementia
Dyspraxias, dystaxias, dysphasias
Incoordination
Sensory neglect
(all require talking across cortices)
Recovery of function from diaschisis is associated with recovery of ________ & ________
Local perfusion, Metabolism
Diaschisis reversal may be related to ________
Resolution of edema
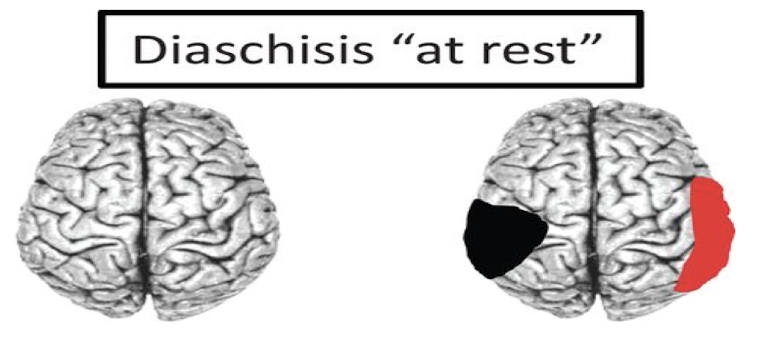
Diaschisis at rest
Focal lesion induces a remote reduction of metabolism (red)
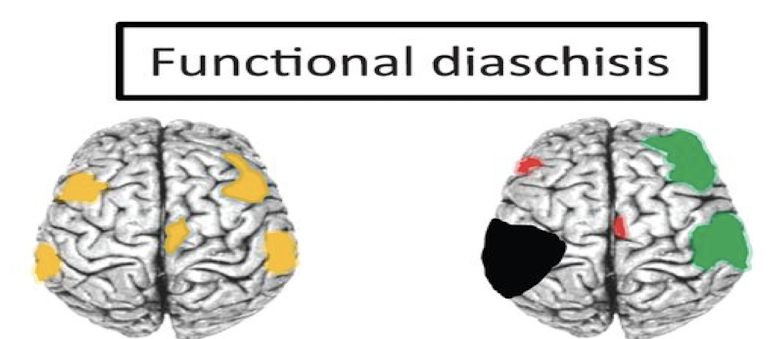
Functional diaschisis
Normal brain activations (yellow) during a selected task may be altered, either increased (green) or decreased (red) after a lesion
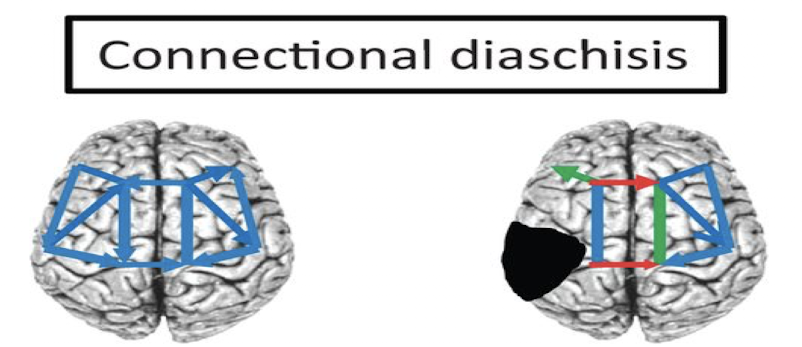
Connectional diaschisis
Distant strengths and directions of connections in a selected network may be increased (green) or decreased (red)
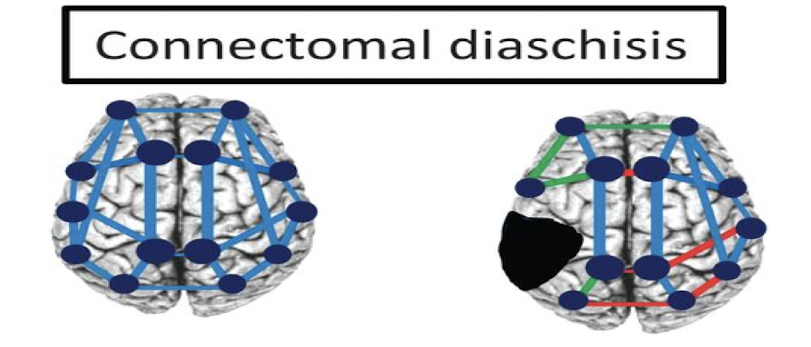
Connectomal diaschisis
Lesion of the connectome includes widespread changes in brain network organization including decrease (red) or increase (green) in connectivity
Post stroke patients exhibit more ________ functional connectivity than healthy controls
Complex
Impacted by compensatory mechanisms, new connections, & overall efforts to restore functionality
________ functional connectivity is associated with better motor recovery
Interhemispheric
Specifically connections between motor areas (M1 → M1) & primary motor area to the supplementary motor area of the unaffected hemisphere (M1 → SMA)
Cognitive recovery is associated more with ________
Default mode networks
Large scale brain network primarily active when an individual is not focused on the external environment
What happens during the Subacute to Chronic phase
Cortical reorganization
Maintenance
Cortical reorganization definition
Use dependent changes in cortical maps/ representations
Three ways cortical reorganization can happen?
Increase in the absolute number and concentration of synapses on dendrites
Unmasking of latent neural networks
Surviving neurons reorganize connectivity patterns to support partial restoration or compensatory substitution for lost function (occurs in bilateral hemispheres)
Ranchos Los Amigos level I
Outcome:
No response
Patient Response:
No response to sounds, sights, touch, or movement
Ranchos Los Amigos level II
Outcome:
Generalized response
Patient Response:
Limited response, which is inconsistent and nonpurposeful
Response to sounds, sights, touch, or movement
Ranchos Los Amigos level III
Outcome:
Localized response
Patient Response:
Inconsistent but purposeful response in a more specific manner to stimuli
May follow simple commands
Ranchos Los Amigos level IV
Outcome:
Confused & agitated
Patient Response:
Confused and often frightened
Overreactions to stimuli by hitting or screaming
Highly focused on basic needs (eating, toileting)
Difficulty following directions
Ranchos Los Amigos level V
Outcome:
Confused & inappropriate
Patient Response:
Appears alert and responds to commands
Easily distracted by the environment
Frustrated and verbally inappropriate
Focused on basic needs
Ranchos Los Amigos level VI
Outcome:
Confused & appropriate
Patient Response:
Follows simple directions consistently
May have some memory but lacks details
Attention span of about 30 minutes
Ranchos Los Amigos level VII
Outcome:
Automatic & appropriate
Patient Response:
Follows a set schedule
Does routine self-care without help
Attention difficulty in distracting or stressful situations
Problems in planning and following through
Ranchos Los Amigos level VIII
Outcome:
Purposeful & automatic
Patient Response:
Realizes difficulties with thinking and memory
Less rigid and more flexible thinking
Able to learn new things
Demonstrates poor judgement
May need guidance on decisions
Recovery after mild TBI (concussion)
For most people, symptoms resolve within 1 month
If symptoms persist longer than 6 weeks, refer to neurology
What is post concussion syndrome (PCS)?
Lingering symptoms following a concussion or mild traumatic brain injury
Symptoms may last weeks, months, or occasionally a year or more
Most common symptoms of mild TBI
Poor concentration - 71%
Irritability - 66%
Fatigue - 64%
Depression - 63%
Memory problems - 59%
Headaches - 59%
Anxiety - 58%
Trouble thinking - 57%
Dizziness - 52%
Blurry or double vision - 45%
Sensitivity to bright light - 40%
Mild TBI returning to play protocol Step 1
Back to regular activities
Mild TBI returning to play protocol Step 2
Light aerobic exercise (5-10 minute walk/ light jog)
Mild TBI returning to play protocol Step 3
Moderate activity (submax lifting, jog/run/bike)
Mild TBI returning to play protocol Step 4
Heavy, non-contact activity (weight lifting)
Mild TBI returning to play protocol Step 5
Practice and full contact
Mild TBI returning to play protocol Step 6
Competition
Patients must spend a minimum of ________ at each level
24 hours
T/F: Patients can move to the next step after 24 hours but with a return of symptoms
FALSE!
(ONLY move to next step if no return of symptoms/ new symptoms)
Functional outcomes over first year after moderate/severe TBI
Approximately ½ of those with severe TBI & ¾ of those with moderate TBI recovered the ability to function independently at home for at least 8 hours per day
Glascow Outcome Scale - Extended
8 levels
Minimum score = 1 (death)
Maximum score = 8 (resumption of normal activity without disability)
12 months post severe TBI ________ of patients scored an 8 and ________ of patients scored a 7
25%, 16%
T/F: If a patient discharges from the hospital, the chance of dying increases significantly
FALSE
(38% chance prior/ at discharge and 39% chance at 1 year)
Explain the neural plasticity principle of use it or lose it.
Failure to drive specific brain functions can lead to functional degradation
Explain the neural plasticity principle of use it and improve it.
Training that drives a specific brain function can lead to an enhancement of that function
Explain the neural plasticity principle of specificity
The nature of the training experience dictates the nature of the plasticity
Explain the neural plasticity principle of repetition matters.
Induction of plasticity requires sufficient repetition
Explain the neural plasticity principle of intensity matters.
Induction of plasticity requires sufficient training intensity
Explain the neural plasticity principle of time matters.
Different forms of plasticity occur at different times during training
Explain the neural plasticity principle of salience matters.
The training experience must be sufficiently salient to induce plasticity
Explain the neural plasticity principle of age matters.
Training induced plasticity occurs more readily in younger brains
Explain the neural plasticity principle of transference.
Plasticity in response to one training can enhance the acquisition of similar behaviors
Explain the neural plasticity principle of interference.
Plasticity in response to one experience can interfere with the acquisition of other behaviors
Good evidence for improving walking function in chronic CVA & TBI
Clinicians should perform:
Walking training at moderate to high aerobic intensities
Walking training with virtual reality
Moderate evidence for improving walking function in chronic CVA & TBI
Clinicians may consider:
Strength training at ≥ 70% 1RM
Circuit training, cycling, or recumbent stepping at 75-85% of HRmax
Balance training with virtual reality
Poor evidence for improving walking function in chronic CVA & TBI
Clinicians should not perform:
Static or dynamic balance activities including pre-gait
BWSTT with emphasis on kinematics
Robot assisted gait training
To improve walking function in chronic CVA/TBI
Train at moderate to high intensity
Virtual reality makes it salient
Why might calculating HRmax using HR reserve be better after CVA?
It accounts for variations in resting HR
HR reserve equation
HRR = HRmax - HRresting
Description of muscle re-education
Improve strength for injuries that affect LMN
Foundation of MMT
Focus on isolated muscle strengthening & stretching
Strengthening is ________ for patients with neurologic disorders
VITAL
Strengthening ________ exacerbate disease process or ________ spasticity if implemented correctly
Will not, Worsen
Muscle re-education limitations
Increasing strength/ROM ≠ change in movement pattern
Neurofacilitation Approach description
Application of appropriate sensory inputs = normal movement patterns
Built on reflex theory and hierarchical organization of reflexive development
Focus on progression through stages of recovery/ motor control using sensory facilitation
Neurofacilitation current use
Fugl-Meyer Motor Assessment of Motor Recovery outcome measure
Postural control
Progression of task difficulty
Application of sensory cueing
Neurofacilitation limitations
Voluntary movement is not entirely reflexive in nature
Brunnstrom Stage 1
Flaccid paralysis
Brunnstrom Stage 2
Development of minimal movement in synergies (some spasticity)
Brunnstrom Stage 3
Voluntary movement synergy dependent (marked spasticity)
Brunnstrom Stage 4
Some movements out of synergy (less spastic)
Brunnstrom Stage 5
Movements almost independent of synergy
Brunnstrom Stage 6
Normal movement with normal speed
Treatment during Brunnstrom Stage 1
PROM
Positioning
Weight bearing through UE
Hand-over-hand assistance
Treatment during Brunnstrom Stage 2
Sensory re-education
AAROM/ reduced friction/ gravity eliminated
Mirror therapy
More weight bearing
Treatment during Brunnstrom Stage 3
Mirror therapy
Spliniting
Functional movements
Task specific
High intensity
Salient
Treatment during Brunnstrom Stages 4 & 5
Functional movements
Constraint induced movement therapy
Strengthening
Treatment during Brunnstrom Stage 6
Functional activities & participation with progressing complexity
Dual tasking
Proprioceptive Neuromuscular Facilitation (PNF) description
Use of diagonal movement patterns to promote functional recovery
Focus on use of sensory inputs to elicit compound muscle activation in diagonal planes